
Abstract
Abstract
Introduction:
Patients with umbilical or epigastric hernias benefit from mesh- based repairs, and even more so if a concomitant rectus diastasis (RD) is present. The ideal technique is, however, still under debate. In this study we introduce the minimal invasive linea alba reconstruction (MILAR) with the supraaponeurotic placement of a fully absorbable synthetic mesh.
Materials and Methods:
Midline reconstruction with anterior rectus sheath repair and mesh augmentation by an open approach is a well-known surgical technique for ventral hernia repair. Between December 1, 2016, and November 30, 2017, 20 patients with symptomatic umbilical and/or epigastric hernias, and coexisting RD underwent a minimally invasive complete reconstruction of the midline through a small access route. The inner part of both incised and medialized anterior rectus sheaths was replaced by a fully absorbable synthetic mesh placed in a supraaponeurotic position.
Results:
Patients were hospitalized for an average of 4 days and the mean operating time was 79 minutes. The mean hernia defect size was 1.5 cm in diameter and the mean mesh size was recorded as 15.8 cm in length and 5.2 cm in width. Two patients sustained surgical postoperative complications in terms of symptomatic seroma occurrences with successful interventional treatment.The early results (mean follow-up period of 5 months) showed no recurrences and only 1 patient reported occasional pain following exertion without rest.
Discussion:
MILAR is a modification of the recently published endoscopic linea alba reconstruction restoring the normal anatomy of the abdominal wall. A new linea alba is formed with augmentation of autologous tissue consisting of the plicated anterior rectus sheaths. Supraaponeurotic placement of a fully absorbable synthetic mesh eliminates potential long-term mesh-associated complications. Regarding MILAR, there is no need for endoscopic equipment due to the uniquely designed flexible lighted retractors, meaning one assistant less is required.
Introduction
P
It has been demonstrated that RD produces weakness and deterioration in the functions of the myofascicular abdominal wall with associated muscular imbalance, core instability, and hyperlordosis related with back pain. Thinning and stretching of the connective tissue due to RD is an important risk factor for hernia development. The patients involved are likely to be exposed to a higher risk of recurrence following sutured umbilical and/or epigastric hernia repair. Such a treatment only distributes tension from one point to another with further attenuation of the weak adjacent linea alba. 6 It is comparable to darning socks regarding distinct distribution of tension predisposing to adjacent holes.
Referring to the hybrid technique of endoscopic linea alba reconstruction (ELAR) published by F. Köckerling, 7 we implemented a modification, restoring the anatomy of the abdominal wall without laparoendoscopic equipment. The minimal invasive linea alba reconstruction (MILAR) is started with the same small periumbilical incision, proceeding dissection with the help of new lighted retractors, and placement of a slowly absorbable synthetic mesh over the plicated midline to avoid permanent prosthetic material in situ.
Materials and Methods
With the informed written consent of our patients, we performed a prospective pilot series of 20 cases without approval by the local ethics committee of our institution, because the principally described operation technique and its results are reported in many publications between the years 1979 and 2016.8,9 Between December 1, 2016, and November 30, 2017, a total of 20 patients with symptomatic primary midline umbilical or epigastric hernias (1–4 cm defect size) and concomitant rectus abdominis diastasis (>2 cm) were recruited for MILAR repair with fully absorbable synthetic meshes at the Departments of General and Visceral Surgery of the Congregation Sisters of Charity Hospital, Linz, Austria. Patients with recurrent or incisional hernias were excluded.
Mesh device
The Phasix™ mesh (Bard, Davol) is a naturally derived fully absorbable surgical mesh. It looks, feels, and handles like macroporous monofilament polypropylene and is made of poly-4-hydroxybutyrate. In experimental 10 and clinical settings, 11 it showed good biocompatibility, allows tissue ingrowth supporting strength restoration of the abdominal wall, and disappears through hydrolysis over 6–18 months.
Technical description
Upon raising their head and beginning to sit up from a supine position during clinical examination, all patients typically exhibited marked bulging or denting of the anterior abdominal wall in combination with an umbilical and/or epigastric hernia. Evidence of these findings was demonstrated by small part ultrasound examination with measurement of size of the defect and width of the rectus divarication. No further preoperative imaging was required.
Patients are lying in the Lloyd Davis position with the right arm abduced. The surgeon is standing between the legs. We consider this being the most ergonomic position. Only one surgical assistant on the left-handed side of the patient is needed to hold two retractors because in contrast with the ELAR technique, laparoendoscopic equipment is not needed. 7 The skin incision is made on the left periumbilical side extending 2–3 cm upwards (Fig. 1). This is followed by lateral dissection of the Scarpa fascia and the subcutaneous tissue down to both anterior rectus sheaths at the level of the detached umbilical stalk. The hernia contents are reduced or cut away and removed (Fig. 2).

Skin incision.
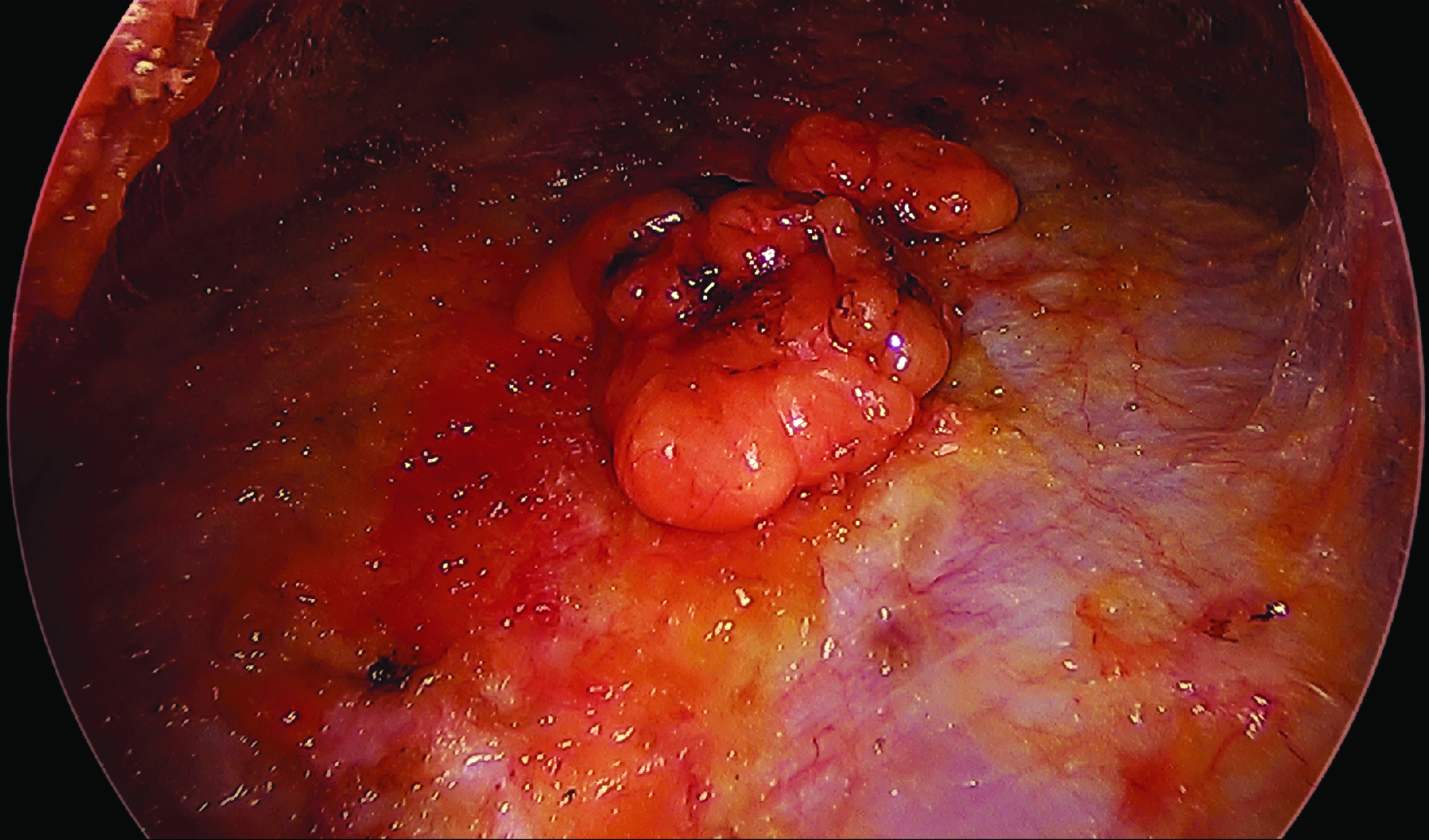
Umbilical hernia with removed hernia sac containing preperitoneal fat.
The cranial dissection proceeds beneath the subcutaneous tissue and both anterior rectus sheaths by elevating the skin with the help of lighted retractors (Lightmat™, Crura Surgical) (Fig. 3a–c). These malleable retractors bring cool, bright light exactly where it is needed in the surgical cavity (Fig. 4) and they can be customized into the desired shape for each individual case. Thus, the procedure can safely be continued as far cranially as needed until the linea alba remains at a physiological width smaller than 2 cm.
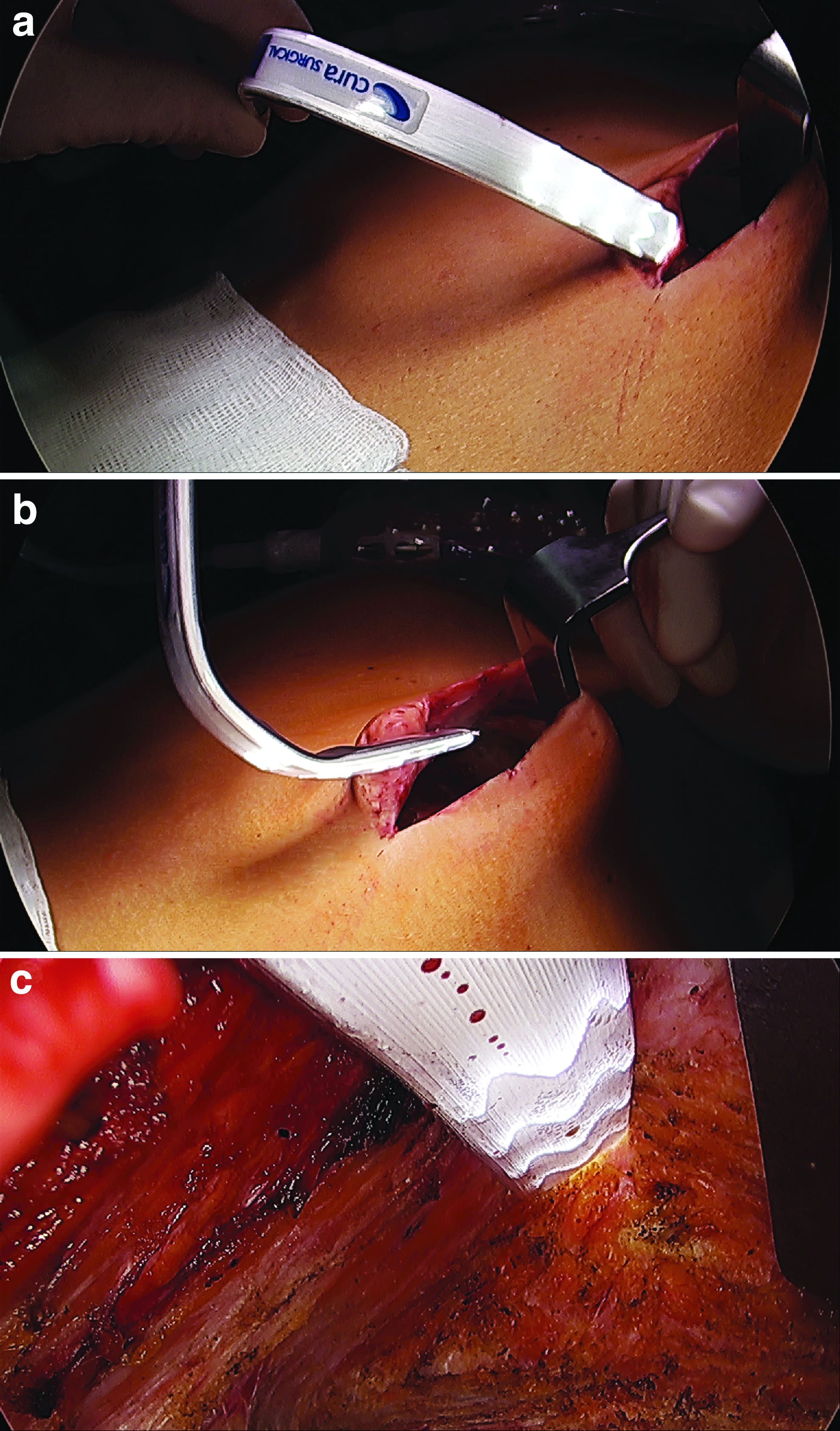

Lighted and dissected surgical supraponeurotic cavity from subumbilical to subxiphoidal.
Next, both rectus sheaths are incised 1 up to 4 cm apart from the medial borders of the rectus muscles depending upon the width of rectus divarication from the subumbilical area up to the defined cranial limit (Fig. 5). The length of the created space is measured by a sterile ruler (Fig. 6). The broader the diastasis, the more lateral the incision should be made due to the possibility of approximating the detached and medialized margins of both anterior rectus sheaths. This is crucial for a tension-free midline closure by suturing together the two medial parts of both anterior rectus sheaths with a slowly absorbable running suture (Fig. 7a–c). We use a polydioxanon self-anchoring knotless wound closure device USB 2/0 (Strattafix™, Ethicon). This suture results in a new linea alba with inverting plication of the anterior rectus sheaths approximating the rectus muscles nearly at their normal anatomic position. This is followed by measurment of the width of the resulting exposed muscle area (Fig. 8) between the incised fascial edges.

Paramedian incision of both anterior rectus sheaths.
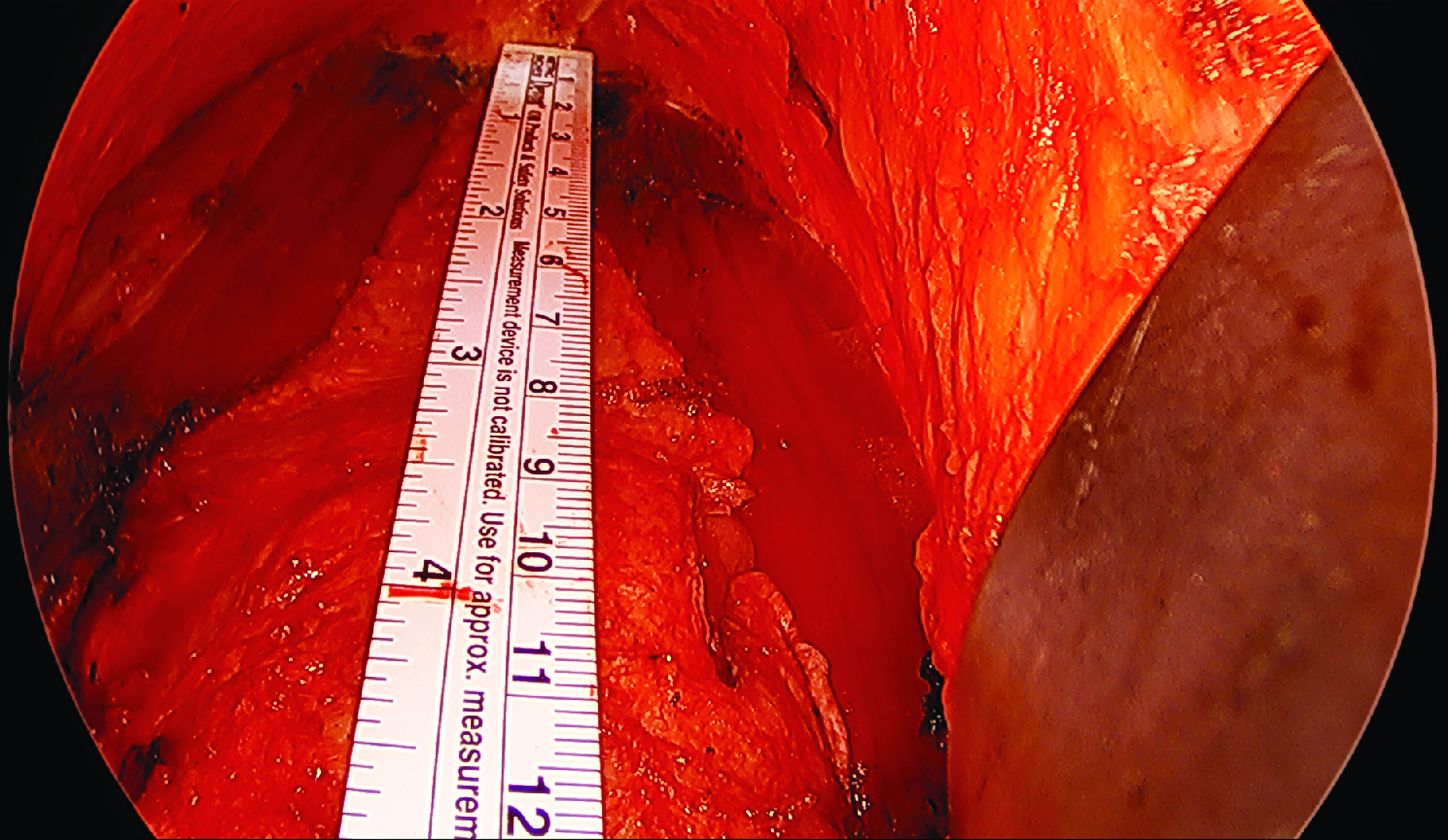
Measurement of defect length with a sterile ruler.

Closure of the medialized flaps of the detached anterior rectus sheaths with a running self-anchoring suture.
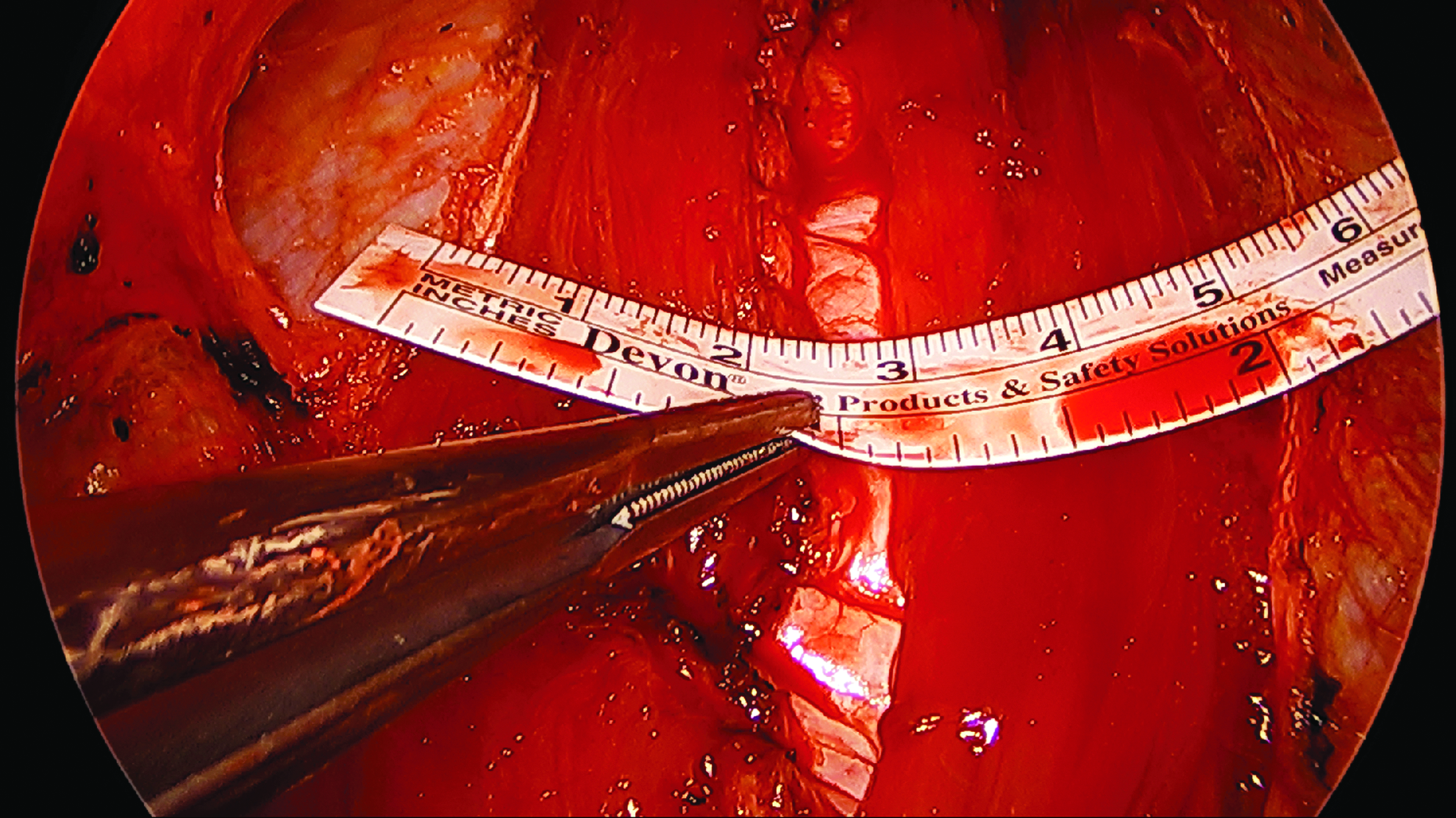
Measurment of the width of the resulting exposed muscle area between the margins of the remaining anterior rectus sheaths.
A Phasix mesh is then trimmed to a suitable size and fixed with running sutures to both remaining margins of the right and left anterior rectus sheaths for their replacement starting with one interrupted suture at the most cranial point with the help of a knot pusher (Fig. 9a–d). We assume that stable reinforcement of the midline had already been done by partial doubling and plication of the anterior rectus sheaths. The mesh replaces the detached anterior rectus sheaths covering the exposed muscular area for additional augmentation, and should therefore not be described as “onlay,” but rather as supraaponeurotic reinforcement. Eventually a suction drain (Charriere 10) is inserted and the skin is closed with absorbable intracutaneous sutures (Fig. 10).
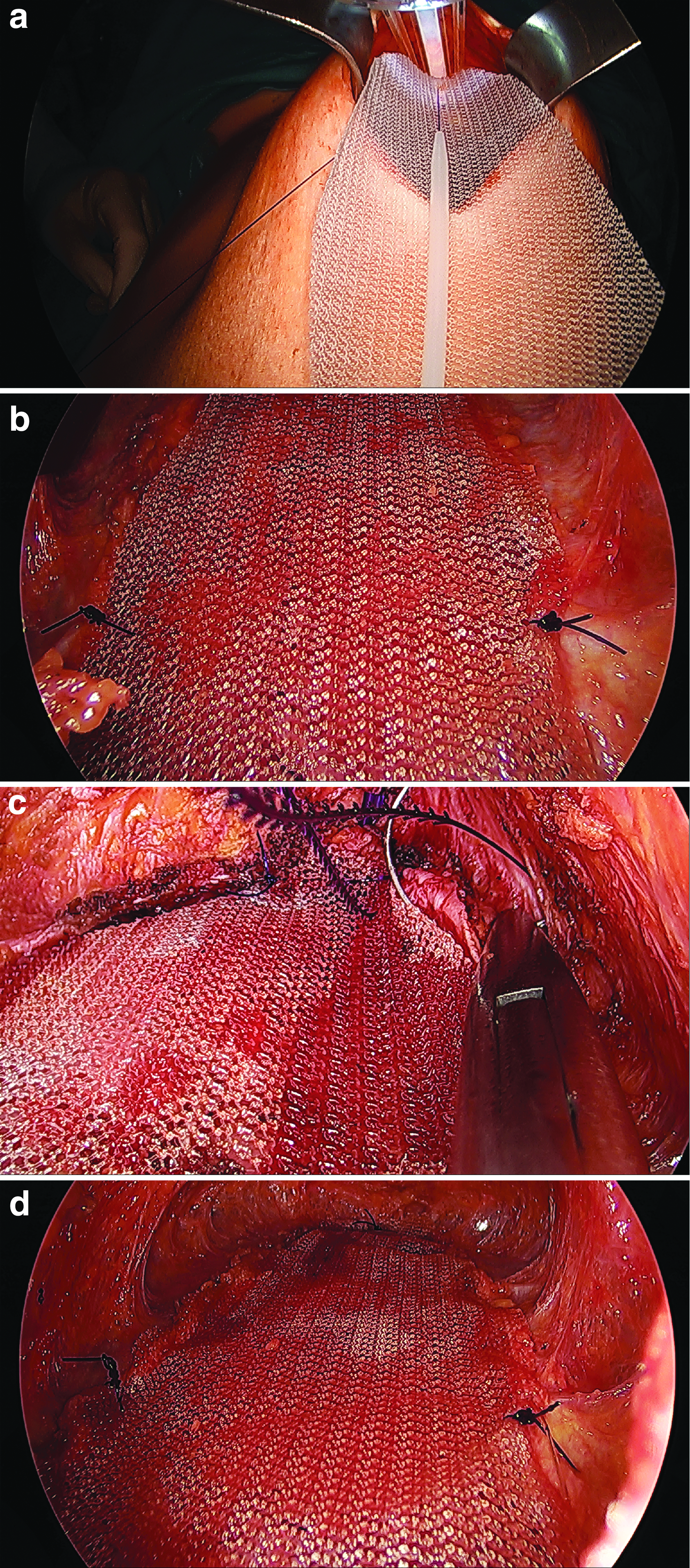
Mesh fixation (The top is fixed with an interrupted suture by the help of a knot pusher. The central points of both lateral margins and the bottom of the mesh are also fixed with interrupted sutures for secure mesh placement. Thereafter, the lateral borders are fixed with running self-anchoring sutures).

Situs after skin incision with an intracutaneous resorbable running suture.
In summary, MILAR effectively eliminates RD as the underlying cause of the abdominal wall weakness. Furthermore, it enables anatomical restauration of the rectus muscles, regaining their function to stabilize the trunk. Nevertheless, the myofascial release by creating flaps of the anterior rectus sheaths leads only to approximation and not to a narrow closure of the parallel running rectus muscles.
Results
Relevant demographic and disease characteristics and outcome parameters are presented in Table 1. One patient sustained postoperative hematoseroma with successful interventional treatment in terms of threefold puncture under local anesthesia and wound compression therapy. All patients attended a follow-up examination in January 2018 for current data collection before this publication. Four patients reported intermittent mild pain less in the midline, but rather on the cranial top of the incision and edgewise at the mesh margin, respectively. Only 1 patient took painkillers 6 months postoperatively after going to the gym, due to occasional stress pain.
EHS, European Hernia Society.
Discussion
The increase in intraabdominal pressure is the main cause of diastasis musculi recti abdominis. Two different types of people typically suffer from RD: first, middle-aged men with central obesity. When these patients start to sit up from a supine position, the contraction of the rectus muscles lead to a bulge in between. Second, small postpregnant women. The contraction of the rectus muscles results in a filiform dent on the thinned and stretched “Linea alba”due to low intraabdominal pressure. Usually, the latter group has much more abdominal wall compliance allowing easy reconstruction of the midline without tension. The rectus myofascial release in MILAR technique enables the centrifugal forces to bring the muscles toward the midline, facilitating closure without significant tension compared with the traditional method of correcting RD by plicating one immobilized anterior rectus sheath against the other. This method creates tension to the midline because fibrotic connections between the intact anterior rectus fascia encasing the muscles hamper medial advancement. Regarding the high coincidence of umbilical and or/epigastric hernias with RD (up to 50%), corrective surgery of all pathologies at the same time could represent the most recommended approach. 2
Novel compared to ELAR technique 7 are some modifications, making the procedure easier. First, the surgeon is standing between the patient`s legs, enabling working ahead without any need for permanent body rotation. Second, the lighted retractors make the laparoscopic equipment redundant, meaning one assistant less is required. The adjustment of the retractors by the surgeon himself brings light deep into the surgical cavity, exactly where it is needed at that moment. These retractors are intended for surgical procedures where visualization can be difficult and help surgeons save time and avoid complications. Third, the use of self-anchoring slowly resorbable sutures makes suturing much easier and faster. The sutures do not need to be tightened up and knotted. Fourth, the fully resorbable mesh stabilizes the autologous tissue and supports sustainable scar formation 10 without the risk of late-term mesh-associated complications. There are only very few studies available addressing this problem.
The 5-year risk of all mesh-related complications requiring subsequent surgery seems to be about 5%. Thus, the benefits attributable to mesh in terms of a lower recurrence rate are offset, in part, by mesh-related complications. 12 Therefore, long-term resorbable mesh represents a promising technology for ventral and inguinal hernia repair that supports strength restoration of the abdominal wall. Preclinical data evaluating mechanical strength, resorption properties, and histologic characteristics are promising. 10 A recent clinical study of complex ventral hernia repair supports preclinical findings, demonstrating positive outcomes and low incidence of hernia recurrence at 18 months. 11
From our point of view, absorbable mesh should not only be considered in contaminated or complex cases but also can play a role in young patients with increased expectation of life and prolific women not wishing to have permanent foreign substances in their body.
There is a clear trend among the hernia community toward extraperitoneal mesh placement. The paradigm shift goes toward defect closure, placing an uncoated mesh outside of the abdominal cavity, minimizing mesh fixation without compromising the repair, and using a minimal invasive/endoscopic approach. At this stage, there is reason to believe that minimal invasive non-intraperitoneal mesh repair techniques will play an essential role in the future.
Footnotes
Disclosure Statement
G.K. has received honorariums from Medtronic, Dahlhausen, and Bard for lectures and educational activities without any relation to this work.
I.F., R.K., and R.S. declare no conflict of interests. No competing financial interests exist.