
Abstract
Abstract
Background:
Endoscopic full-thickness resection (EFTR) derived from endoscopic submucosal dissection has gradually been accepted and even promoted for the treatment of submucosal tumors (SMTs) originating from the muscularis propria (MP) layer. However, there are some difficulties when EFTR is used to treat MP lesions in the gastric fundus. This study intends to explore whether EFTR can be made simpler, safer, and more effective with the traction assistance of dental floss.
Methods:
The clinical data of patients (trial group) with lesions in the MP layer in the gastric fundus undergoing EFTR with traction assistance of dental floss at Zhongshan Hospital, in 2016, were reviewed retrospectively. The control group was matched with the trial group according to tumor size. The differences in tumor resection time, patient hospitalization time, and complication rate were evaluated.
Results:
There was no significant difference in the average age of the two groups, each of which comprised 24 cases (58.7 ± 11.8 years versus 56.6 ± 7.9 years, t = 0.663, P = .511). However, there was a statistically significant difference in the operative time between the two groups (10.8 ± 2.8 minutes versus 19.0 ± 4.7 minutes, t = 7.298, P < .05). There was no statistically significant difference in the length of the postoperative hospital stay (3.2 ± 0.5 days versus 3.2 ± 0.5 days, t = 0.291, P = .772). In the trial group, there were 19 cases of gastrointestinal stromal tumors (group 1) and 5 cases of leiomyoma. The control group had similar results. Neither group experienced postoperative delayed bleeding, perforation, or other complications.
Conclusions:
When EFTR is used to treat SMTs originating from the MP in the gastric fundus, dental floss traction assistance can relieve the tumor boundary to simplify the surgical procedure and save the operation time.
Introduction
I
With the development of and advances in endoscopic resection, endoscopic full-thickness resection (EFTR), a technique derived from ESD and used to treat submucosal tumors (SMTs), has gradually become accepted and even promoted.3–6 When ESD is used to remove mucosal lesions, especially those of lager size, exposing the submucosa and revealing that the surgical incision depth is critical to the success of this technique. In addition, the dissection is more challenging and more time is required for resection when the tumor is located within the gastric fundus because of retroflexion of the endoscope and specific anatomical features. Similar situations are also common when EFTR is used to treat SMTs. In the past, many auxiliary traction methods for endoscopic resection have been invented to improve the efficiency and safety of ESD.7,8 Among these methods, dental floss traction assistance has been widely used, because it is easy to learn, affordable, and practical.9–11
The aim of this study was to evaluate the usefulness of EFTR-assisted dental floss traction for the removal of SMTs in the fundus of the stomach.
Methods
Patients
Between January and December 2016 at the Zhongshan Hospital of Fudan University, 24 consecutive patients with SMTs of the gastric fundus originating from the muscularis propria (MP) layer were treated with EFTR, assisted by dental floss traction; these patients made up the trial group. Lesions in the control group, which were also located in the fundus of the stomach, were matched to the trial group according to tumor size and other clinicopathological characteristics; controls were recruited from January to December in 2015. All the tumors were defined by endoscopic ultrasonography (EUS) and/or computed tomography (CT) before EFTR.
Informed patient consent was also obtained before the procedures. The study was approved by the Institutional Review Board of Zhongshan Hospital.
Procedures
All endoscopic surgery procedures were performed by an experienced endoscopist (Y.S.Z.). All patients were treated under intravenous anesthesia with airway intubation. A single-channel endoscope (GIF-Q260J; Olympus, Japan or VME-98S; Aohua, China or EG-580RD; Fujifilm, Japan) was used during the procedures. A short transparent cap (ND-201–11802; Olympus) was attached onto the tip of the endoscope to improve endoscopic visualization. An insulated-tip knife (KD-611 L; Olympus), a hook knife (KD-620LR; Olympus), and/or a hybrid knife (ERBE; Tuebingen, Germany) were used during EFTR. A high-frequency generator system was used (ICC-200; ERBE, Germany). Other equipment included injection needles (NM-4 L-1), snares (SD-230 U-20), hot biopsy forceps (FD-410LR) (all from Olympus), and metal clips (ROCC-D-26-195-C; Micro-Tech, China).
EFTR with dental floss traction was performed as follows: (1) Marker dots were made close to the lesion. (2) Several milliliters of solutions (100 mL saline, 5 mL 0.8% indigo carmine, and 1 mL epinephrine) were injected around the lesion using a 23-gauge disposable needle to lift the mucosa. (3) The mucosa side furthest from the cardia was first incised along the marker dots using the hook knife or IT knife. (4) After the endoscope exited, the dental floss was tied to any arm of the metallic clip. (5) We reinserted the endoscope and attached the metal clip onto the tumor side that had been cut. (6) When the submucosa and boundary was clearly exposed with the dental floss pulled, active perforation was made by the hook knife first at one point around the lesion, and then a circumferential incision was made as deep as the serosal layer surrounding the lesion by IT knife. (7) Then, we aspirated the gastric fluid and completed the full-thickness incision of the tumor. (8) Finally, we closed the gastric wall defect by multiple metallic clips or a metallic clip interrupted suture with an endoloop, as reported previously (Fig. 1). 6 We have previously described 4 the EFTR procedure without dental floss traction. In the presence of pneumoperitoneum, a 20-gauge needle was inserted into the right upper quadrant of the abdomen to percutaneously decompress the abdominal cavity during the procedure. In all patients, a nasogastric tube was routinely inserted after endoscopic resection.
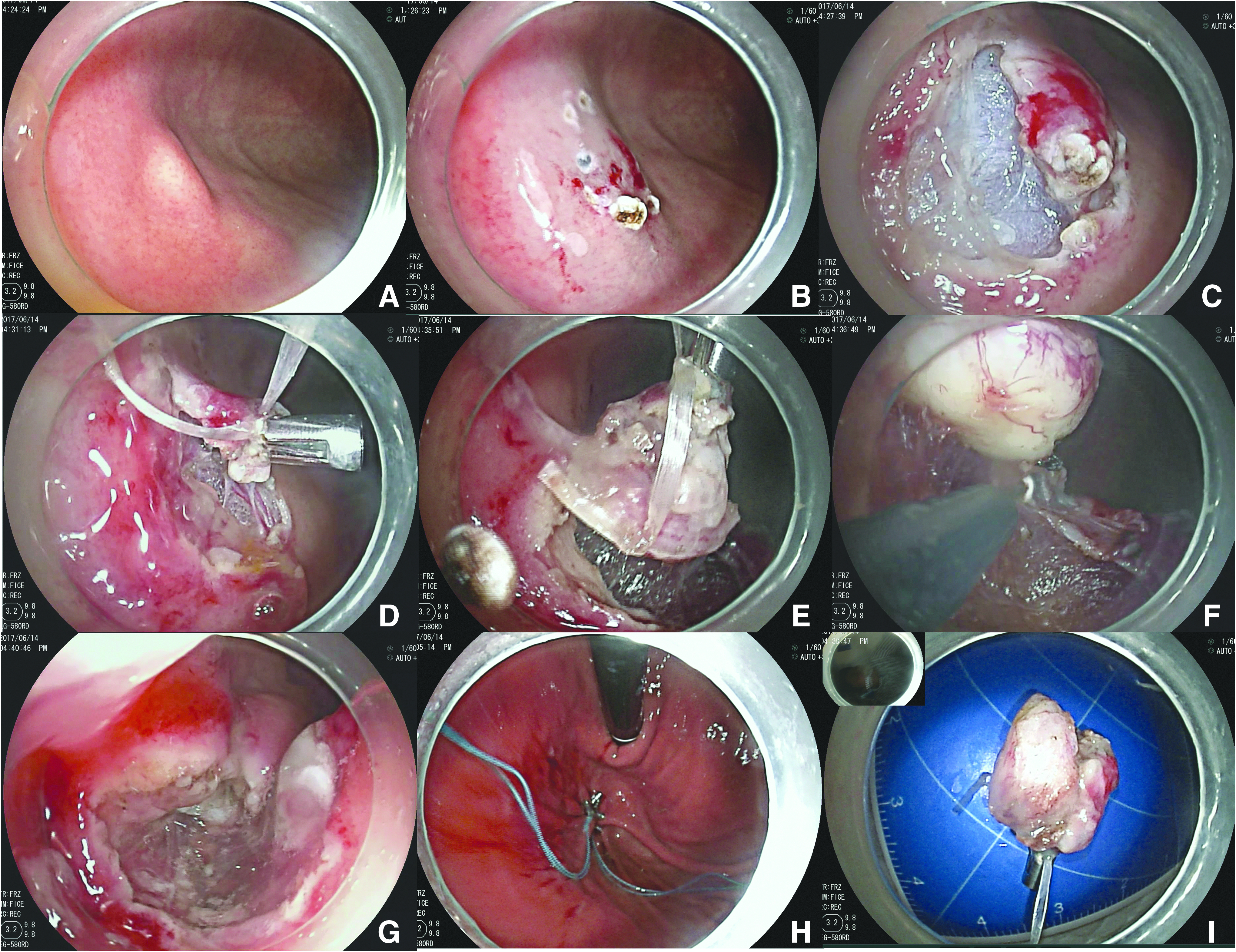
EFTR with the dental floss traction. (
Postoperative treatment and follow-up
All tumors, which were fixed in 10% formalin after endoscopic resection, were sent for pathological evaluation at the Pathology Department of Zhongshan Hospital. Proton pump inhibitors and intravenous antibiotics were routinely administrated to all patients after endoscopic resections. All patients were followed up with standard endoscopy and at 3, 6, and 12 months during the first year after the initial procedure to observe the healing of the wound and to check for residual tumor or recurrence. Subsequently, patients were followed up annually if no local recurrence was identified in two consecutive follow-up examinations.
Statistical analysis
Commercial software (IBM SPSS Statistics 18, Chicago, IL) was used for statistical analysis, and P < .05 was accepted to be statistically significant. Continuous values are expressed as the mean ± standard deviation.
Results
There were 10 males and 14 females in the trial group, with an average age of (58.7 ± 11.8) years and an average tumor size of 0.88 ± 0.33 cm. The tumors were all located in the MP layer, which was consistent with preoperative assessment by EUS or CT. In the control group (matched with the trial group), 24 cases were treated by the same doctor without dental floss traction from January 2015 to December 2015, including 6 males and 18 females. These patients had an average age of 56.6 ± 7.9 years and an average tumor size of 0.88 ± 0.33 cm. There was no significant difference between the two groups as far as age (t = 0.663, P = .511) or gender (F = 1.484, P = .229) is concerned.
The operation time of the experimental group was 10.8 ± 2.8 minutes, and the postoperative hospital stay was 3.2 ± 0.5 days. In the control group, the operation time was 19.0 ± 4.7 minutes, and the postoperative hospital stay was 3.2 ± 0.5 days. The operation time of the experimental group was significantly less than that of the control group (t = 7.298, P < .05). However, there was no significant difference in the postoperative hospital stay between the two groups (t = 0.291, P = .772). Both the trial and the control groups had the same pathological results with 19 cases of gastrointestinal stromal tumors (group 1) and 5 cases of leiomyoma. No postoperative complications, such as delayed bleeding or delayed perforation, were found in the two groups, and no patients were transferred to a surgical operation.
Discussion
Gastrointestinal SMTs refer to a class of tumors located in the muscularis mucosa, submucosa, MP, or serosa. 5 Endoscopic techniques can assess the intracavity growth and surface mucosal integrity of most lesions. EUS can detect the level of tumor origin and speculate the nature of the tumors according to the tumor echo. In addition, endoscopic ultrasonography-time needle aspiration can be used to obtain lesion tissue to finish the pathological diagnosis. With an overall improvement in health awareness and the popularization of endoscopy, increasing numbers of SMTs have been found, diagnosed, and treated. Considering the malignant potential of some SMTs, including stromal tumors and neuroendocrine tumors, both doctors and patients have gradually accepted the use of minimally invasive endoscopic surgical resection for SMTs. 12 Endoscopic resection techniques have steadily gained popularity in recent years, as the technology has continued to grow, develop, and become more precise. 13
SMTs of the gastric fundus, treated by EFTR, usually originate from the MP layer, where stromal tumors and leiomyomas are most common. Due to the special site, some lesions were difficult to access, even with retroflexion of the endoscope. Therefore, the traditional method of using a transparent cap to expose the incision level was difficult to perform. It is apparent then that EFTR treatment for some SMTs in this area has a certain degree of difficulty. Inspired by the dental floss-assisted traction used in ESD treatment of mucosal lesions, we utilized an EFTR method combined with dental floss traction to treat gastric SMTs. 14 In clinical practice, we found that dental floss-assisted traction EFTR has certain advantages for the resection of SMTs in the gastric fundus.
First, dental floss traction can help to expose the tumor boundaries, so that the operation field is clearer, thus simplifying the operation process and significantly reducing the procedure time. Second, in the course of surgery, EFTR-assisted dental floss traction can better reveal the blood vessels or be used to find bleeding vessels for the prevention and early treatment of bleeding. Furthermore, this method also has some advantages in the prevention and treatment of accidental injury of the extravascular vessels during EFTR. This helps to reduce the risk of delayed postoperative bleeding. Third, when the tumor was completely resected, dental floss can also help prevent the tumors from slipping into the abdominal cavity and help remove the excised tissue. In this research, the average operation time of EFTR with dental floss assistance for SMTs of the gastric fundus was 10.8 ± 2.8 minutes, which was significantly shorter than the time it took to perform traditional EFTR (19.0 ± 4.7 minutes). In fact, the operation time of the trial group in this research also included the manufacturing time of the external traction devices, when the floss was fixed to the metal clip in vitro. Thus, even less time was spent performing EFTR for lesions in the trial versus control group.
There are many kinds of traction assistance that use metal clips, dental floss, or an endoloop for endoscopic resection, as reported previously.14–16 Compared with the previously reported methods, EFTR-assisted dental floss traction has its own advantages as follows: (1) the dental floss with metal clip was more suitable as a traction device, making it easier to cut the tumor during the process of snare and traction using the endoloop, (2) passive traction was performed, which means traction was used in the beginning of EFTR rather than when the border of tumor was not easy to expose or the bleeding site was not easy to find, (3) the metal clip was fixed on the mucosa above the tumor, which increased the stability of traction and avoided breaking the integrity of the tumor, (4) a metal clip can enter the biopsy hole in the closed state to avoid injuring the normal mucosa, and the location of the clamping can then be adjusted, (5) for SMTs in the gastric fundus, the tumor side near the gastric body can be cut first to facilitate traction. When the traction direction does not meet expectations, pulley traction, using another metal clip to secure the pull line to the opposite side, can be applied. 15 (6) Due to the auxiliary traction of the dental floss, the tissue can be cut under direct vision to ensure complete resection and a negative tumor edge.
EFTR-assisted dental floss traction also has some technical limitations to be improved for the clinical removal of SMTs. In the process of traction, the metal clip can easily fall off, if the strength of traction was too strong or the procedure time was too long, although the rate was lower than when the metal clip was directly connected with the tumor. In addition, because the metal clip was fixed on the mucosa above the tumor, the mucosa should not be cut too severely in the beginning to avoid removing the portion of the mucosa with the dental floss traction before the tumor is completely removed. However, this situation can be remedied by retraction. In the future, commercial dental floss with a metal clip traction device should be expected to save the time needed to make/prepare the traction device during the operation.
Some limitations are present in this study. The study design used was a retrospective, single-center trial; the number of research cases should be increased before making any firm conclusions. Therefore, a large, prospective, and randomized study is warranted.
Conclusions
In conclusion, dental floss traction assistance in EFTR for SMTs originating from the MP layer in the gastric fundus can help expose the tumor boundaries so that the incision can be made while directly viewing it. Overall, this traction method helps to simplify the operation process and reduce operation time. Furthermore, this method makes it easier to identify bleeding during the procedure, which can be used to assure effective hemostasis and prevent postoperative complications (e.g., bleeding). When the tumor is completely resected, it also helps to facilitate tumor recovery to prevent the tumor tissue from entering the abdominal cavity before retrieval.
Footnotes
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (81502000,W2015JZC12) and a grant from the Shanghai Committee of Science and Technology (15ZR1406800,15DZ1940202,16DZ2280900)
Disclosure Statement
No competing financial interests exist.