
Abstract
Abstract
Background:
Laparoscopic common bile duct exploration (LCBDE) is used to treat choledocholithiasis. Flexible choledochoscopy is usually performed; however, this instrument is fragile and liable to breakage.
Materials and Methods:
Data were collected and reviewed retrospectively from a prospectively maintained database. All cases of attempted LCBDE with the rigid ureteroscope at the institution since January 2014 were included. Demographic characteristics, preoperative attempted endoscopic retrograde cholangiopancreatography (ERCP), size of the bile duct, findings at laparoscopy, use of drain or T-tube, conversions, and morbidity or mortality were documented.
Results:
A total of 37 patients were identified. The median age was 51 years (32–71). The male to female ratio was 1:5. Twenty-eight patients had failed ductal clearance at ERCP (75.7%). The mean common bile duct (CBD) diameter was 11.4 mm (10–13.5). There were five conversions. Cirrhosis in 2 patients, bleeding in 1 patient, impacted stone in 1, and equipment failure in 1. T-tubes were placed in 5% of cases. N = 8 (21.6%) of the patients had a Mirizzi syndrome. Average hospital stay was 4 days (3–7). Two patients had complications postoperatively—bleeding and collections.
Conclusions:
LCBDE using the rigid ureteroscope is feasible. It can be performed with acceptable morbidity. Use of the rigid ureteroscope represents a good alternative to the flexible choledochoscope with high duct clearance rates. One disadvantage is cirrhosis where the scope may not be negotiated into the CBD due to a stiff liver. It is a viable option when preoperative ERCP has failed to clear the CBD.
Introduction
C
Laparoscopic cholecystectomy was the next major step in the management of patients with gallstones. The majority of surgeons were not comfortable with laparoscopic common bile duct exploration (LCBDE); hence the popular approach of laparoscopic cholecystectomy combined with preoperative or postoperative endoscopic retrograde cholangiopancreatography (ERCP). This approach allowed for the procedure to be completed laparoscopically; however, the disadvantages were a two-stage procedure requiring two anesthetic procedures, as well as procedure specific morbidity related to ERCP. 5
It has been demonstrated that it is possible to clear CBD stones with a single stage procedure with acceptable morbidity and mortality.6–10 The most commonly used methods are transcystic where the CBD is not dilated and transductal if the CBD is dilated >10 mm. A transductal approach requires the ability to suture laparoscopically, as well as a choledochoscope. The majority of centers use a flexible instrument, which is liable to damage the flexible glass fibers. The fiberoptic choledochoscope is composed of thousands of densely packed flexible glass fibers. There are lenses both proximally and distally, and if the glass fibers themselves are damaged the delicate instrument is rendered useless.
The purpose of this study is to review the cases of LCBDE performed at our institution, Dr George Mukhari Academic Hospital (DGMAH) which is a tertiary academic center North West of Pretoria in South Africa. The focus of the study is on the technique of LCBDE using the rigid ureteroscope. The primary end point was feasibility and duct clearance rate, and the secondary end points were morbidity and mortality.
Materials and Methods
Ethics clearance was obtained from the institutional review board, and this is the clearance number SMUREC/M/243/2015. The study was registered on research registry UIN number 3561.
We queried our prospectively maintained database for all patients that underwent LCBDE where a rigid ureteroscope was used at DGMAH between January 2014 and December 2017. We included patient demographic data, operative findings, postoperative and intraoperative complications, conversion rate, retained CBD stones, and mortality.
Mean (±standard deviation) was presented for continuous variables, and frequencies (%) were presented for categorical variables. Continuous variables were tested for normality, and if normal, t-tests are used and if not normal, nonparametric tests are used. For our primary analysis, linear regression is used to model the association between X and Y, adjusting for a, b, and c. For secondary analysis examining the presence or absence of logistic regression is used adjusting for a, b, and c. A P value of <.05 was considered significant. All analyses were performed using IBM SPSS 22 software.
The preoperative evaluation involved routine laboratory and ultrasound examination, including determination of serum amylase, bilirubin, aspartate aminotransferase, alkaline phosphatase, and γ-glutamyl transferase. LCBDE is performed for cases in which CBD stones can be confirmed with associated dilatation of the CBD on ultrasound or magnetic resonance cholangiopancreatography.
Inclusion criteria: patients with choledocholithiasis and dilated CBD.
Exclusion criteria: patients with a narrow CBD; unstable patients; patients who were offered a flexible choledochoscope; and patients who had a successful clearance using an ERCP.
Operative procedure
The surgical procedure was carried out in the anesthetized patient in the supine position with 30 degrees of reverse Trendelenburg. Video monitors are placed on the right side of the patient toward the head. Pneumoperitoneum was obtained by open Hassan technique infraumbilically and set at 14 mmHg. A 30 degree angled laparoscope was introduced. Under direct vision three further trocars are introduced: 10 mm in epigastrium this port should be to the right of the falciform ligament to facilitate access and alignment to the CBD, 5 mm right subcostal midclavicular line, and 5 mm midaxillary 2 cm below right costal border (Fig. 1).
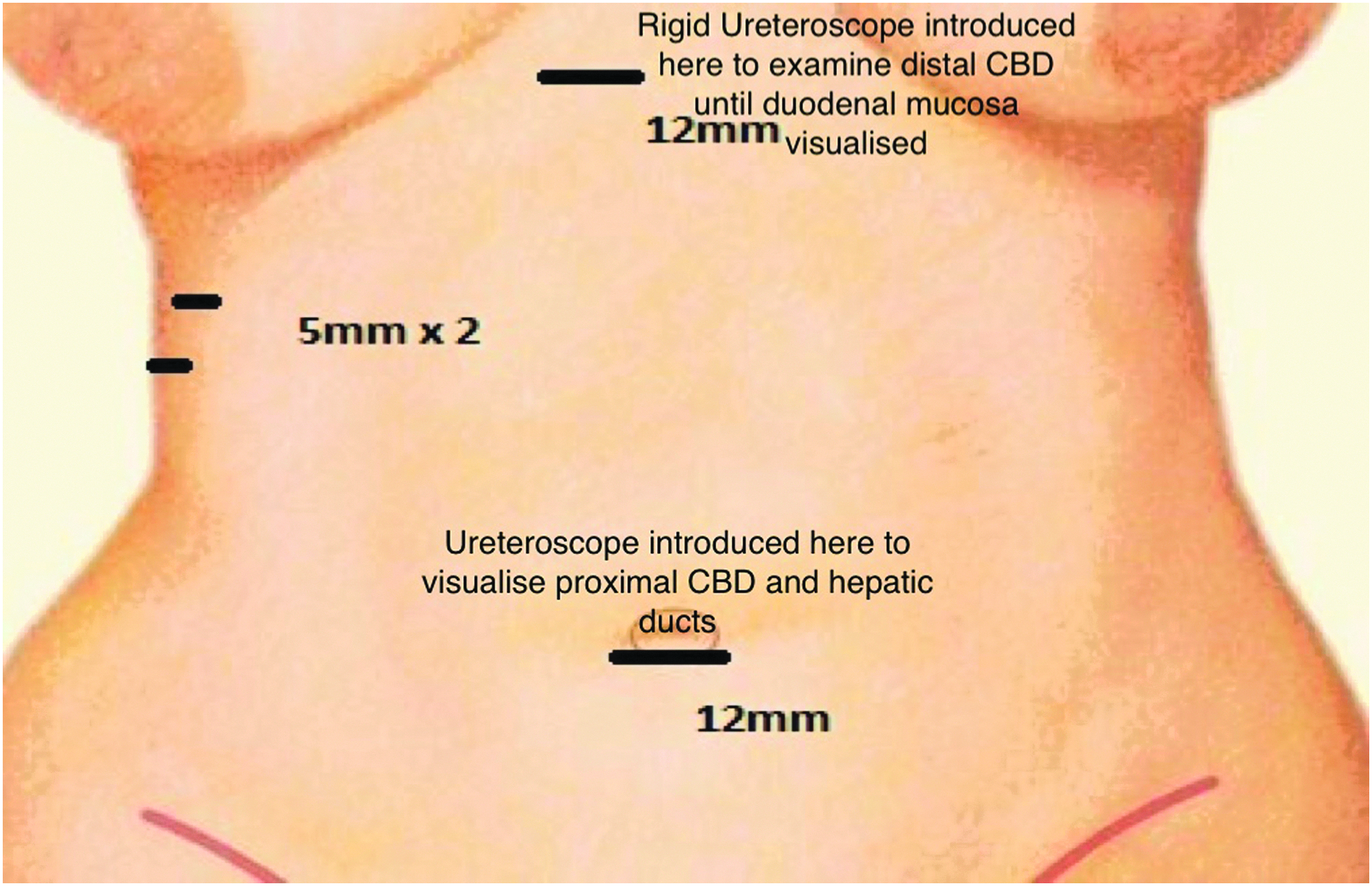
Port sites. CBD, common bile duct.
Dissection of Calot's triangle was carried out, and cystic artery and duct were clipped and ligated if possible but left attached. In the case of Mirizzi syndrome, a gallbladder flap is performed. The CBD was opened at 12 o'clock position using a longitudinal choledochotomy using diathermy initially and subsequent cold dissection; stay sutures are placed at the margins of the choledochotomy. The choledochotomy is 1–1.5 cm in length in the supraduodenal CBD (Fig. 2). A 7F rigid ureteroscope from Karl Storz™ was introduced through the epigastric port into the distal CBD. As the gallbladder is still attached traction on the gallbladder can be used to manipulate the axis of the CBD to facilitate examination using the rigid ureteroscope. Continuous saline irrigation distends the CBD further. Stones are removed by gently manipulating the scope that passed the stones and leveraging the stones out of the choledochotomy.
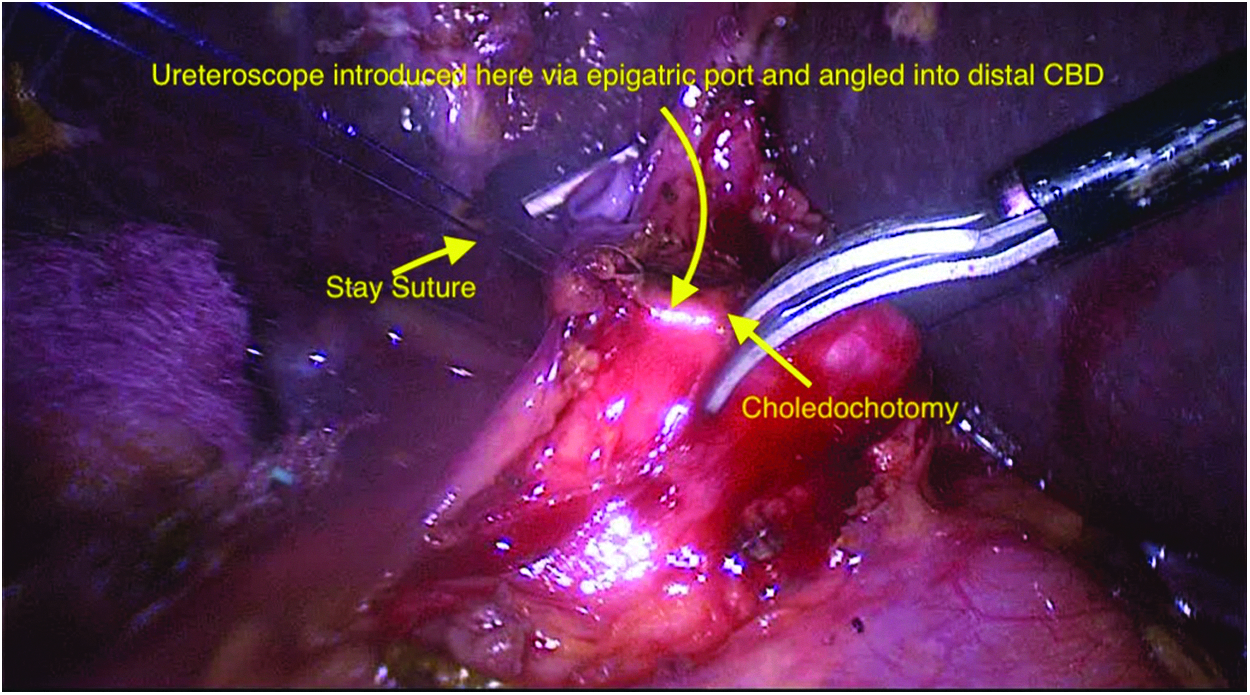
Choledochotomy with stay sutures. CBD, common bile duct.
The CBD is confirmed to be cleared using direct visualization of the duodenal mucosa (Fig. 3). The ureteroscope is also directed proximally using the umbilical port; care is taken not to traumatize the CBD epithelial lining. This allows visualization of the right and left hepatic ducts, as well as the second-order bile ducts (Fig. 4). The surgeon can also use a large fogarty catheter to clear further stones; if the patient had an ERCP preoperatively, stones can be pushed distally using the rigid scope into the duodenum. The choledochotomy is closed with 4-0 PDS II sutures (Ethicon, Inc., Somerville, NJ) in a continuous over-and-underlocking manner. T-tubes were used earlier in the operative experience, and a Penrose Silastic drain was placed in the subhepatic space.
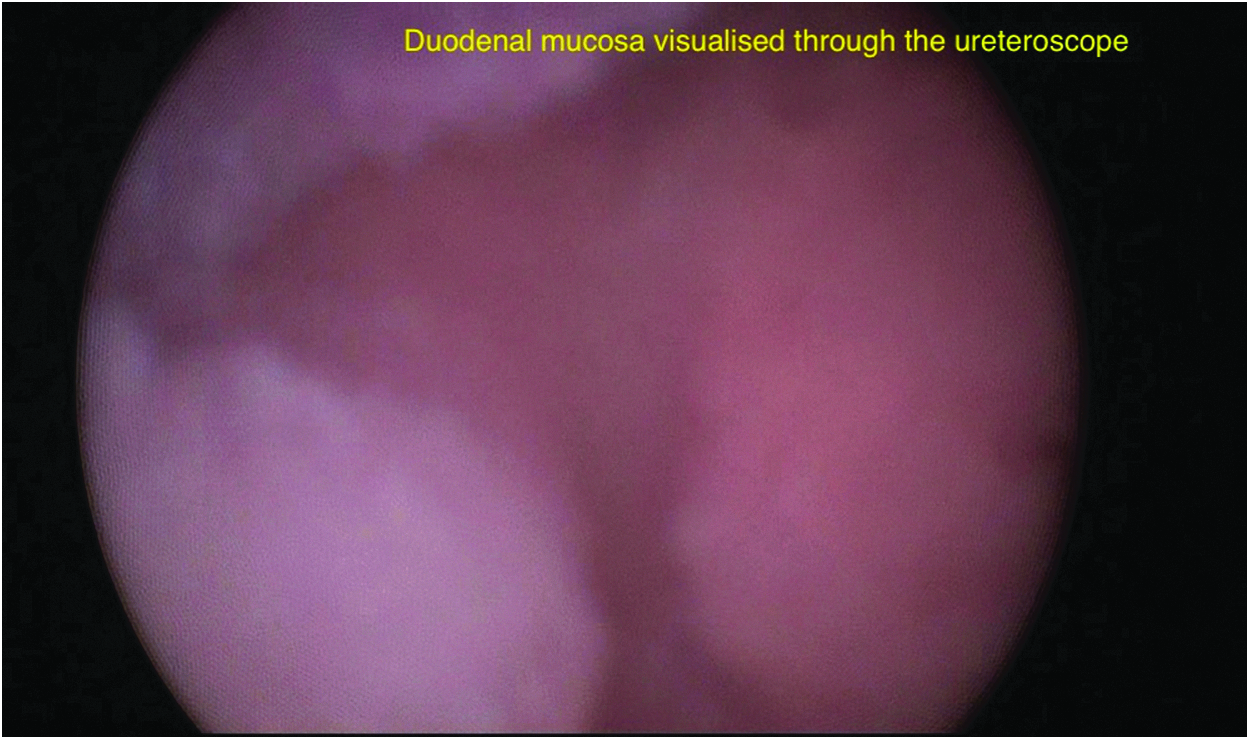
Duodenal mucosa viewed through ureteroscope.
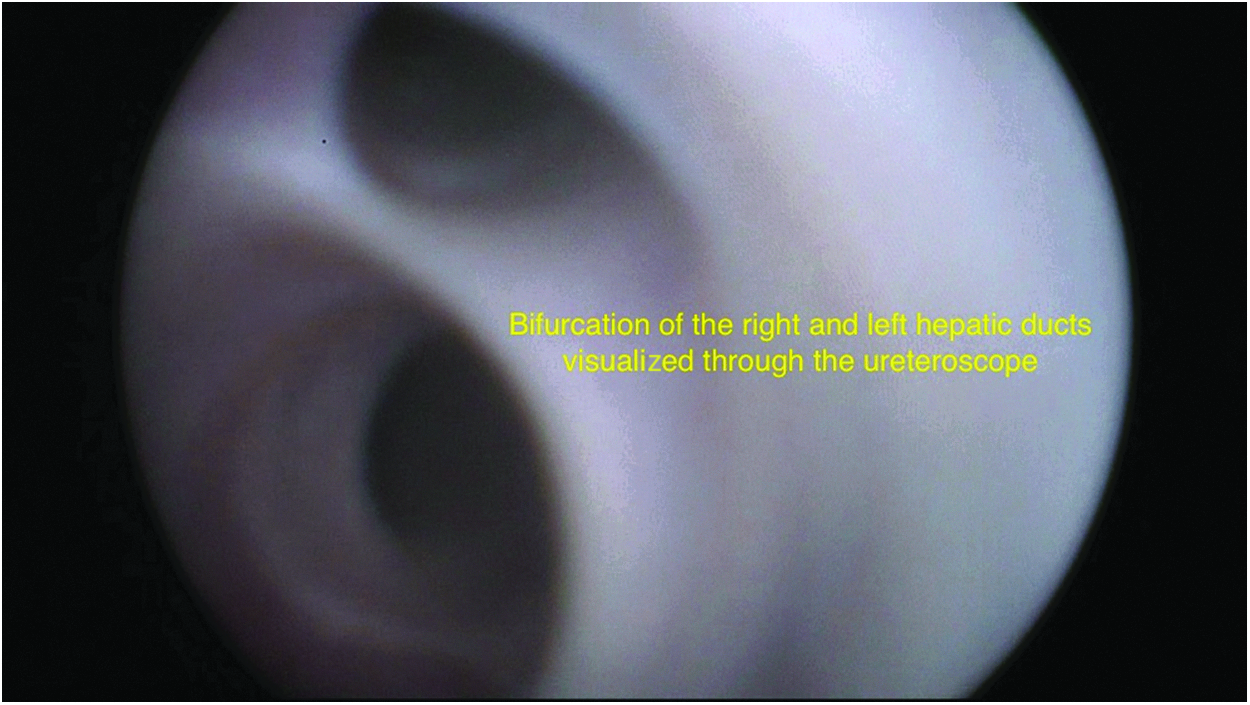
Bifurcation of the hepatic ducts viewed through the ureteroscope.
Results
From January 2014 to December 2017, LCBDE was performed on 37 patients. The mean age of the patients was 51 years (32–70). Thirty-one (83.8%) of the patients were female. These patients all had confirmed choledocholithiasis with a dilated CBD >10 mm (Table 1).
Of these patients n = 28 (75.7%) had failed duct clearance at preoperative ERCP, and the remainder was taken primarily for LCBDE.
The mean CBD diameter was 11.4 mm (10.5–12.3). The procedure was completed successfully in 32 (86.5%) of the cases; conversion was required in 5 cases (13.5%).
One patient was converted due to equipment failure where the irrigation system failed, 2 patients had liver cirrhosis, and the CBD exploration could not be completed due to inability to manipulate the rigid scope into the CBD due to the stiff liver; this was impossible even after converting to open exploration. Two patients were converted due to impacted stones that were impossible to remove; these were large stones that were successfully cleared at open surgery.
Mirizzi syndrome was noted in n = 8 (21.6%) of the patients; these patients were treated successfully laparoscopically using a gallbladder flap.
A T-tube was used in 8 of the cases (21.6%); these were used earlier on the operative experience.
The procedure was completed successfully with four ports in n = 27 (84.4%) cases; the remainder required additional port.
Mean operating time was 212 minutes (127–423).
Mean hospital stay was 4 days (3–9).
Morbidity occurred in 3 patients (8.1%), 1 had cholangitis plus severe pneumonia and developed a bed sore in intensive care unit, the second had a bile leak post LCBDE, required washout and stenting through ERCP route, and the third which had multiple collections post LCBDE was relooked and washed out, but no bile leak was noted.
There was no procedure related mortality.
Discussion
Choledocholithiasis is found in 10%–15% of patients operated on for symptomatic cholecystitis.11,12 Intraoperative cholangiogram was first performed by Mirizzi in 1931. 12 The introduction of endoscopic sphincterotomy by Japanese and German surgeons as an alternative to open CBD exploration occurred in the 1970s.13,14 This was considered to be the state of the art in managing gallstone disease and its complications. With improvement in laparoscopic technique and equipment, as well as better preoperative diagnostic tools, LCBDE became possible for CBD stone. There are four possible approaches as follows: transcystic, transcystic choledochotomy, laparoscopic choledochotomy, and laparoscopic antegrade sphincterotomy.15–18
The main disadvantages related to endoscopic clearance of CBD stones relate to the fact that it requires two or three separate episodes of anesthesia for the patient. This puts strain on scarce resources. Morbidity is related to post ERCP pancreatitis, bleeding, and perforation of the duodenum. The morbidity is ∼7% and mortality 0.2%–2.3%. In view of these problems ERCP is now indicated only in specific cases when (1) the patient shows signs of cholangitis, (2) stones are diagnosed in the postoperative phase, (3) adverse factors prohibit the surgery, and (4) a limitation in technical ability or equipment renders the LCBDE unfeasible.19–21
Exploration of the CBD with laparoscopy and choledochoscopy has proven to be efficient, safe, and well accepted by patients because two different pathologic conditions are solved in a single surgical procedure. Access through choledochotomy is indicated for patients with a dilated CBD (>10 mm), with large stones or multiple stones. An 86.6% success rate was reported in our series and in previous series 90% success rate. 22 In our series 75.7% of the patients had failed ductal clearance at preoperative ERCP and 21.6% of the patients had Mirizzi syndrome; these represent challenging cases to perform LCBDE on. Also our series is unique in demonstrating exclusively the use of the rigid ureteroscope.
The main challenge with LCBDE is the large impacted stones that cannot be managed with the use of a flexible choledochoscope as it has narrow working channel, and instruments like graspers cannot be negotiated through it. To break stones through a flexible choledochoscope, it is necessary to apply a holmium laser 23 or an electrohydraulic lithotripter 24 ; accessories that are very expensive and not available in most of the developing world. This prompted us to attempt a novel technique using the rigid ureteroscope.
The previous work was looking at LCBDE used a rigid nephroscope, which is larger than the ureteroscope. These articles also reported that the technique is safe, with high duct clearance rates. It was feasible, and the nephroscope allows for passage of grasper which is useful for crushing impacted stones. However, a larger choledochotomy is required, and this prompted us to analyze our results using the smaller rigid ureteroscope.25,26
A large series analyzing the outcomes of laparoscopic common bile duct exploration using a flexible choledochoscope have reported excellent results. The conversion rate was 5% overall in their series. In our series the conversion rate was 13.5%. The overall rate of duct clearance was similar in both studies. The reason for the slightly increased rate of conversion in our study was related to the stiffness of the liver and inability to manipulate the scope into the distal CBD with a cirrhotic liver. This represents one disadvantage of the rigid ureteroscope. The other reason for conversion was impacted stones. Our institute does not have access to a holmium laser or a frequency-doubled dual-pulse Nd:YAG (FREDDY; World of Medicine, Berlin, Germany) laser lithotripsy. If this was available some of the impacted stones could have been fragmented and subsequently cleared decreasing the conversion rate. 27
The rigid ureteroscope is readily available, and it is a robust instrument. Vision through the rigid nephroscope is excellent. It confirms clearance of the CBD of stone reliability. In our series where the procedure was completed successfully, the duct clearance rate was 100% with no missed stones. Stones can also be pushed distally using the ureteroscope. It is also a far more robust instrument and is less liable to breaking than the flexible choledochoscopes as it does not have the delicate fiberoptic fibers, which can be crushed when handled with the laparoscopic graspers rendering an expensive piece of equipment useless.
Conclusions
Our study demonstrates that LCBDE using the rigid ureteroscope is a valuable technique to obtain ductal clearance in patients with a dilated CBD either primarily or where ERCP has failed. The technique is safe without major morbidity or mortality and is feasible. The main disadvantage of the rigid scope is in the rigid cirrhotic liver where the scope may fail to manipulate distally into the CBD.
Footnotes
Acknowledgment
This work was undertaken in partial fulfillment for the Edinburgh Specialist Surgical Qualification.
Disclosure Statement
No competing financial interests exist.