
Abstract
Abstract
Objective:
To determine the effectiveness of treatment via laparoscopic approach and to present the long-term outcomes in patients with isolated renal hydatid cyst.
Materials and Methods:
We reviewed the data of 11 patients who underwent laparoscopic treatment for isolated renal hydatid cyst between March 2004 and January 2017. Demographic characteristics and clinical, laboratory, and radiological findings of cases were examined. Mann–Whitney U and t-test were used in statistical analysis.
Results:
The mean age of the patients was 36.7 years (25–51). The common complaint of the patients was lumbar pain and 9 patients had a palpable mass. It was identified that serologic evaluation of Echinococcus granulosus was positive in 5 patients. The mean cyst size was determined as 72 mm (40–150). The mean operation time was 128 minutes (120–150) while the length of hospital stay was 4 days (3–13). Perioperative major complication was not observed in any of the patients. The levels of hematocrit and creatinine were measured, 37.8 (26–43) and 0.93 (0.5–1.3), respectively, in the postoperative period, while these levels were 39 (26–45) and 0.90 (0.5–1.3) in the preoperative period and there was no statistically significant difference (P > .05). The mean follow-up time was 84 months (40–166). No relapses were observed in any patients.
Conclusions:
The treatment of renal hydatid cyst disease with laparoscopic approach is a safe and effective method. There was no recurrence in any of the patients in the long-term period. Further studies including a large series of patients are needed.
Introduction
E
Hydatid is a larval form of Echinococcus granulosus, its primary host is dog, and intermediate hosts are mainly sheep and cattle. Occasionally, humans may be intermediate hosts. Renal involvement alone is rare, as most parasites are seized by hepatic or pulmonary filters during the circulation. Renal involvement constitutes 2%–3% of cases. Kidney involvement may occur alone or in conjunction with other neighboring organs. The involvement area in the genitourinary system is almost always the kidney, but prostate, bladder, and epididymal involvement can be observed very rarely.3–5
The vast majority of hydatid cysts grow very slowly and can remain still for years without any clinical signs. It can be difficult to diagnose because of late symptoms and their different presentations.
The general approach in the surgical treatment of renal hydatid cyst disease is cyst excision with conservation of the renal parenchyme. 6 A wide range of treatment options are in the literature extending from conventional open surgical to minimally invasive approaches. Scolicidal agent injection, marsupialization, percutaneous drainage, cystectomy, and partial or total nephrectomy are applied techniques. Studies of case reports demonstrating the applicability of laparoscopic approach as a surgical treatment alternative to the hydatid cyst treatment have taken place in the literature with the increase in laparoscopic experience.7–11 In this study, we aimed to present the outcomes and complication rates of patients diagnosed with hydatid cyst in the kidney and treated with laparoscopic approach.
Materials and Methods
Between March 2004 and January 2017, records of 11 cases diagnosed with isolated renal hydatid cyst and treated with the laparoscopic approach at our clinic before being tracked in the postoperative period were retrospectively evaluated. Demographic characteristics, complaints, and clinical, laboratory, and radiological findings of cases were examined. The indirect hemagglutination (IHA) test was used as a laboratory test, while ultrasound and computed tomography (CT) were used as a radiological imaging method for cyst hydatid disease. The radiological results of the patients were classified in accordance with the 2001 World Health Organization (WHO) classification system.
Albendazole (15 mg/kg/day) treatment was applied to patients 4 weeks before the operation. Before the operation, the evaluation of response to medical treatment was carried out by control ultrasonography (US). No regression was detected in the radiological evaluation in patients whose medical treatment was initiated before the operation. Albendazole (15 mg/kg/day) treatment was continued with 4-week intervals after the operation. Oral treatment was applied three times with 14-day intervals. Postoperative complications were classified according to the Clavien classification. 12 Patients were evaluated by radiological and laboratory findings during follow-up.
This study was designed retrospectively and all patients signed an informed consent agreement. Ethics committee approval was not applied because of retrospective design.
The data were analyzed with the Statistical Package for the Social Sciences v. 16 (SPSS, Inc., IL). The Mann–Whitney U and t-test were used in statistical analysis. A P-value of less than .05 was considered statistically significant.
Surgical technique
Patients were operated with the transperitoneal laparoscopic approach for renal hydatid cyst. Under general anesthesia, the kidney and cyst were totally mobilized with the help of a 12 mm, a 10 mm, and two 5 mm trocars. Gas buffers soaked with three 10% povidone/iodine solutions were inserted into a 12 mm trocar and placed surrounding the cysts and kidneys. The cyst was identified. The Veress needle was placed directly into the cyst from a different point to drain cyst contents first, and then, 20% serum was injected and reaspirated to reduce the intracystic pressure.
The cyst wall was opened and the liquid content was aspirated. At this stage, the endoscope was inserted into the cystic mass and checked if the female cyst remained. Cystic cavity was repeatedly irrigated with 20% hypertonic solution. Finally, the cyst wall was excised as an en-block, detached from the cavity without damage to the integrity of germinative and laminar membranes, and taken out of the abdomen with an endobag. Scolicidal agent-impregnated buffers were also removed from the abdomen using the endobag. The operation was terminated by placing an aspirative drain into the cavity.
Results
Of the 11 patients, 3 were females (27.3%) and 8 were males (72.7%), and the mean age was 36.7 years (25–51). All of the cases presented to our clinic with complaints of lumbar pain, and 9 patients (81.9%) had a palpable mass identified on physical examination (Table 1). Four of the cases (36.4%) were localized in the left kidney, and 7 (63.6%) were in the right kidney. The average size of the cyst was 72 mm (40–150). CT findings on radiological evaluation and ultrasound findings classified in accordance with the 2001 WHO classification are given in Table 2. When laboratory parameters at the clinic were evaluated, it was detected that the IHA test was positive for E. granulosus in 5 cases (45.5%). All patients except 1 were diagnosed with cyst hydatid disease preoperatively.
ASA, American Society of Anesthesiologists classification; HCT, hematocrite.
2001 WHO classification of hydatid cysts is used to assess the stage of renal hydatid cyst.
CE, cystic echinococcosis; CL, cystic lesion; CT, computed tomography; WHO, World Health Organization.
The mean operative time of the cases was 128 minutes (120–150), while the length of hospital stay was 4 days (3–13) (Table 3). No perioperative complication was observed in the patients. Mean blood loss was measured as 38 mL (22–53). The levels of hematocrit and creatinine were measured as 37.8 (26–43) and 0.93 (0.5–1.3), respectively, in the postoperative period, while these levels were 39 (26–45) and 0.90 (0.5–1.3) in the preoperative period, and there was no statistically significant difference (P > .05). One patient who was not preoperatively diagnosed with hydatid cyst was considered to have symptomatic simple cyst and was taken into surgery. During operation, a renal hydatid cyst was detected and the procedure was completed successfully on this patient by following the preoperative general principles explained earlier. The postoperative complication rate in our patients was 27.3%.
HCT, hematocrite.
Postoperatively, 2 patients developed high fever with grade 1 complication according to the Clavien classification, and paralytic ileus with grade 2 complication in 1 patient. These patients recovered after medical treatment and follow-up process. Oral albendazole treatment was applied for 28 days preoperatively, and then, the treatment was repeated three times for 4 weeks with 14-day intervals in the postoperative period and terminated. Hepatotoxicity due to medical treatment did not develop. During the follow-up, patients were evaluated according to laboratory tests and radiological findings (US and CT). During the average follow-up period of 84 months (40–166), none of the patients had any complication or relapses (Fig. 1).
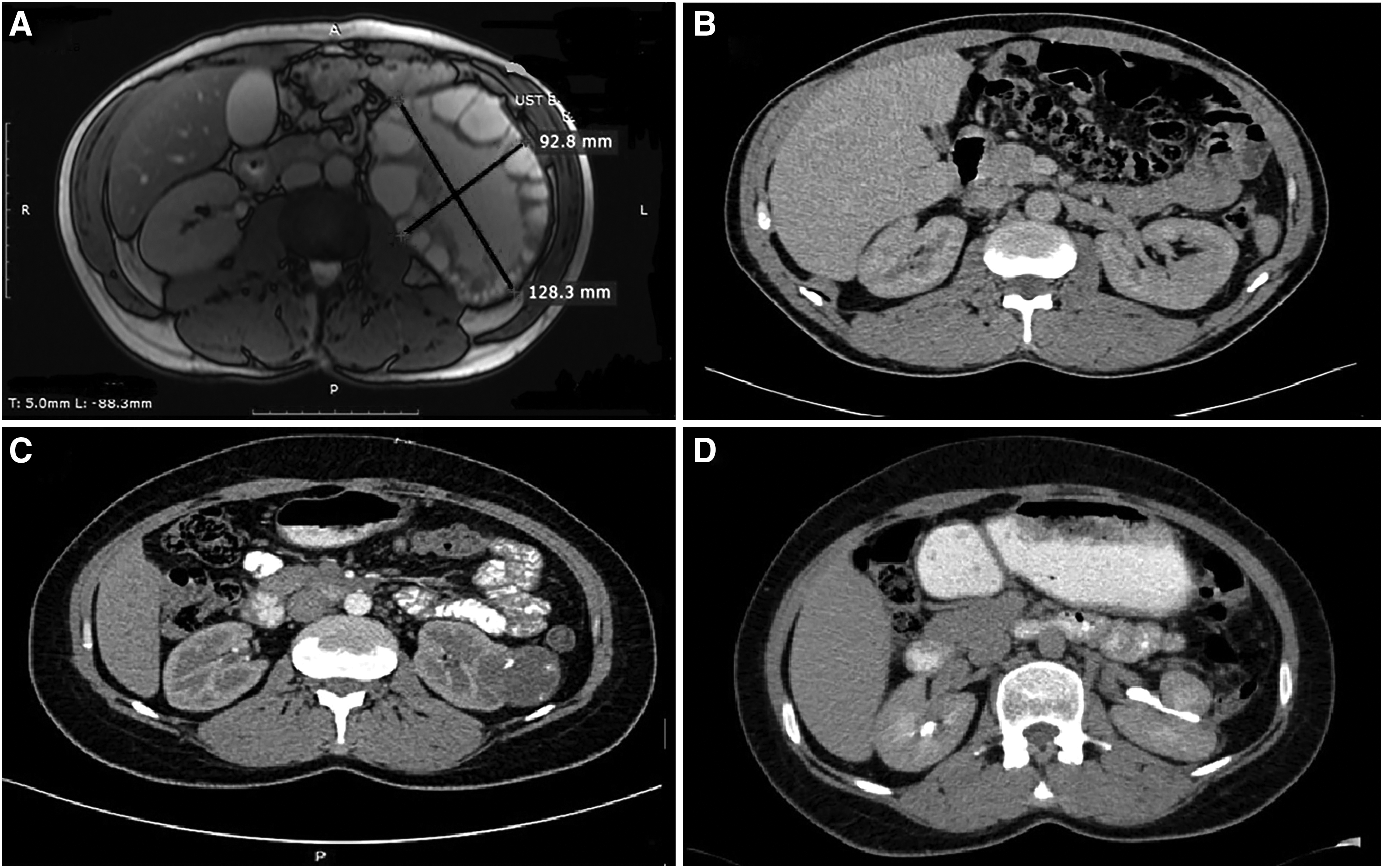
CT images of 2 patients with preoperative and postoperative periods.
Discussion
Kidney protection in surgical treatment should be the primary goal in patients diagnosed with renal hydatid cyst in the preoperative period. The cysts located in the liver and lungs can occasionally be treated medically with albendazole and mebendazole. 4 However, there are no data available on medical treatment of hydatid disease of the kidney. Surgical treatment modalities include scolicidal agent injection, marsupialization, percutaneous drainage, simple cystectomy, and total nephrectomy. Studies in the literature show the success of open surgical treatment of renal cyst hydatid. 13 Hence, surgical treatment with laparoscopic approach is still controversial.3,4 However, case reports stating that the laparoscopic approach to uncomplicated hydatid cysts is a safe and effective method have been indicated in the literature.7–11
When presented case reports were examined, unroofing, pericystectomy, partial nephrectomy, or nephrectomy was performed with laparoscopic approach in renal cyst hydatid.7–11,14 To the best of our knowledge, this study is the broadest patient series in renal hydatid cyst disease studies, including midphase follow-up results, treated with the laparoscopic approach in the literature. Laparoscopic approach has been successfully applied to all of our patients and no intraoperative complications have been observed.
Since the renal hydatid cyst does not have specific indications or symptoms, the disease may remain asymptomatic for years and cyst sizes can reach large dimensions (10–15 cm). 4 The most frequent symptoms are palpable mass, hematuria, blunt pain, and hydatiduria. All of our patients had pain complaints. In 9 of our patients (81.8%) with large cyst size, a palpable mass was found on physical examination. One of our cases presented with fever, while another with an occasional hematuria. No hydatiduria, which was pathognomonic for hydatid cyst diagnosis, was found in any of our patients.
The Casoni intradermal test, routinely used in the diagnosis of hydatid cyst in the past, has been replaced by serological/immunological tests. For this purpose, complement fixation test, latex agglutination test, IHA test, counter immunoelectrophoresis, immunosorbent assay with hydatid fluid and antigen 5, and immunoelectrophoresis with thermodynamic arc-5 lipoprotein precipitation are used today. The IHA test is a serologic test with the highest sensitivity (75% sensitivity). However, it should be noted that false negative results due to circulating immune complexes or false positive results due to other parasitic infections can be observed. 15 In our series, 5 of the cases (45.5%) were positive at the IHA test for E. granulosus.
CT identifies calcifications and female vesicles easier in the preoperative diagnosis of renal hydatid cysts. It also provides more detailed information on urinary tract and extrarenal involvement. 4 The diagnosis of hydatid cyst in our cases was made by US and CT in addition to laboratory findings in radiological evaluation. Besides being the most commonly used system, the WHO classification system classifies hydatid cysts into different species based on ultrasound imaging. The distribution of our cases according to this classification is given in Table 2. After suspicious appearance on conventional ultrasound, it should be assessed with CT. It should not be forgotten that the sensitivity and specificity of CT in hydatid cyst are high.
Typical findings of renal hydatid cyst on CT imaging include (1) unilocular cysts with a calcified rim occasionally associated with membrane detachment or (2) multilocular heterogeneous cysts that occasionally contain daughter cysts of lower density than the maternal matrix. 16 Seven of our cases had a first type CT appearance, while 3 cases had second type. However, in every case, CT may not be sufficient to establish final diagnosis. The general approach should be based on clinical evaluation as well as immunohistochemical findings and radiological evaluation. As a matter of fact, in our study, 1 patient was considered to have a symptomatic simple cyst and an operation was decided, but the diagnosis of renal hydatid cyst was not made before the operation.
Despite serological tests and having significant imaging techniques, the diagnosis of renal cyst hydatid cannot be made in 1/3 of the patients before the operation. 5 Also, in our case, renal hydatid cyst was diagnosed during the operation and the surgery went well. As for other patients, these patients also did not develop any perioperative complications.
There are many techniques described in literature for the surgical approach to renal hydatid cyst disease. These may include cystectomy and omentoplasty, partial nephrectomy, nephrectomy, laparoscopic cystectomy, and laparoscopic partial nephrectomy/nephrectomy.3–5,7–11 Controlled drainage of cystic content and washing with a scolicidal solution before open cystectomy reduce the possibility of allergic reaction and seeding/recurrence. Partial nephrectomy can be considered as a treatment option in small and peripheral lesions, in cysts suspected to be associated with the collecting duct system and uncertain diagnosis.3,4 Nephrectomy is a commonly used treatment method in cases in which preoperative evaluation is incomplete. General principles in open surgery are also applied in laparoscopic approach.
Basiri et al. applied laparoscopic partial nephrectomy to the patients with renal hydatid cyst disease. 7 The cyst and renal parenchyma were intertwined in their cases, and the authors decided laparoscopic partial nephrectomy. Rabii et al. performed laparoscopic treatment with the retroperitoneal approach to prevent the patient from abdominal cavity contamination. 14 In our opinion, the laparoscopic retroperitoneal approach may be preferred in cases without giant hydatid cysts, however, the transperitoneal approach will be more appropriate when it is large or giant sized as in our series. Although there is a risk of intraperitoneal contamination, if carefully applied, the transperitoneal approach provides a better workspace for the operating surgeon.
Preoperative antihelmintic agent is effective to sterilize cyst contents. In addition, the first trocar entry with the open Hasson technique is a protective factor to prevent leakage from the cyst. Except for 1 case in our series, oral albendazole treatment was initiated before the operation, and hypertonic sodium chloride was used as an intraoperative scolicidal agent. In any case, no allergic reaction or anaphylactic shock developed.
In the literature, the number of studies involving complications is rather limited and in general, no postoperative complications have been observed in studies with case reports. Adventitia layer hemorrhage of the cyst is the most common complication in open surgeries. 3 No bleeding complications were observed in our study. In the postoperative period, according to the Clavien classification, 2 patients developed high fever with grade 1 complication, and paralytic ileus with grade 2 complication in 1 patient. No abscesses or collections were observed in patients. After the necessary conservative treatment, all 3 patients were discharged without any problems.
It has been emphasized that preoperative oral albendazole or mebendazole therapy reduces the risk of relapse and can shrink the cyst, which can facilitate intraoperative manipulation. 17 However, the length of medical treatment in renal hydatid cysts in the preoperative and postoperative period is not identified definitely in the literature. There is no consensus on this subject. It is rational to give adjuvant therapy as a medical treatment besides surgical treatment. 1
The general approach is to initiate medical treatment before the operation and continue for at least 1 month (for albendazole) or 3 months (for mebendazole) after the operation. 18 Similarly, Creţu et al. suggested multimodal treatment to patients who underwent minimally invasive procedures for hydatid disease. 19 They started oral albendazole at least 1 month before surgery and continued for 3–6 months postsurgery, according to the situation of the cyst during surgical intervention. In our study, oral albendazole treatment, which was started preoperatively, was applied in 3 courses of treatment for 4-week intervals with 14-day breaks. Hepatotoxicity due to medical treatment did not develop in our patients, who were monitored with laboratory and radiological findings.
There is no study in the literature reporting local recurrence in the treatment of renal hydatid cysts. When we take a look at the studies addressing the laparoscopic treatment of hydatid cysts of the liver, in cases where laparoscopic cystectomy applied, as it is known that pericystic scolex is not involved, there are many studies showing that pericystectomy reduces recurrence and some of the authors suggest this technique, which is relatively more radical than cystectomy and pouch shrinking.
Ozden et al. also applied pericystectomy with a laparoscopic retroperitoneal approach to their patient to avoid risk of intraperitoneal contamination. 8 We did not apply pericystectomy in our series. Nevertheless, we did not observe recurrence in any of our patients during the follow-up period. In fact, this subject is rather mentioned in the literature and recurrence/relapse rates are unknown. In this regard, we think that our series will contribute to the authors.
Although this is the first study reporting the outcome and complication rates of laparoscopic treatment of renal hydatid cyst disease, our study has several limitations. The data were collected longitudinally and verified retrospectively, which could have introduced error. Another limitation of our study was we did not compare the technique with open surgery. However, we performed the general principles of open surgery to prevent spillage during the procedure. Despite these limitations, our results suggest that laparoscopy is a safe and effective treatment in the management of isolated renal hydatid cyst disease. Future studies should be prospectively designed to overcome existing limitations.
Conclusion
In conclusion, parenchymal protective surgical approaches are the main approach in renal cyst hydatid disease. This study, which includes outcomes of laparoscopic transperitoneal treatment of renal cyst hydatid disease, revealed that the laparoscopic approach involving open surgical principles is applicable in this patient group and is also effective in the long term. We believe that further studies involving a wider series of patients will raise the level of evidence for this result.
Footnotes
Disclosure Statement
No competing financial interests exist.