
Abstract
Abstract
Introduction:
Intraoperative pneumothorax may complicate surgery by obscuring surgical view and cause cardiorespiratory instability during fundoplication with large hiatus hernia. Proactive intraoperative treatment may reduce conversion and drain insertion and facilitate timely completion of surgery.
Materials and Methods:
The authors present effective surgical and anesthetic measures to alleviate pneumothorax, which are helpful for hemodynamic stability and surgical visibility.
Conclusion:
Pneumothorax can complicate surgery by reducing surgical vision and causing cardiorespiratory instability. There is no requirement for laparoscopic or intercostal drainage. The authors provide various techniques to control intraoperative pneumothorax.
Introduction
D
Materials and Methods
Intraoperative pneumothorax has been treated in multiple different ways in a large single-surgeon practice of laparoscopic antireflux surgery. Pneumothorax appeared most frequently in treating very large hiatus hernia/paraesophageal hiatus hernia (PEH). 1
Anesthetic management
The occurrence of pneumothorax in the elderly patient population with multiple comorbidities, in the head up position, may compromise cardiorespiratory function during anesthesia, causing sudden onset of hypotension, tachycardia, or bradycardia. 1 Such an occurrence frequently required returning the operating table to level and aspiration of carbon dioxide (CO2) from the pleural space until the patient's hemodynamic situation stabilized. Pressors, atropine, and other agents were often necessary in a population group with a potential for cerebral ischemia. Management with intravenous arterial monitoring was valuable, allowing instantaneous detection of deteriorating blood pressure and facilitating early corrective intervention, which often appeared suddenly.
Surgical management
Identification and preservation of the pleura can prevent damage (Fig. 1); when the pneumothorax occurs, it is frequently visible as a rent in the pleura. The experienced surgeon will often instantaneously recognize a pleural breach and communicate this to anesthetics prior to the development of obvious pneumothorax and physiological deterioration (Fig. 2). Otherwise pneumothorax may appear as convex movement of the diaphragm or bulging on ventilation of the mediastinal pleura, frequently obscuring vision, and making dissection of the vagal nerves and posterior esophageal structures more difficult. Flattening the table and aspirating CO2 are time consuming and temporary in nature, which requires further surgery performed at lower pressures with less adequate visualization. Avoidance of this situation is greatly advantageous in ease of surgery, potential for complications, and duration of surgery.
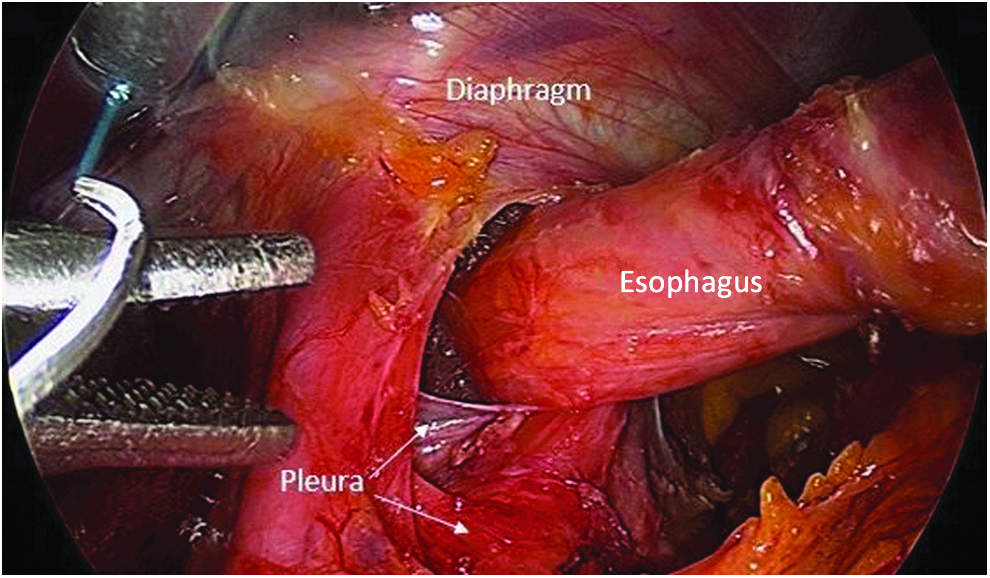
Pleura: in the midline behind the esophagus.
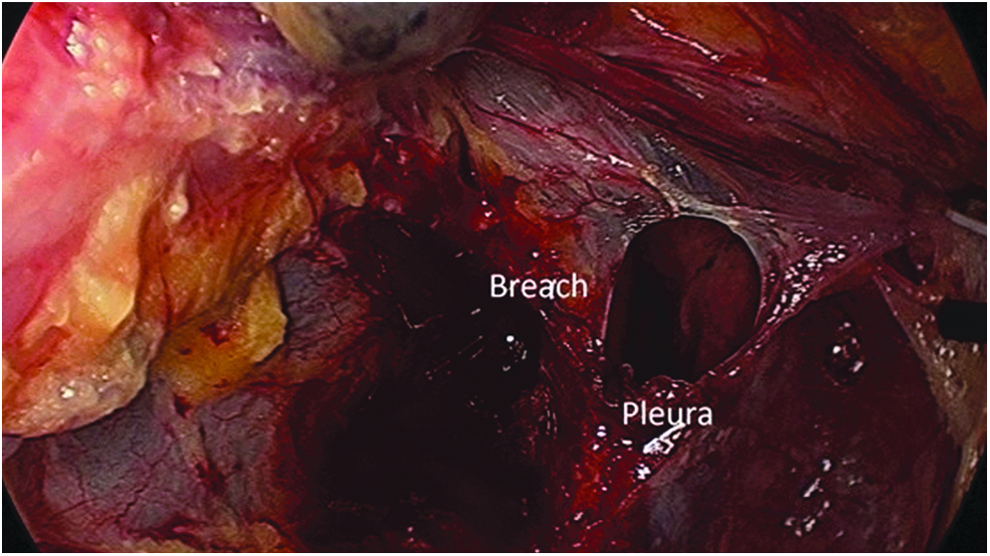
Pneumothorax: circular breach in the pleura with lung in background.
In our experience, as this condition occurred more commonly during surgery of PEH, however, dissection within the mediastinum emphasizing identification and preservation of the pleura decreased the incidence of inadvertent pneumothorax. Pleura was closely applied to the esophagus and often crossed the midline posteriorly. It was necessarily closely applied to the hernia sac and reduction of the hernia sac could pull the pleura into the operative field. Dissection of fatty tissue on the mediastinal surface of the sac and sweeping it back toward the lung helped preserve pleura. Absolute hemostasis aided vision of the pleura, for which harmonic scalpel was found highly useful (Johnston & Johnston Medical, Cincinnati, OH).
Multiple techniques were utilized to occlude pleural breach including PDS Endoloop (Fig. 3) (Ethicon Endo Surgery, Cincinnati, OH), a piece of hernia sack (Fig. 4), clips, hemostatic mesh gauze (Fig. 5), or V-lock suture (Covidien, Dublin, Ireland) (Fig. 6) for larger defects (Figs. 1–5). Occasionally two techniques may be combined.
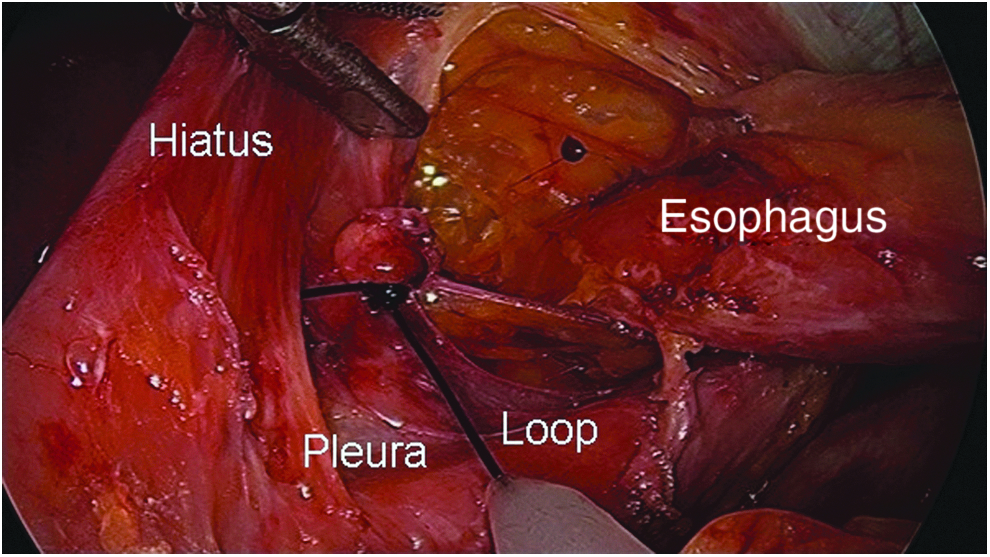
Loop closure: PDS loop around breach in posterior right pleura.
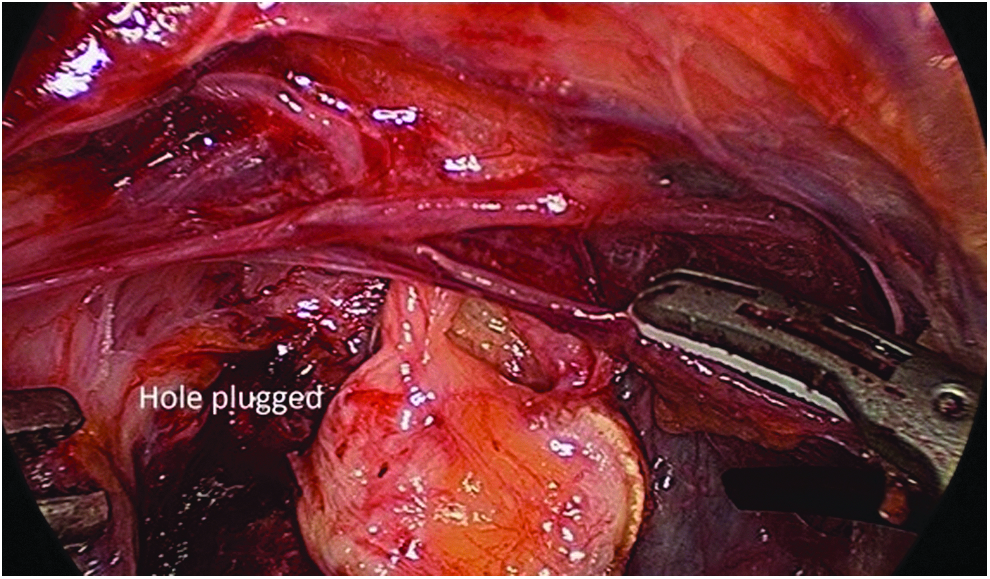
Fat pad closure: small pleural defect “plugged” with sac material.
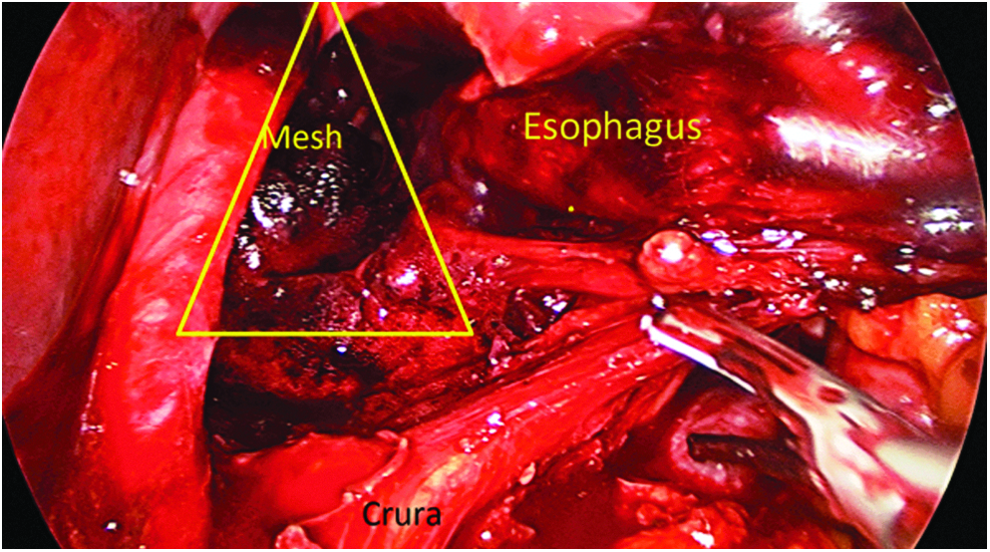
Surgical mesh: wet mesh placed over a pleural breach.
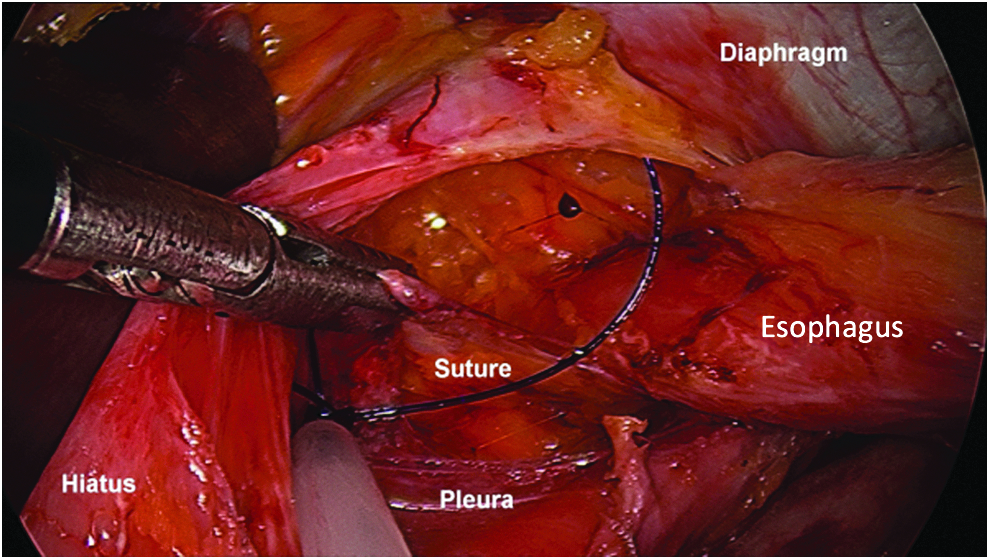
V'lock suture: closure.
The loop was utilized if a small hole could be easily grasped by the forceps and drawn into the loop. Alternatively, a large piece of hernial sac with minimal fat on it was “pasted” over the defect. Large amounts of fat in the mediastinum are avoided due to previous experience of fat necrosis causing a fibrotic esophageal stricture. Clips or a hemostatic sponge can work. Should one technique fail, an alternative can be sought. A large rent may be closed with barbed suture. Once closure is obtained, rapid lung re-expansion occurs as the CO2 is reabsorbed.
Results of the Technique
All techniques were advantageous allowing better vision, stabilization of hemodynamic situation, and almost complete intraoperative resolution of the pneumothorax without necessity to decrease instillation pressure of CO2. At completion of the case, a valsalva maneuver was performed with mediastinal suction and abdominal suction to remove the majority of the CO2. Rapid resorption of small residual pleural gas amounts was then expected. Patients were returned to the recovery ward where chest X-ray was performed only if oxygen saturation was reduced after a period of 30 minutes of observation or there was respiratory or hemodynamic instability. No chest drains were required and no patient required open surgery after laparoscopic pneumothorax occurrence.
Conclusion
Although avoidance of pneumothorax is desirable and dissection with close attention to the pleural reflection advantageous, occasional breaches occur. Hemodynamic instability can be rapid. Early surgical treatment of this defect is desirable and adequate anesthetic monitoring necessary.
It has not been necessary to convert or pleurally drain any patient since this approach has been performed. Some authors2–4 have recommended heroic management of intraoperative pneumothorax, including intercostal catheter and even thoracotomy. We have not found this to be necessary before intraoperative management and rapid seal of any defect has been technically easy and facilitates surgical exposure and timely completion of surgery.
Footnotes
Disclosure Statement
The authors declare no conflict of interest.