
Abstract
Abstract
Background:
Adequate pain control is a major concern in the immediate postoperative period. In multiple strategies for postoperative pain management, topical analgesics have significant advantages of minimizing severe side effects caused by oral and parenteral administration and drug–drug interactions. Therefore, we studied the effect of lidocaine patch on postoperative pain control in laparoscopic appendectomy.
Patients and Methods:
This randomized double-blind prospective controlled study enrolled 40 acute appendicitis cases that were treated by laparoscopic appendectomy and randomly divided into two groups. Lidocaine patches containing lidocaine 175 mg was applied to the umbilical trocar site of each patient, and pain intensity was assessed with the visual analog scale every 6 hours up to 48 hours after laparoscopic appendectomy.
Results:
There was no significant difference in age, gender, body mass index, the American society of anesthesiologists score, comorbidity, or underlying disease between the lidocaine patch and control groups. The postoperative pain scores were lower in the lidocaine patch group than in the control group, but statistical significance was not noted at the trocar site or the right lower quadrant of the abdomen (P = .320 and P = .903, respectively). The mean amounts of pethidine used after surgery were significantly smaller in the lidocaine patch group than in the control group (0.10 ± 0.31 mg versus 0.25 ± 0.79 mg, P < .001).
Conclusions:
The results of this study suggest that lidocaine patch application to the trocar site after laparoscopic appendectomy may have a positive effect on the management of postoperative pain and can eliminate the need to inject additional analgesics for further postoperative pain control.
Introduction
L
Postoperative pain has been mainly controlled using systemic or topical analgesic administration. Systemic administration of analgesics is the primary option for pain control after surgery, but can cause nausea, vomiting, impaired intestinal movement, and abdominal discomfort. However, topical administration of anesthetics can reduce the incidence of side effects of anesthetics by acting directly at the surgical site and by minimizing drug–drug interactions. 3 There have been numerous studies reporting that topical use of anesthetics has a positive effect on alleviation of postoperative pain.4–8 In addition, several studies have demonstrated that the topical lidocaine patch is effective in managing postoperative pain in patients undergoing laparoscopic ventral hernia repair or gynecologic laparoscopic surgery.9,10
Therefore, we studied the effects of the lidocaine patch 5% (Lidoderm®; Endo Pharmaceuticals, Inc., Chadds Ford, CA) on pain control in patients undergoing laparoscopic appendectomy.
Patients and Methods
This randomized, double-blind, prospective, controlled study enrolled 40 patients who were diagnosed with acute appendicitis and underwent laparoscopic appendectomy at the Department of Surgery, Konkuk University Chungju Hospital between March 2016 and February 2017. We excluded patients who (1) received topical anesthetics or nonsteroidal anti-inflammatory drugs (NSAIDs), (2) ingested analgesics on a regular basis, or (3) had chronic painful conditions or neurological impairment. This study was approved by the Institutional Review Board (IRB) of Konkuk University Chungju Hospital (KUCH 2016-03-015). Informed consent was given by each patient after complete description of the study protocol. Forty patients who underwent laparoscopic appendectomy were randomized into two groups immediately after surgery by an IRB moderator who was blinded to the study using block randomization with blocks of four: the lidocaine patch and control groups (1:1 ratio, 20 patients in each group). All the surgical procedures were performed by a single surgeon using the three-trocar technique with one 10-mm umbilical port and two additional 5-mm trocars in the right iliac fossa and the suprapubic area. General anesthesia was performed by the same anesthesiologist. No premedication was used. General anesthesia was induced with propofol (2 mg/kg), fentanyl (2 g/kg), or thiopental sodium (5 mg/kg), and tracheal intubation was facilitated with vecuronium bromide (0.6 mg/kg). Sevoflurane and oxygen were used for the maintenance of anesthesia, and additional vecuronium bromide (0.6 mg/kg) was administered to maintain an adequate level of muscle relaxation. In the lidocaine patch group, a lidocaine patch containing lidocaine 175 mg was applied to each side of the umbilical trocar site, which was changed every 12 hours up to 48 hours after surgery. In the control group, indistinguishable patches with the same shape and nature were applied in the same way. The following data were collected from each patient: demographic data, body mass index (BMI), the American Society of Anesthesiologists (ASA) score, operation time, anesthesia time, hospitalization day, and laboratory test results. Pain intensity was assessed using visual analog scale (VAS) scores at 0, 6, 12, 18, 24, 30, 36, and 48 hours after surgery. The following side effects probably due to lidocaine were evaluated: nausea, vomiting, erythema, rash, contact dermatitis, hypotension, bradycardia, cardiovascular instability, headache, and dizziness. Additional pain control was performed using pethidine injection (25 mg).
Statistical analyses
Statistical Analyses were performed using the IBM SPSS software (version 21; IBM Corp., Armonk, NY) and the MedCalc for Windows version 14.8 (MedCalc software, Ostend, Belgium). All data were entered into and reviewed using Microsoft Excel (Microsoft, Redmond, WA). Continuous variables were tested for normality using the Kolmogorov–Smirnov test. Continuous variables showing normality were analyzed using the Student's t test, paired t test, analysis of variance, and two-way analysis of variance, followed by the post hoc test. Data are expressed as the arithmetic mean ± standard deviation (SD). Continuous variables not showing normality were analyzed using the Mann–Whitney U test and are expressed as the median (25–75 interquartiles). Categorical variables are displayed as frequency distributions and were evaluated with Pearson's Chi-square test or Fisher's exact test. Statistical significance was accepted at the 5% level (P < .05). Univariate comparisons between the groups for categorical variables were made using the chi-square test and Fisher's exact test as appropriate. Multiple logistic regression analysis using backward stepwise regression was performed. Variables with a level of significance defined as P < .20 for univariate logistic regression analysis, as well as clinically important variables, were entered as candidate variables in the multivariate models to assess their viability as independent predictors for postoperative pain scores. The results were reported as odds ratios with 95% confidence intervals (CI) and relevant P values.
Results
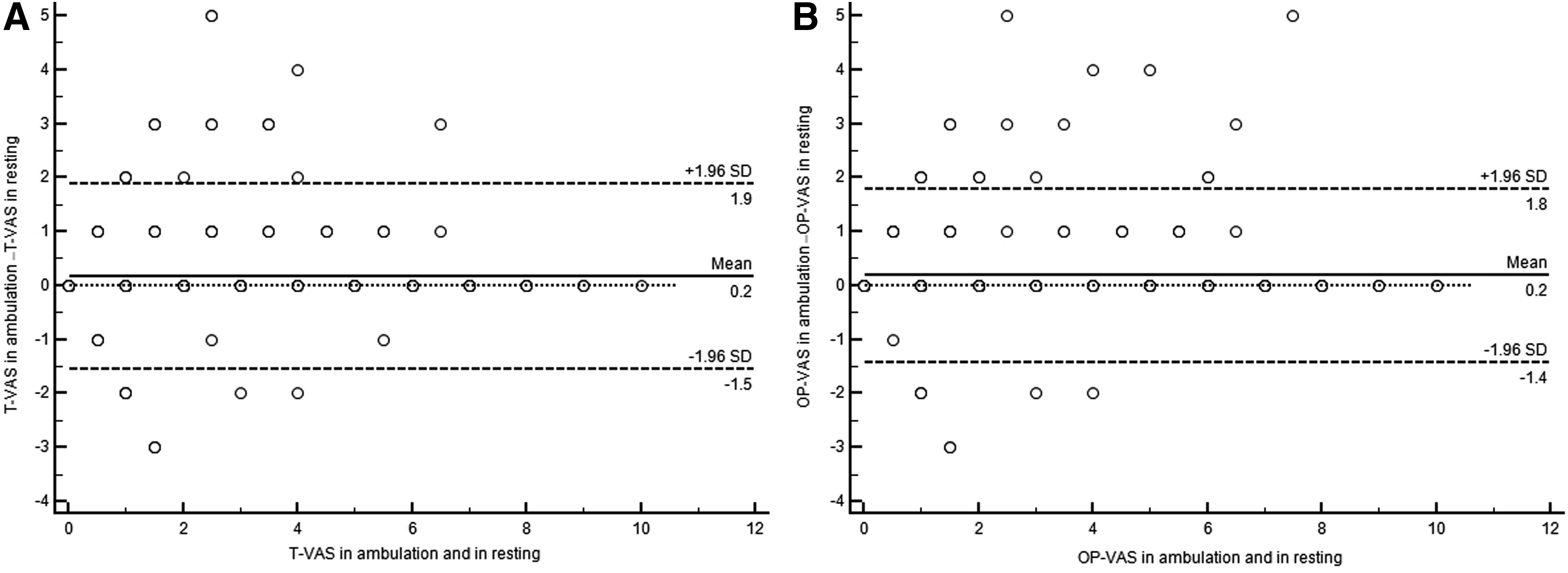
The mean age of the patients was 34.88 ± 15.29 years (range, 19.0–77.0 years), and there were 27 males and 13 females. The mean BMI of the patients was 23.8 ± 4.20 (range, 17.3–37.2). There was no significant difference in age, gender, BMI, the ASA score, or the incidence of diabetes/hypertension between the lidocaine patch and control groups. There were various types of acute appendicitis: focal (n = 1), suppurative (n = 34), and gangrenous (n = 5) types. There was no significant difference in the mean operation time (41.88 ± 14.26 minutes), mean anesthesia time (66.88 ± 15.88 minutes), or mean hospitalization day (4.10 ± 0.81 days) between the two groups. Table 1 shows the demographic characteristics of the patients. There was no significant difference in the VAS scores at the umbilical trocar site, right lower quadrant of the abdomen, or shoulder area between the two groups (Table 2). The VAS scores at the umbilical trocar site at rest and ambulation were lower in the lidocaine patch group than in the control group and tended to decrease over time, although the difference was not statistically significant (P = .320 and P = .398, respectively) (Fig. 1A, B). The VAS scores at the right lower quadrant of the abdomen at rest and ambulation were similar between the lidocaine patch and control groups, and tended to decrease over time, without significant differences (P = .931 and P = .903, respectively) (Fig. 1C, D). The VAS scores at the shoulder and all the other areas at rest and ambulation were lower in the lidocaine patch group than in the control group, although the difference was not statistically significant (P = .606). The mean amounts of pethidine used after surgery were 0.10 ± 0.31 mg in the lidocaine patch group and 0.25 ± 0.79 mg in the control group, and the difference was statistically significant (P < .001) (Table 2). None of the patients showed nausea, vomiting, erythema, rash, contact dermatitis, hypotension, bradycardia, cardiovascular instability, headache, or dizziness. The Bland–Altman technique was used to access accuracy, precision, relationship between the differences, magnitude of paired measurements, and degree of agreement between the postoperative VAS scores at rest and ambulation in the umbilical trocar site and the right lower quadrant of the abdomen (Fig. 2A, B). Neither accuracy nor the positive relationship between the postoperative VAS scores at rest and ambulation was statistically significant (umbilical trocar site: differences in arithmetic mean 0.1656, 95% CI −0.2615 to −0.06979, P = .0008, SD = 0.8714, lower limit = −1.8735, lower limit 95% CI −2.0375 to −1.7096, upper limit = −1.5423, upper limit 95% CI 1.3783–1.7063; right lower quadrant of the abdomen: differences in arithmetic mean − 0.1844, 95% CI −0.2749 to −0.09385, P = .0001; SD = 0.8231, lower limit = −1.7977, lower limit 95% CI −1.9525 to −1.6428, upper limit = 1.4289; upper limit 95% CI 1.2740–1.5838). Regardless of lidocaine patch use, the VAS scores were significantly higher at ambulation than at rest (1.74 ± 2.30, 95% CI 1.59–1.88 versus 1.54 ± 2.20, 95% CI 1.40–1.68; P < .0001) (Table 3). However, there was no significant difference in VAS scores between rest and ambulation overall (P = .055) (Table 3).
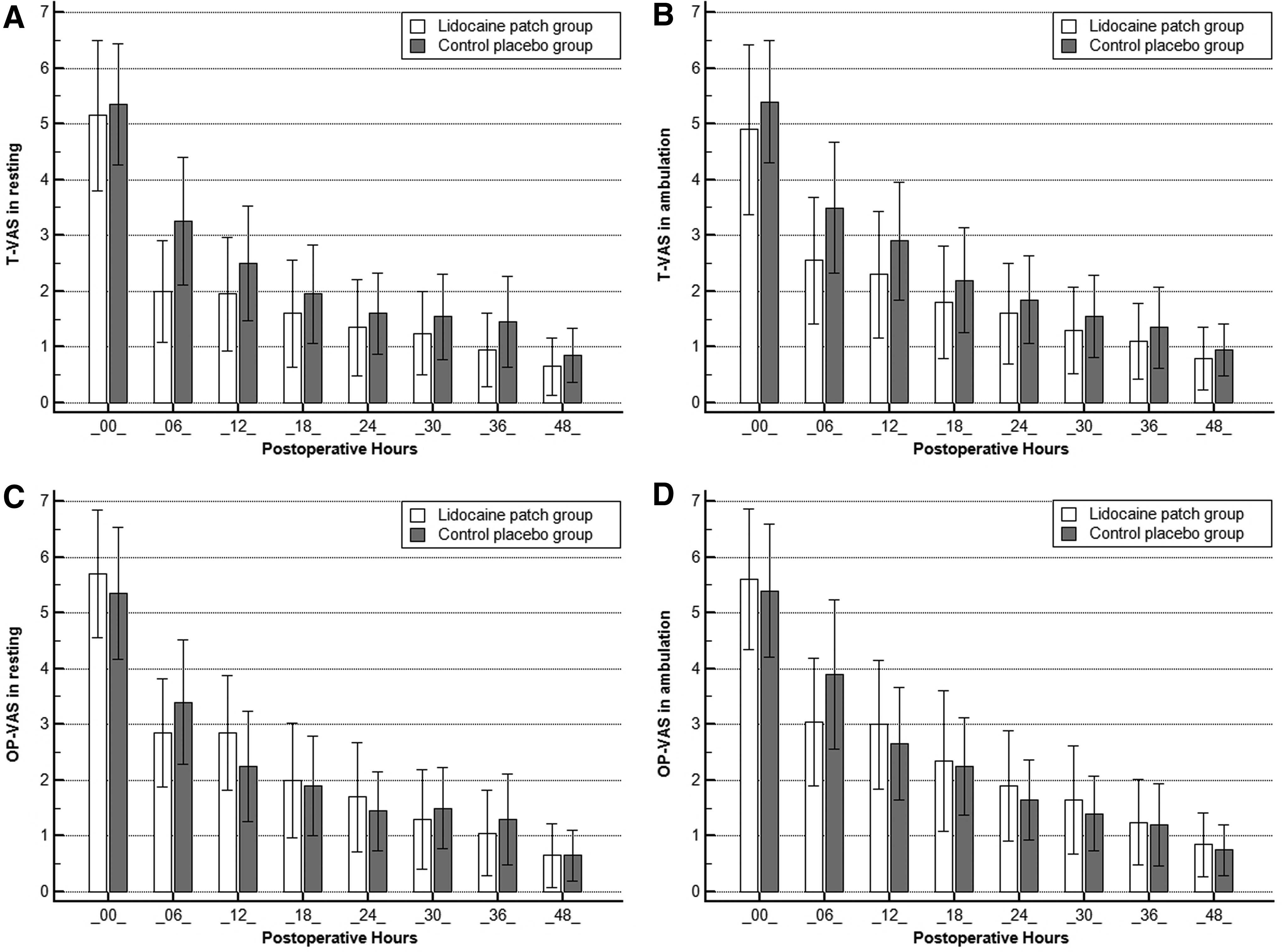
Difference in VAS scores for postoperative pain between the lidocaine patch and control groups.
Difference of VAS pain score for postoperative pain between lidocaine patch group and placebo group.
Data are presented as the arithmetic mean ± SD.
M/F, male/female; BMI, body mass index; ASA, American Society of Anesthesiologists; WBC, white blood cells; CRP, C-reactive protein; SD, standard deviation.
Data are presented as the arithmetic mean ± SD.
T-VAS, trocar site pain measured with visual analog scale score; hr, hour; RM-ANOVA, two-way analysis of variance; RLQ-VAS, right lower quadrant area pain measured with visual analog scale score; S-VAS, shoulder area radiating pain and all of other pain measured with visual analog scale score; SD, standard deviation.
Data are presented as the arithmetic mean ± SD at the top, 95% CI for the mean in the middle and numbers in each group at the bottom.
SD, standard deviation; CI, confidence intervals; No., number of enrolled patients; T-VAS, trocar site pain measured with visual analog scale score; LP, lidocaine patch; RLQ-VAS, right lower quadrant area pain measured with visual analog scale score; S-VAS, shoulder area radiating pain and all of other pain measured with visual analog scale score; Total VAS, VAS including all of the T-VAS, RLQ-VAS, and S-VAS.
Discussion
Various factors may cause pain after laparoscopic surgery. Gaseous pneumoperitoneum-related factors include neuropraxia of the phrenic nerve, type of insufflated gas, intra-abdominal pH, residual intra-abdominal gas, gas temperature, and gas humidity. In addition, there are sociocultural and individual factors as well as operation-related factors, such as the number/size of incisions, wound drainage, and use of appropriate analgesics. 1 These factors should be considered in the management of postoperative pain. Although laparoscopic appendectomy is considered a minor surgical procedure because of its short operation time as well as minimal bowel irritation and manipulation in many cases, it requires multimodal pain management due to moderate to severe postoperative pain in some cases. 11 For this reason, proper pain management after laparoscopic surgery is important for quality of life during the immediate postoperative period. The conventional pain control method is systemic administration of analgesics, including opioids, NSAIDs, and acetaminophen, which frequently cause side effects. In contrast, topical anesthetics act directly on the pain area and minimize the incidence of side effects and drug–drug interactions. 3 Topical anesthetics have an analgesic effect by suppressing the activity of peripheral sodium channels of sensory afferents, thereby reducing ectopic paroxysmal discharge and pain transmission as well as decreasing expression of mRNA in the sodium channel. 12 In addition, topical anesthetics suppress release of proteolytic and inflammatory mediators from the surgically damaged tissue, which activate and maintain postoperative pain, thereby inducing antinociception and alleviating the pain.13,14 There have been numerous studies on the effects of topical anesthetics on postoperative pain. Cervini et al. 4 have reported that intraoperative bupivacaine administration reduces the use of parenteral narcotics after laparoscopic appendectomy. However, Ghezzi et al. 5 have documented that preemptive ropivacaine infiltration into the trocar site is not effective in relieving pain after gynecologic laparoscopy. A recent study of 226 patients undergoing laparoscopic gynecological surgery has demonstrated that lidocaine infiltration into the port site is beneficial for postoperative pain relief during the early postoperative period. 8 In the present study, we used the 10 × 14-cm lidocaine patch 5% (700 mg) which is soft, elastic, and cohesive, and acts for up to 12–24 hours. The patch is approved by the Food and Drug Administration as a peripheral analgesic for postherpetic neuralgia. 15 The lidocaine patch has been shown to be effective for osteoarthritis, 16 low-back pain, 17 diabetic polyneuropathy, 18 and carpal tunnel syndrome. 19 Saber et al. 9 have indicated, in a study of 30 patients undergoing laparoscopic ventral hernia repair, that lidocaine patch is effective for postoperative pain control. Kwon et al. 10 have studied 40 patients who were treated with laparoscopic gynecologic surgery and reported that since the VAS scores were significantly lower in the lidocaine patch group than in the control group, topical lidocaine patches can reduce postoperative wound pain. Elhafz et al. 20 studied 27 patients undergoing laparoscopic colorectal surgery with lidocaine patch and intravenous administration of lidocaine. They stated that the lidocaine patch group showed lower VAS scores than the placebo group for 72 hours after surgery and that the amounts of morphine used were also smaller in the lidocaine patch group. They also mentioned that there was no significant difference in VAS scores between the lidocaine patch and intravenous lidocaine groups. However, in our study, the VAS scores at the trocar site at rest and ambulation were lower in the lidocaine patch group than in the control group, without statistical significance. Also, there was no significant difference in the VAS scores at the right lower quadrant of the abdomen at rest and ambulation between the two groups. The reason for this may have been attributed to insufficient doses of lidocaine because the lidocaine patch 700 mg was equally divided into eight pieces and applied to the study areas. Since this is a randomized, prospective, controlled study, the data are reliable. However, this cannot be generalized due to its small sample size. Further studies with a larger sample size and adequate doses of lidocaine are needed to confirm our results.
In conclusion, the results of this study suggest that the lidocaine patch 5% may be effective in port site pain control after laparoscopic appendectomy.
Institution Approval
The present study has been approved by the IRB human research Konkuk University Chungju Hospital (KUCH 2016-03-015).
Author's Contributions
Kim, Hur, and Lee drafted the article, searched the literature and the findings, and wrote the article. Lee and Kim critically reviewed the article. All authors read and approved the final article submission.
Footnotes
Disclosure Statement
No competing financial interests exist.