
Abstract
Abstract
Background:
Owing to the aggressive nature of radical nephroureterectomy (RNU), it is extremely important for the diagnostic modalities to be accurate. The European Association of Urology guidelines recommend that diagnostic ureteroscopy (URS) and biopsy be performed for upper urinary tract urothelial carcinomas (UUTCs). But that diagnostic URS adversely affects oncologic outcomes still exist. In the current systematic review and meta-analysis, we had attempted to evaluate oncologic outcome of diagnostic URS before RNU.
Methods:
All relevant articles were retrieved from PubMed, Embase, Web of Science, and the Cochrane Library. Endpoint events were recurrence-free survival, metastasis-free survival, cancer-specific survival, and overall survival.
Results:
Compared with patients who underwent RNU alone, those who underwent diagnostic URS before RNU had significantly higher intravesical recurrence rate (HR = 1.42, 95% CI: 1.24–1.61, I2 = 37%). Overall, no significant difference was found in CSS (HR = 0.72, 95% CI: 0.51–1.03, I2 = 0%) and OS (HR = 0.73, 95% CI: 0.45–1.19, I2 = 0%) between patients who underwent diagnostic URS and those who did not. Meanwhile, there was lack of evidence indicating that the risk of tumor metastasis increased after diagnostic URS (HR = 0.97, 95% CI: 0.74–1.26, I2 = 0%).
Conclusions:
Diagnostic URS before RNU does not seem to compromise long-term survival outcomes, even though it is associated with a higher rate of intravesical recurrence (IVR). Our findings suggest that further investigation, especially through prospective studies, should focus on decreasing the rate of IVR by administration of intravesical chemotherapy immediately after diagnostic URS.
Background
U
Ureteroscopy (URS) is a useful tool for visual detection and to provide a working channel during UTUC biopsy. In their prospective study, Grahn et al. 7 reported that diagnostic URS has significantly higher specificity and accuracy than multiphase CTU. Golan et al. 8 and Sadow et al. 9 reported that all suspicious filing defects of size less than 5 mm discovered on CTU were found to be benign morphological changes on diagnostic URS. In addition, some experts reported that the rate of the specificity of diagnostic URS with biopsy reaches 100%.10,11 Nonetheless, concerns related to the increased risk of recurrence, progression, and metastases following diagnostic URS persist. First, the surge pressure in the renal pelvis may increase the possibility of dissemination through submucosal vessels or lymphatic tubes during the irrigation step of diagnostic URS, and this would counteract the survival benefits.12,13 Second, slough tumor cells along with the irrigation fluid can flow back into the bladder and get implanted in the mucous membrane, which increases the risk of intravesical recurrence.
Previous studies have evaluated the oncologic outcomes of diagnostic URS using different endpoint events, such as recurrence-free survival, intravesical recurrence (IVR), metastasis-free survival (MFS), cancer-specific survival (CSS), and overall survival (OS). For this reason, it is difficult to draw constructive conclusions without a systematic analysis of current studies. The aim of the present systematic review and meta-analysis was to compare and evaluate oncologic outcomes of patients with and without diagnostic URS before RNU.
Methods
Identification of studies
All relevant articles were retrieved from PubMed, Embase, Web of Science, and the Cochrane Library using the following search terms: (“upper tract urothelial carcinomas” OR “ureteral carcinoma” OR “pelvic carcinomas”) AND (“Ureteroscopy” OR “Ureteroscopic surgery”) AND (“intravesical recurrence” OR “cancer specific survival” OR “overall survival” OR “metastases free survival”); last updated: 10 May, 2017).
Inclusion and exclusion criteria
Study eligibility was defined on the basis of the participants, (P), intervention (I), comparator (C), and outcome (O) (PICO) approach, as recommended in the Systematic Reviews and Meta-analysis (PRISMA) guidelines 14 . In the present analysis, a study was included if it met the following criteria: it included patients with UTUCs (P) who did (I) or did not (C) undergo diagnostic URS following RNU, and analyzed oncologic survival outcomes (O). Additionally, the studies needed to (i) compare oncologic outcomes between patients who underwent diagnostic URS following RNU and those who did not undergo diagnostic URS following RNU; (ii) present results included at least one of the following outcomes: IVR, CSS, OS, and MFS; and (iii) be published in English. Studies were excluded if they were editorials, letters to the editor, reviews, case reports, or meeting abstracts. The primary results of the literature search were exported to EndNote, and 711 duplications were identified.
Data extraction and outcomes of interest
Data from the included reports were extracted independently by two investigators (Z.F.L. and S.Y. Z.). All disagreements were resolved by adjudication by the senior author (Z.W.L.). The extracted data included the name of the first author, year of publication, study design, number of participants in each treatment group, participants' age and gender, and the outcomes of interest. Our primary outcome was IVR, and the secondary outcomes were CSS, MFS, and OS.
Quality assessment
Criteria established by the Center for Evidence-Based Medicine in Oxford, UK, were used to rate the level of evidence in the included studies 15 . The modified Newcastle–Ottawa scale, a validated tool to evaluate nonrandomized studies, was used to assess the risk of bias in the nonrandomized control trials. This scale involves three factors, namely, patient selection, comparability of the study groups, and assessment of outcomes. We determined that the included studies were high-quality articles with scores exceeding 7.
Statistical analysis
A meta-analysis was conducted using Review Manager 5.0 (Cochrane Collaboration, Oxford, United Kingdom) to examine studies comparing the same pair of treatments. Generally, the hazards ratio (HR) is considered the only summary statistic for censored outcomes as described by Parmar 16 . In the present study, we used the HRs and 95% confidence intervals (CIs) to determine the relationship between URS and oncologic survival outcomes (IVR, CSS, MFS, and OS). Standard deviations were calculated using the technique described by Hozo et al. 17 for continuous variables, which were presented as mean and range values in the included studies. Statistical heterogeneity among the reports was assessed using the chi-square test with significance set at P < .05, the I2 statistic, and a forest plot. The random-effects model was used when data were significantly heterogeneous (I2 > 50%); otherwise, the fixed-effects model was used. Subgroup analyses for IVR were conducted to evaluate the influence of diagnostic URS with biopsy and history of bladder cancer. Sensitivity analyses were performed to explore the potential sources of heterogeneity and eliminating the effect of low-quality articles. Potential publication bias was screened using funnel plots.
Results
Overall study characteristics and eligibility
The flow of study selection and the funnel plot of all included studies were presented as Figures 1 and 2, respectively. Overall, after 1092 studies were excluded, 9 studies met the inclusion criteria and were included. Data of patients from the 9 included studies18–26 were examined in this systematic review and meta-analysis. In total, 3198 patients were analyzed, including 1038 patients who underwent diagnostic URS before RNU and 2160 patients who did not. None of the 3198 patients underwent kidney-sparing surgery or endoscopic treatment. With the exception of one study published in 1999, the remaining studies were published after 2000, including one published in 2010 and seven published in the last 5 years. All included studies were retrospective. Four of the included studies were considered to be of high quality (7 scores) and the remaining five had scores of 5–6 (Table 1).

Study selection flow.
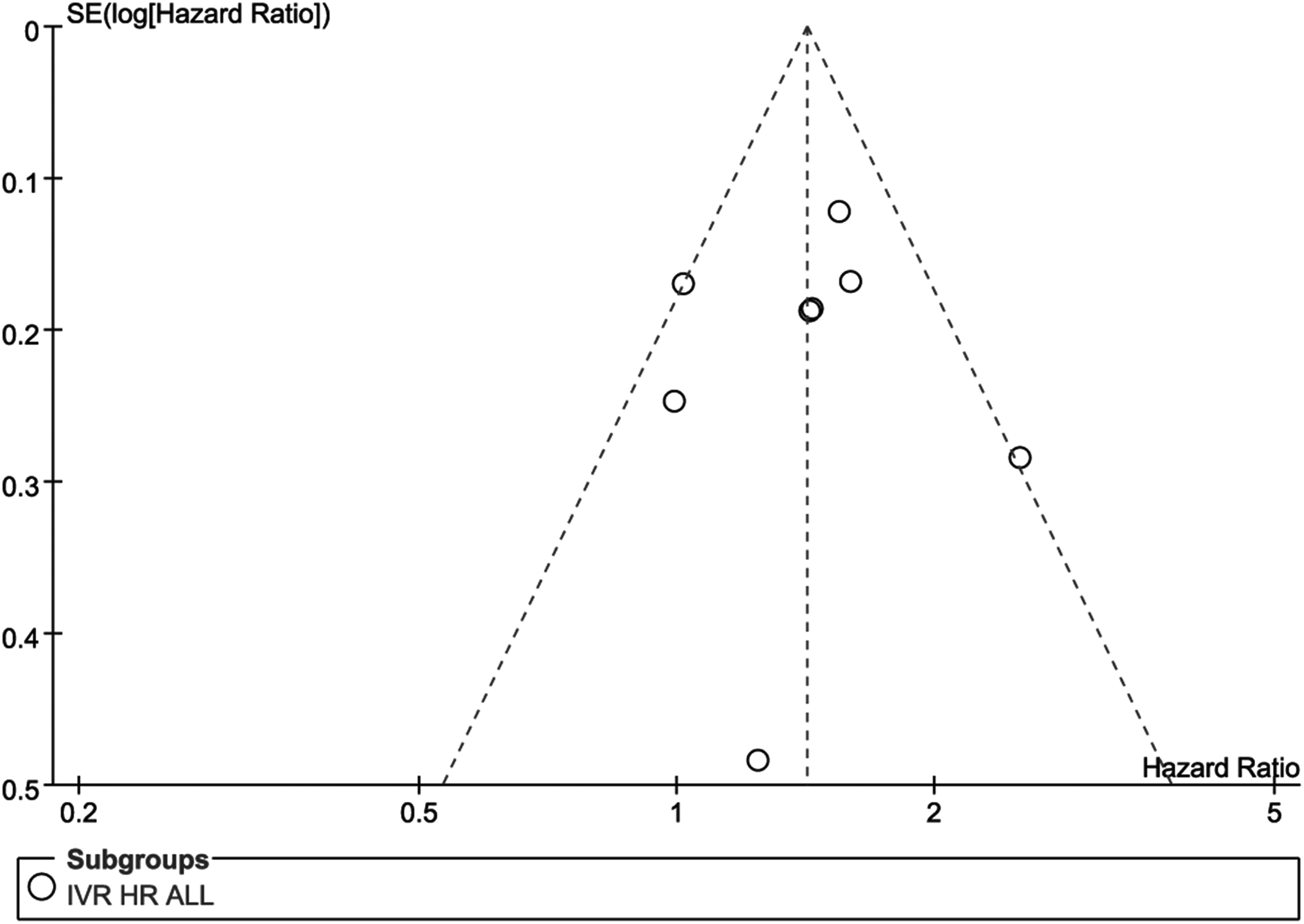
Funnel plot of all included studies. IVR was compared between patients who underwent diagnostic URS before RNU and those who did not. SE, standard error; OR, odds ratio; IVR, intravesical recurrence; RNU, radical nephroureterectomy; URS, ureteroscopy.
Matching: 1, tumor grade; 2, tumor stage; 3, cis; 4, lymphovascular invasion; 5, history of bladder tumor; 6, multiple tumors.
R, retrospective; NA, data not available; URS, ureteroscopy.
Patients' demographic and clinicopathological features
Diagnostic URS was far more likely to be selected for patients with smaller, low-grade, <T2 stage, ureter tumors (Table 2). This choice was not affected by American Society of Anesthesiologists score (Table 3).
NA, data not applicable.
NA, data not available; URS, ureteroscopy; ASA, American Society of Anesthesiologists.
Intravesical recurrence
We found that compared with patients who underwent RNU alone, those who underwent diagnostic URS before RNU had a significantly higher IVR (HR = 1.42, 95% CI: 1.24–1.61, I2 = 37%, Fig. 3A). Nison et al. 20 defined disease recurrence as bladder or contralateral upper urinary tract recurrence. After the study by Nison et al. 20 was excluded, the heterogeneity decreased from 37% to 9%, but diagnostic URS still significantly increased the rate of IVR (HR = 1.50, 95% CI: 1.31–1.73, I2 = 9%, Fig. 3B). After exclusively including patients with RNU and bladder cuff excision, diagnostic URS associated with high risk of IVR (HR = 1.46, 95% CI: 1.26–1.69, I2 = 0%, Fig. 3C). We noticed that five literatures had no neoadjuvant or adjuvant chemotherapy and their outcome shows that diagnostic URS was a risk factor for IVR (HR = 1.34, 95% CI: 1.13–1.59, I2 = 0%; Fig. 3D). Subgroup analysis, including patients who did not receive intravesical chemotherapy after RNU (HR = 1.50, 95% CI: 1.25–1.78, I2 = 0%, Fig. 3E), and excluding patients with a history of bladder cancer (HR = 1.71, 95% CI: 1.38–2.11, I2 = 0%; Fig. 4A), showed the same result. The biopsy during the diagnostic URS did not significantly influence the rate of IVR (HR = 0.81, 95% CI: 0.61–1.07, I2 = 0%, Fig. 4B). Lee et al. 18 and Sung et al. 23 classified patients into two groups according to the period between diagnostic URS and RNU: one group underwent diagnostic URS and RNU on the same day, whereas RNU was delayed in the other group. Therefore, subgroup analysis between patients who received concurrent RNU after diagnostic URS and those who received delayed RNU was presented in Figure 4C. Totally, there was no evidence that delayed RNU significantly increased the risk of IVR (HR = 0.90, 95% CI: 0.61–1.32, I2 = 1%, Fig. 4C).
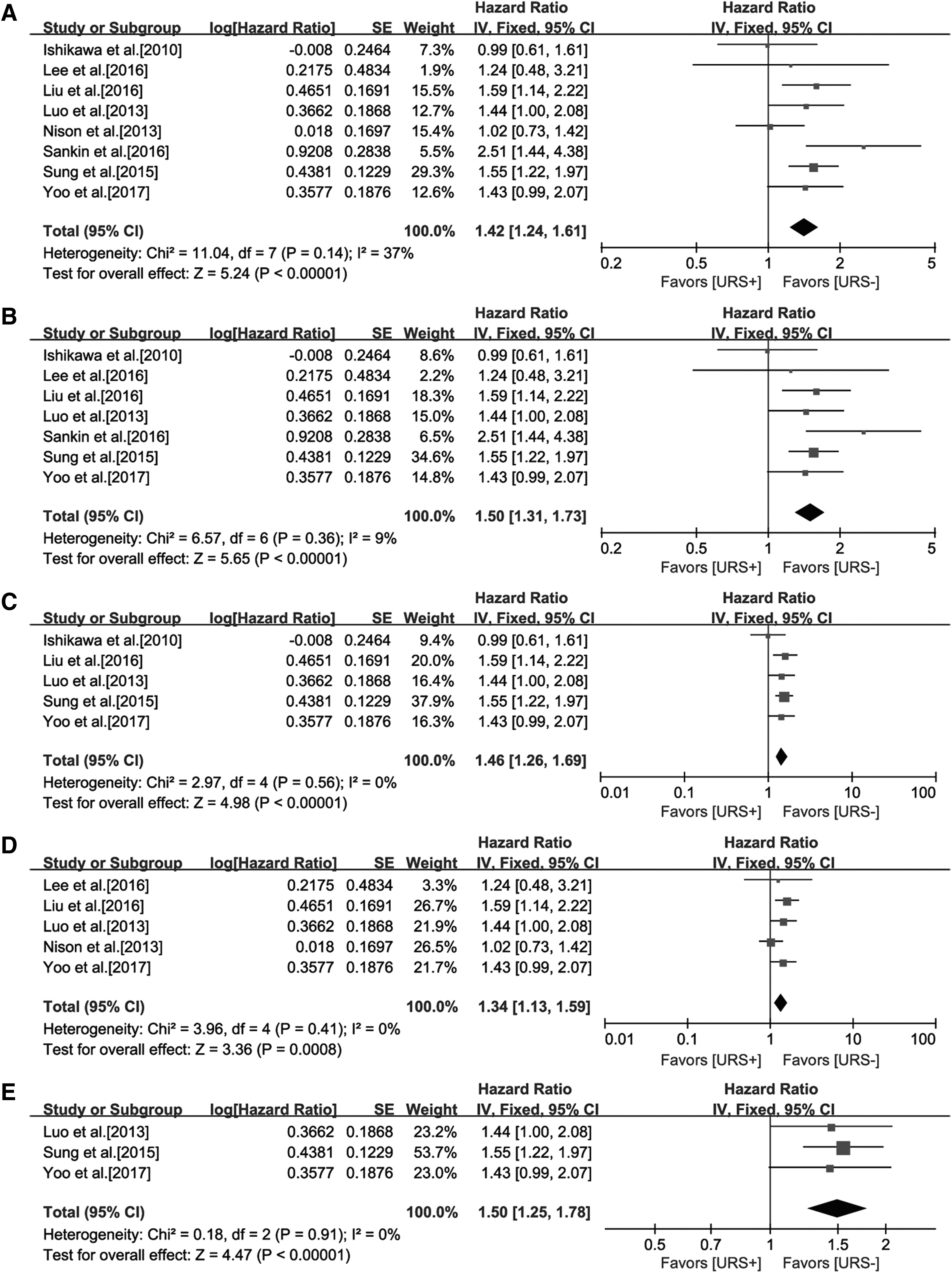
Forest plot and meta-analysis of IVR.
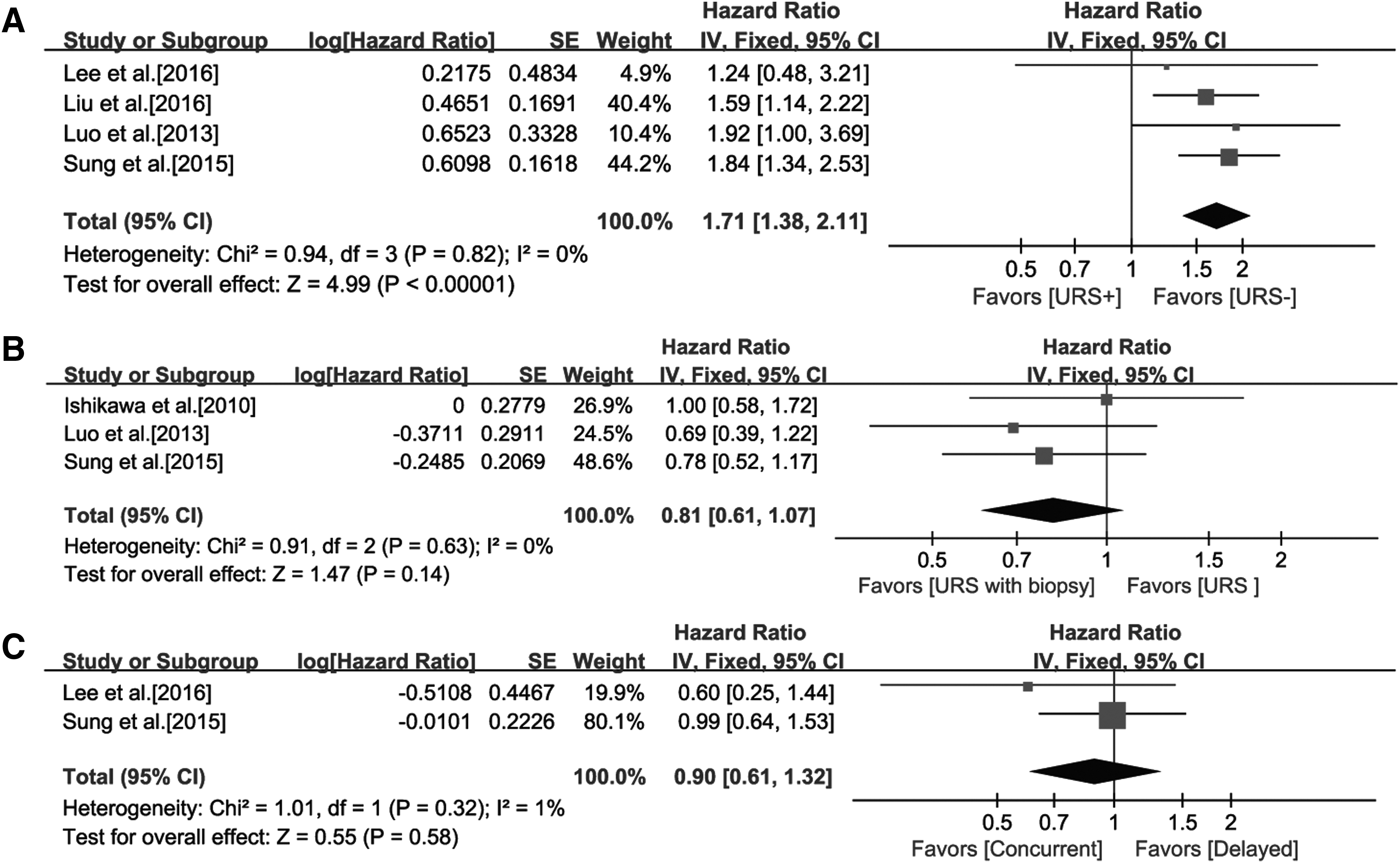
Forest plot and meta-analysis of IVR.
Long-term survival endpoint events (MFS, CSS, and OS)
The heterogeneity in the subgroup analyses for long-term survival endpoint events were mostly low (I2 = 0%). Overall, no significant difference was found in CSS (HR = 0.72, 95% CI: 0.51–1.03, I2 = 0%, Fig. 5A) and OS (HR = 0.73, 95% CI: 0.45–1.19, I2 = 0%, Fig. 5B) between patients who underwent diagnostic URS and those who did not. Meanwhile, there was lack of evidence indicating that the risk of tumor metastasis increased after diagnostic URS (HR = 0.97, 95% CI: 0.74–1.26, I2 = 0%, Fig. 5C).
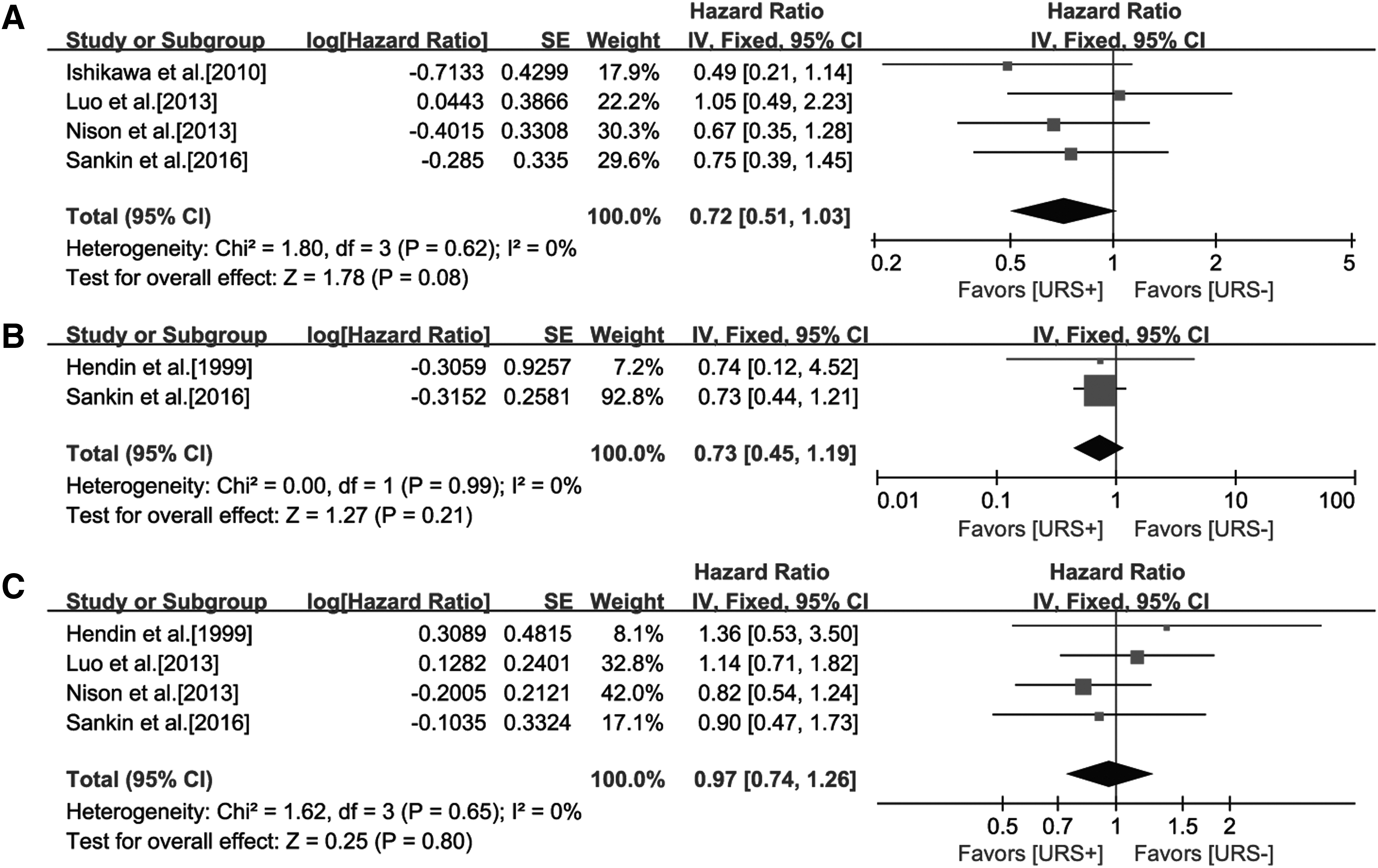
Forest plot and meta-analysis of long-term oncologic survival outcomes. Outcomes were compared between patients who underwent diagnostic URS before RNU and those who did not.
Discussion
RNU is recommended as standard surgery for patients with UUTCs. However, it is an extremely aggressive surgery and is generally accompanied by loss of half the renal unit. Therefore, accurate diagnosis plays an essential role in the treatment of patients. In fact, diagnostic URS has a higher sensitivity and specificity than other imaging modalities,7,8 but the grade for which the EAU guidelines recommend the use of this technique is C. 2 Currently, concerns about the increased risk of recurrence, progression, and metastasis following diagnostic URS persist.12,27 Minowada et al. 28 reported that three (75%) patients with grade three UUTCs who underwent diagnostic URS before RNU developed systematic metastases within a year of the surgery.
We found that diagnostic URS before RNU was associated with significantly higher rate of IVR, but not poorer MFS, CSS, or OS. An explanation for the increased risk of IVR after diagnostic URS is that tumor cells get detached and are shed following the fluid irrigation step of URS. However, heterogeneity across the nine studies included for evaluation of the IVR was modest (I2 = 37%). According to some studies, patient characteristics (gender and history of preoperative chronic kidney disease), type of surgery (e.g., laparoscopic or open), tumor differentiation (T stage, number, etc.), and a history of bladder cancer also affect the IVR rate.29–32 Therefore, we conducted some subgroup analyses with the aim of reducing heterogeneity.
Because patients with a history of bladder urothelial carcinomas have a higher possibility of IVR after RNU than those without these conditions,29–32 we performed a subgroup analysis of patients without a history of bladder urothelial carcinomas. Similar to previous studies, we found that diagnostic URS was associated with a significant higher rate of IVR in these patients (I2 = 0%, Fig. 4A). Subsequently, we analyzed that literatures included patients with RNU and bladder cuff excision and the outcome show diagnostic URS also significantly increased the risk of IVR (I2 = 0%, Fig. 3C). Recently, Nissar et al. 33 reported that diagnostic URS with biopsy before RNU were significantly associated with a higher risk of IVR compared with diagnostic URS without biopsy before RNU. However, we found that diagnostic URS with biopsy did not significantly increase the risk of IVR (I2 = 0%, Fig. 4B). Since it is known that prophylactic intravesical chemotherapy could significantly decrease the IVR 34 , we performed a subgroup analysis excluding patients receiving intravesical chemotherapy following RNU, and our findings confirmed that diagnostic URS appeared to increase the risk of IVR (I2 = 0%, Fig. 3E). Some experts are also concerned that a prolonged interval between diagnostic URS and RNU might increase the risk of tumor seeding. The findings of our study did not show that concurrent RNU was beneficial toward decreasing the risk of IVR (I2 = 1%, Fig. 4C). At present, whether or not IVR after RNU affects the survival benefits remains debatable. Yamashita et al. 35 reported that IVR was associated with the risk of poor CSS (HR = 4.27, P = .016), whereas Xylinas et al. 31 did not observe such a relationship between IVR and CSS (log rank P = .06).
The high irrigation pressure in the renal pelvis and ureter caused by diagnostic URS may contribute to tumor metastasis through the vascular or lymphatic tube. Our study found similar long-term survival (MFS, CSS, and OS) among patients who underwent diagnostic URS before RNU to those who underwent RNU alone. Notably, we found that patients who underwent diagnostic URS had been conferred potential tendency for better CSS and OS. Indeed, we were not able to conclusively interpret this phenomenon because we were unable to acquire individual data. Keeley et al. 36 noted that diagnostic URS combined with biopsy could provide precise information about tumor stage and grade. We speculate that accurate diagnosis of tumor stage and grade contributes to the decision about the necessity of lymph node dissection during RNU, which shows survival benefits in a more extended scope dissection 37, 38. From the pathological viewpoint, the selection bias in patients from both groups is responsible for that potential tendency toward better CSS and OS. For example, patients who have not undergone diagnostic URS usually have predisposing factors, such as a higher tumor grade and T stage and larger tumors than those who have not (Table 2).
Not only did the URS allow direct visual examination of radiologic filling defects, but it also provided a working channel for the biopsy and other advanced imaging techniques. The prognostic information provided by imaging as well as pathological examination is critical for urologists to categorize patients so they receive the optimal treatment. Seisen et al. 39 established a risk-adapted selection system for patients with UUTCs who would benefit more from conservative treatment, in which diagnostic URS plays an essential role. The main strength of our study is that application of diagnostic URS before RNU does not compromise long-term survival outcomes. Furthermore, our findings mitigate concerns related to the poorer survival benefits in patients who undergo diagnostic URS before kidney-sparing surgery or endoscopic management.
The findings of the present study should be considered taking into consideration the limitations of the retrospective design of all included studies. First, the differences in clinicopathological features between groups may have introduced some bias in the results. Moreover, it is not possible to divide the patient groups between those with lower stage and grade tumors (T1-2 or low grade) and higher stage and grade tumors (T3-4 or high grade), and then further investigate the influence of URS on those subgroups. Future studies should mostly focus on the prognostic information provided by diagnostic URS for low-risk patients and high-risk patients separately.
In conclusion, accurate preoperative diagnosis and classification of UUTCs is critical for decision making regarding treatment. Diagnostic URS before RNU does not seem to compromise long-term survival outcomes, even though it is associated with a higher rate of IVR. Our findings suggest that further investigation, especially through prospective studies, should focus on decreasing the rate of IVR by administration of intravesical chemotherapy immediately after diagnostic URS.
Footnotes
Acknowledgments
The meta-analysis was designed by L.Z.F., Z.S.Y., and Z.F.J., and L.Z.W., L.Z.F., and Z.S.Y. performed the systemic review and data summary. Z.S.Y., L.X.D., G.S.J., and W.Y.J. were responsible for the analysis of pooled data. The article was written and modified by L.Z.F., Z.F.J., and L.Z.W. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.