
Abstract

T
The review covers the journey of the laparoscopic liver resection (LLR) since the first reported case in 1991, through the two consensus conferences held, respectively, in Louisville Kentucky, United States, in 1998 and in Morioka, Japan, in 2014 and provides comprehensive insight into the current status of the LLR focusing on hot topics such as robotic LR, major LLR, LLR for living-related liver transplantation, and laparoscopic associating liver partitioning and portal vein Ligation for staged hepatectomy (ALPPS).
Interestingly, the results of this study are presented in different sections.
(1) Oncological indication to LLR: More and more articles are documenting malignancy as primary indication to LLR with mortality <1%, significantly less complications, transfusions, blood loss, and hospital stay when compared with open LR, and cumulative overall long-term survivals not different in the two groups.
(2) Safety and learning curve on major LLRs and LLRs for lesions with “difficult location”: Increased difficulty in LLRs for the removal of three or more segments or for the resection of lesions located in the caudate lobe, or posteriorly or centrally into the liver, is well documented. Although feasibility of these LLRs has been documented, it appears clear that majority of those challenging cases are performed in selected high-volume centers, and surgeons should approach LLRs for those types of cases after at least a learning curve of 60 minor or anteriorly located lesions.
(3) Robotic assisted LR: Robotic assisted LR using the da Vinci system is being reported as a tool to overcome some ergonomic and visual problems of the laparoscopic approach; however, few groups are consistently dedicated to it and cost and learning curve remain an important problem.
(4) Laparoscopy and living donor liver transplantation: It has been documented that left lateral sectionectomy, for adult to child liver transplantation, provides graft with excellent outcome for the recipient and less wound morbidity and faster recovery for the donor. In the adult counterpart, although the feasibility of both left and right hemihepatectomy has been reported, we are far from the possibility of considering it as a standard of practice; in this scenario, donor safety being the paramount concern. 2
(5) Laparoscopy and ALPPS: The rationale of using minimally invasive procedures to diminish the already high rate of morbidity in this two-step challenging procedure seems to be fascinating but needs much more literature background to be considered a valuable option.
LLRs performed each year are increasing and so the number of scientific publications and of the scientific societies related to this field of medicine; in this regard, I would like to mention the Italian experience of the Italian Group of Minimally Invasive Liver Surgery “I GO MILS,” which develops and reports all the activity related to LLR in the country. Our unit is part of the I GO MILS project, and we as well as others in Italy have being performing an increased number LLRs per year (Fig. 1).3,4
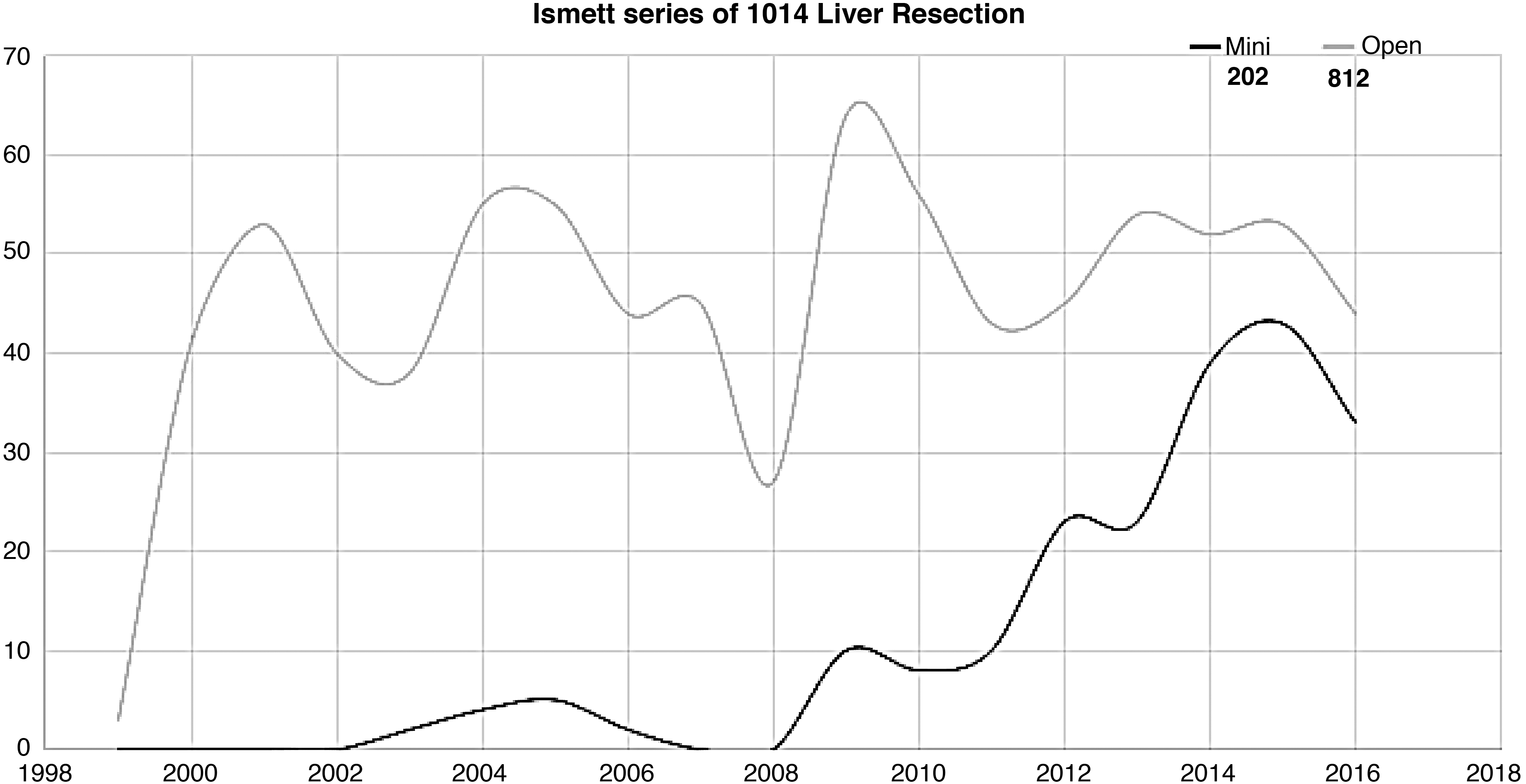
ISMETT liver resection series. ISMETT, Istituto Mediterraneo per i Trapianti e Terapie ad Alta Specializzazione.
Over a period of a few decades, laparoscopic surgery has changed the surgical thinking, shifting toward diminishing invasiveness even in areas such as liver surgery, in which traditionally invasiveness pervaded the majority of surgical strategies.
Still two major points need to be better addressed: lack of prospective randomized controlled clinical trials comparing LLRs with open LR and how to face the learning curve and the reproducibility of these challenging operations.
In this setting, the review by Geller and his associates helps in finding answers provided by a methodologically correct search of the literature.
Footnotes
Disclosure Statement
Nothing to disclose.