
Abstract
Abstract
Background:
Laparoscopic D3 anterior posterior extended mesenterectomy (D3APEM) in right colectomy has received increased attention. The aim of this study is to prove feasibility, systemize technical accomplishment, and provide short-term outcomes data.
Methods:
From July 2013 to February 2017, 18 patients with adenocarcinoma in the right colon underwent right colectomy with laparoscopic D3APEM, including lymph nodes anterior and posterior to the superior mesenteric vessels. A reconstructed three-dimensional anatomy map derived from the staging computed tomography was used as a road map at surgery. The procedure was systematized into seven operative steps: Step 1, trocar placement and inspection; Step 2, release of the transverse colon; Step 3, identification of the terminal mesenteric vessels; Step 4, release of the anterior flap; Step 5, division of the transverse mesocolon; Step 6, release of the posterior flap; and Step 7, anastomosis and specimen removal. Patient disposition and variations regarding vascular anatomy and ability to expose consequentially may necessitate a variation in the sequence of the steps.
Results:
A total of 7 (39%) cases were converted, 3 due to bleeding and 4 due to challenging dissection. Median operative time and blood loss were 276 minutes (168–439 minutes) and 200 mL (< 50–1300 mL), respectively. Postoperative complications occurred in 6 (33%), including 2 (11%) major complication requiring reoperation. Median hospital stay was 5 days (3–13 days). R0 resection was achieved in all cases. Median number of the lymph nodes harvested was 40 (25–86), including 11.5 (4–35) in the D3 volume. Six patients (33%) had positive nodes, 3 of them affecting the D3 zone, including 1 case of a skip metastasis. There was no mortality, and at present all the patients are alive. One patient developed distant lymph node metastases.
Conclusion:
Laparoscopic right colectomy with D3APEM is feasible, associated with acceptable morbidity and fast recovery; now in readiness for introduction in specialized colorectal institutions.
Introduction
R
Advances in minimally invasive surgery enabled safe laparoscopic colorectal resection.3–5 A few publications reported D3 mesenterectomy performed through laparoscopic approach; however, these reports have not demonstrated lymphatic dissection posterior to the superior mesenteric vessels.6–9 The question of lymphadenectomy along the superior mesenteric artery (SMA) still remains unresolved.
The aim of this study is to prove the feasibility and provide short-term outcomes data of laparoscopic right colectomy with extended D3 mesenterectomy supported by a preoperatively reconstructed three-dimensional (3D) anatomy map derived from the staging abdominal computed tomography (CT) angiography, used as a road map during surgery. Systematization of the procedure and exploration of its pitfalls were the secondary aims of this study.
Materials and Methods
Eighteen patients with adenocarcinoma in the right colon underwent laparoscopic right colectomy with extended D3 mesenterectomy at three collaborating Norwegian institutions—Akershus University Hospital, Lørenskog; Oslo University Hospital—Rikshospitalet, Oslo; and Vestfold Hospital, Tønsberg from July 2013 to February 2017 (16 of these patients from January 2016 to February 2017). Procedures were performed by either R.G., B.E., or D.I. as main operators. All cases were guided by DI to provide standardized approach to extended D3 mesenterectomy. Extended D3 mesenterectomy included removing all lipolymphatic tissue surrounding the superior mesenteric vessels from 5 mm cranial to the middle colic artery (MCA) origin to 10 mm caudal to the ileocolic artery (ICA) origin. Dissection included removal of lipolymphatic tissue posterior to the superior mesenteric vessels in contrast to a standard D3 mesenterectomy. All procedures were guided by preoperative 3D vascular reconstruction of abdominal CT-angiography, providing crucial data on relationships between the arterial and venous branches of the superior mesenteric vessels (Fig. 1). 3D reconstructions of vascular anatomy were performed by B.V.S. at the Anatomy Sector, Faculty of Medicine, University of Geneva (Geneva, Switzerland) as previously described. 10 Basically, the CT data sets underwent segmentation through the 3D volume rendering technique, using the FDA-approved Osirix MD ver. 8.5.2 64-bit software (Pixmeo, Bernex, Switzerland). The software kit included region of interest, multiplanar reconstruction, maximal intensity projection, polygon, pencil, and length tools. The CT data were further analyzed through Mimics Medical ver. 19.0.0.347 and 3-matic Medical ver. 11.0.0.109 software, both Windows 7 ultimate edition x64 2016 (Materialise NV, Leuven, Belgium). The tools implied were thresholding, multiple slice editing with interpolation, region growing, 3D LiveWire, morphology operations and Boolean operation, as well as 3-matic measurements—distance, length, and radius.
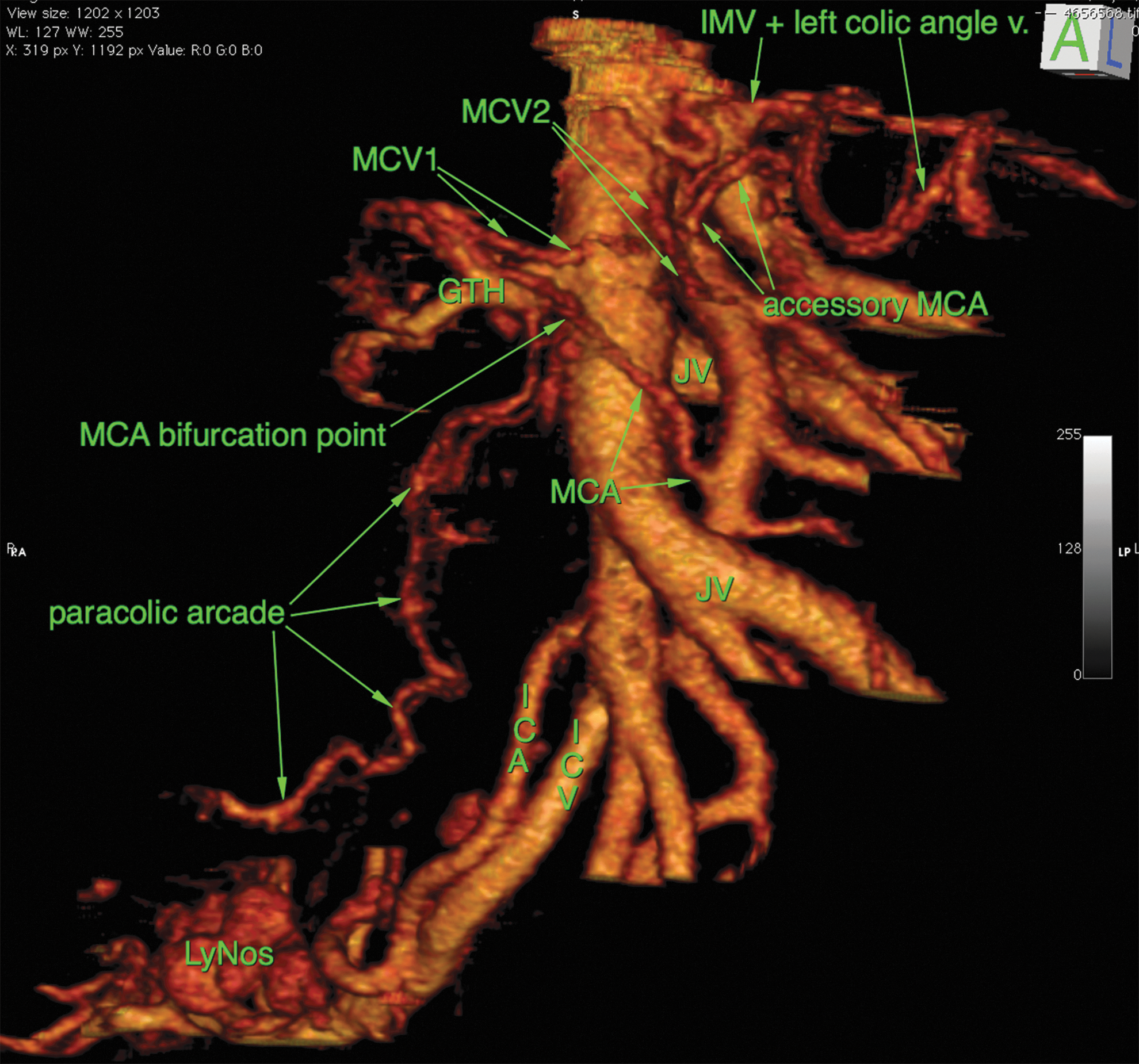
Three-dimensional reconstruction of the superior mesenteric vessels and their branches.
The standard preoperative investigations included spiral CT of the abdomen and the thorax, and analyzing the level of carcinoembryonic antigen. The patients received perioperative subcutaneous low-molecular weight heparin. Intravenous anesthesia was used. At the end of surgery, bupivacaine hydrochloride was injected at the trocar port sites.
Postoperative analgesia consisted of a nonsteroidal anti-inflammatory drug and intravenous paracetamol. Fast-acting opioids were given if additional analgesia was required. The patients were encouraged to mobilize early and resume feeding as soon as it was tolerated. Epidural anesthesia was not administered to these patients. To reduce postoperative lymphorrhea, the patients were advised to consume low-fat food for a period of 3 days. 11 If lymph was not detected in the drain fluid (triglycerides, cholesterol, and mononuclear cells), the drain was removed and the diet continued for 1 more day. After removal of the specimen, it was divided into the ileocolic specimen (containing the N1 and N2 lymph nodes) and the D3 area defined by a line positioned 1 cm to the right of the vascular sheath of the superior mesenteric vein (SMV), cranially bordered by the right branch of the MCA and caudally 1 cm distal to the ICA. 12 Tumor size was measured after specimen fixation in acetic acid during the histopathologic analysis of the resected specimens.
The unified criteria for grading perioperative adverse events were applied. 13 Intraoperative unfavorable incidents were assessed using the revision of Satava approach to grade surgical error, and postoperative complications were graded in agreement with the Accordion classification.14,15
Clinical data were collected from patient journals and registered in a prospective database. Patients' preoperative data are presented in Table 1.
ASA, American Society of Anesthesiologists.
Patients were routinely followed up at the outpatient clinic 1 month postoperatively, then every 6 months up to 36 months, and then every 12 months up to 60 months with clinical examinations, carcinoembryonic antigen assay, and spiral CT of the abdomen. CT of the thorax was performed yearly. The duration of follow-up was median 20 (9–56) months. Chemotherapy was applied in accordance with recommendations from the Norwegian Gastrointestinal Cancer Group. None of the patients received neoadjuvant chemotherapy. Adjuvant chemotherapy was administered to patients with affected lymph nodes with either folinic acid/fluorouracil/oxaplatine (FOLFOX) or the fluorouracil/calcium folinate (FLF). Patient follow-up data were updated, and all research data were ready for analysis in November 2017.
Techniques
The procedure was systematized to seven operative steps: Step 1, trocar placement and inspection; Step 2, release of the transverse colon; Step 3, identification of the terminal mesenteric vessels; Step 4, release of the anterior flap; Step 5, division of the transverse mesocolon; Step 6, release of the posterior flap; Step 7, and anastomosis and specimen removal. Patient disposition and variations regarding vascular anatomy and ability to expose consequentially may necessitate a variation in the sequence of the steps. The procedure has several potential pitfalls specified in a following description of operative steps. See the 7 minutes Supplementary Video S1 (Supplementary Data are available online at www.liebertpub.com/lap) clip including key procedural steps.
Step 1: Trocar placement and inspection
We operate typically through 4 to 5 trocars placed in a semicircular manner. Pneumoperitoneum is established through a 12-mm optical trocar inserted at the left paramedian line at the level of the umbilicus under visual control to avoid intra-abdominal injury. Pneumoperitoneum pressure of 12 mm Hg is applied. Another 12 mm laparoscopic port is introduced at the midclavicular line just below the left costal arch. The third 5 mm trocar is placed subumbilical and the fourth 5 mm trocar in the right iliac fossa. Sometimes an additional fifth 5 mm laparoscopic port is positioned in the right flank. The abdomen is inspected to identify any presence of metastatic lesions.
Step 2: Release of the transverse colon
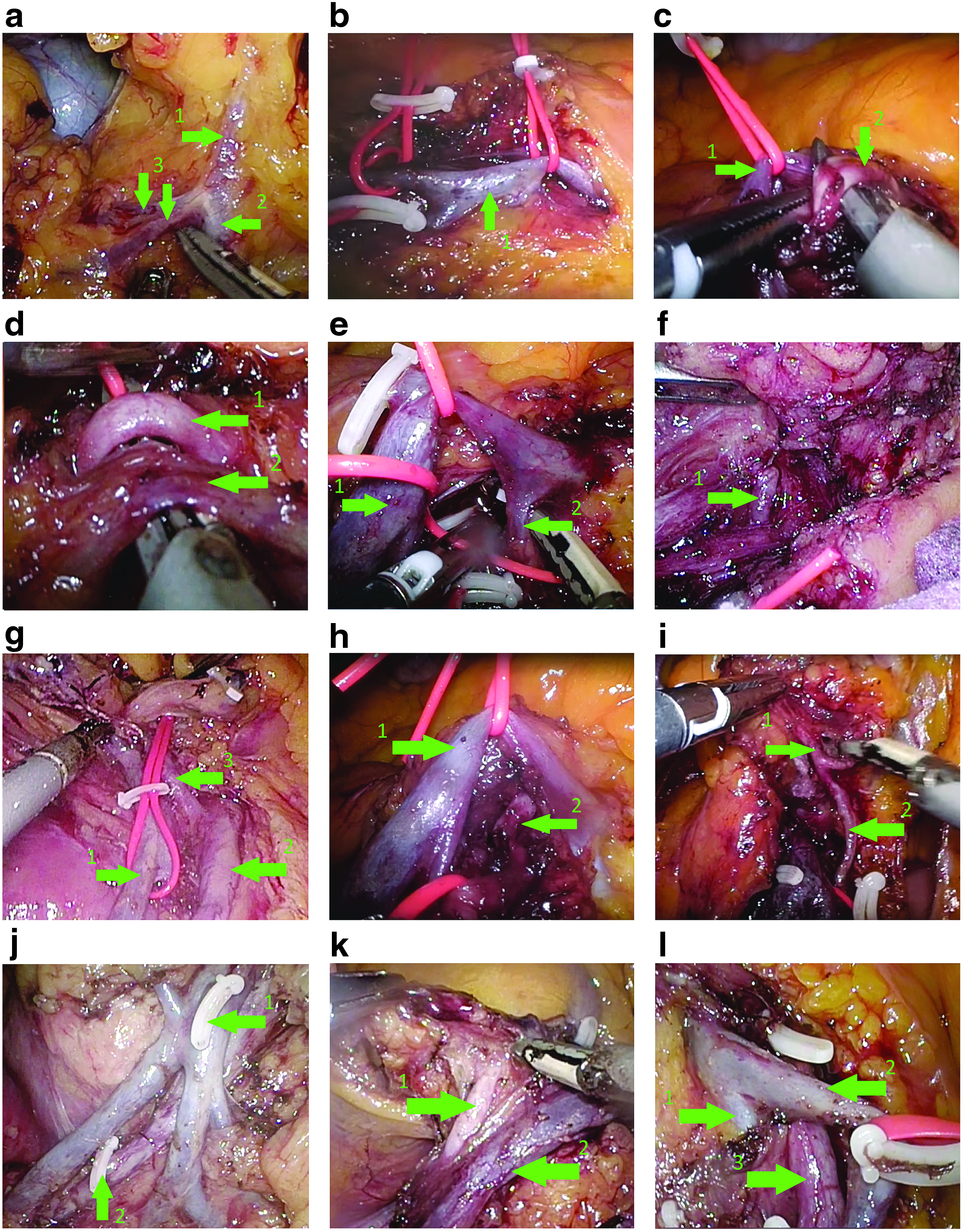
The gastrocolic ligament is divided caudal to the gastroepiploic vessels, thereby entering the lesser sac. The plane between the mesocolon on one side and the mesogastrium, pancreatic head, duodenum, and Gerota's fascia on the other side is developed while advancing toward the right colonic flexure. The gastroepiploic vein is dissected centrally, exposing the gastrocolic trunk and the SMV. The superior right colic vein is divided when present (Pitfall 1, Fig. 2a).
Operative pitfalls:
Step 3: Identification of the terminal mesenteric vessels
The transverse mesocolon is lifted cranially, the ileocolic vessels stretched, and a horizontal visceral peritoneum incision is made 1 cm caudal to the origin of the ileocolic vessels. The terminal ileal vein (TIV) is dissected free and secured in a vessel loop for manipulation or traction purposes (Pitfall 2, Fig. 2b). The terminal ileal artery (TIA) is found according to the anatomy reconstruction either behind the TIV or to its left; the arterial vascular sheath is opened and the vessel placed in a loop (Pitfall 3, Fig. 2c).
Step 4: Release of the anterior flap
Dissection continues along the vascular sheath of the TIA and the upcoming SMA to 5 mm proximal to the origin of the MCA (Pitfall 4, Fig. 2d). On occasion, large jejunal veins crossing anterior to the SMA must be honored and placed in vessel loops (Pitfall 5, Fig. 2e). The anterior flap, containing lymphatic and fatty tissue lying anterior to the superior mesenteric vessels, is then released. If the ICA or the occasional right colic artery is crossing anteriorly to the SMV, then these vessels must be divided at this time since their trajectory belongs to the anterior flap (Pitfall 6, Fig. 2f). After skeletonizing the SMV, the ileocolic vein can be ligated. The SMV vessel loop is lifted and the areolar tissue behind the SMV dissected, releasing it from the flap of tissue lying behind the superior mesenteric vessels, respecting the origins of jejunal veins or the much smaller pancreaticoduodenal veins (Pitfall 7, Fig. 2g). In this manner, the SMV is skeletonized and the anterior aspect of the vascular anatomy exposed, allowing for the clipping and division of the posteriorly crossing ICA or the occasional right colic artery (Pitfall 8, Fig. 2h).
Step 5: Division of the transverse mesocolon
After the MCA is placed in a vessel loop, lateral traction is applied so that dissection can continue along its vascular sheath to its point of division into right and left branches (Pitfall 9, Fig. 2i). After division of the right branch, the transverse mesocolon is divided to the planned level of resection on the transverse colon. At this stage, the bowel wall is skeletonized (including the division of the omentum majus) for later division. The confluence of the middle colic vein is found and divided between clips showing the pancreatic notch and its anterior surface (Pitfall 10, Fig. 2j). This segment of the procedure is simplified as a consequence of the previous release of the transverse colon.
Step 6: Release of the posterior flap
The terminal ileum is divided 15 cm proximal to the ileocolic junction. The paraintestinal vascular arcade is divided and then followed at its right-hand side toward the TIA, thereby dividing the mesentery. Dissection of the flap of tissue posterior to the superior mesenteric vessels is facilitated through traction of the SMV and the SMA vessel loop toward the left (Pitfall 11, Fig. 2k). This maneuver effectively transpositions the SMV and the SMA and also partially rotates the vessels, allowing the removal of the posterior flap containing lymphatic tissue and fatty tissue, by division along the left-hand side of the SMA. Jejunal–ileal arteries originating from the left side of the SMA can be injured at this point (Pitfall 12, Fig. 2l). The posterior flap is released through traction of the specimen to the right and the SMV to the left, and dividing all tissue adjacent to the vascular sheath of the SMA from 1 cm distal to the ICA origin to the level of the MCA origin, taking into consideration jejunal veins that may cross posterior to the SMA. The mesocolic plane is then followed laterally, thereby releasing the posterior flap completely from its dorsal adhesions over the pancreatic head and duodenum. The mesocolic plane is dissected laterally. The release of the specimen is completed by dividing the lateral peritoneal attachments.
Step 7: Anastomosis and specimen removal
Extracorporeal hand-sewn end-to-end anastomosis was applied mainly in initial cases through minilaparotomy, as well as in cases of conversions. Intracorporeal isoperistaltic side-to-side anastomosis was performed in later cases with help of Endo-GIA (Medtronic). The specimen was removed through a transverse suprapubic incision. The D3 area was separated from the specimen for selective pathologic examination. It is defined as the lipo lymphatic package constituting the anterior and posterior flap with a distal horizontal border 1 cm caudal to the origin of the ICA, a proximal horizontal border 5 mm cranial to the origin of the MCA, and a lateral border 1 cm lateral and parallel to the SMV.
Dissection instruments used were either Thunderbeat (Olympus, Tokyo, Japan) or LigaSure (Medtronic), reflecting institutional and/or personal surgeon preferences.
The final result after dissection of the D3 area is illustrated in Fig. 3.
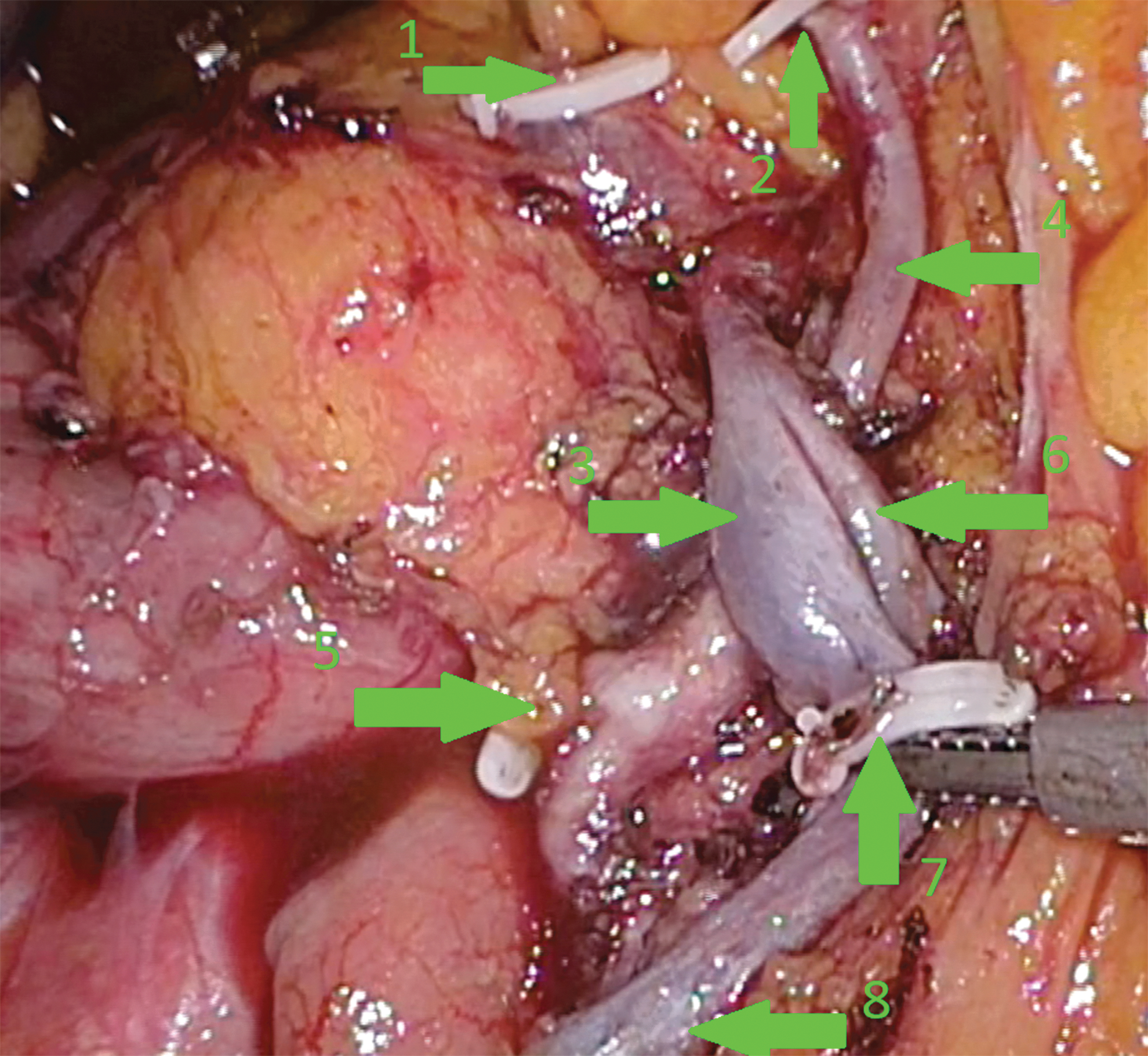
Final result after dissection of the D3 area: 1, stump of the gastrocolic trunk; 2, stump of the right branch of the MCA; 3, the superior mesenteric vein; 4, the MCA; 5, stump of ileocolic artery; 6, the jejunal vein; 7, stump of the ileocolic vein; 8, the terminal ileal vein. MCA, middle colic artery.
Statistics
The main data are given as median (range) or number (percentage) and presented in accordance with both the intent-to-treat concept and per protocol analysis. To illustrate a possible discordance between intent-to-treat and per protocol analyses, parameters were also presented as laparoscopically completed cases.
Ethical concerns
Patients with potentially curable right colon cancer were recruited from the “Safe D3 Right Hemicolectomy for Cancer through Multidetector Computed Tomography (MDCT) Angiography” trail, registered at clinicaltrials.gov (NCT01351714). All patients were required to sign a written consent form before inclusion. The study has ethical approval from the Regional Ethical Committee (REK Sør-Øst no. 2010/3354)
Results
Seven (38%) cases were converted, 3 due to bleeding and 4 due to challenging dissection. The hemorrhages included bleedings from the MCA, a jejunal branch of the SMA, and the TIV. The challenging dissections included difficulties to follow the terminal ileal vessels (in 2 cases), difficult dissection posterior to the SMA toward the MCA, as well as tedious search for the MCA.
Two patients had resectable liver metastases. The first patient was scheduled to combined procedure—left lateral sectionectomy followed by right hemicolectomy, whereas another patient was scheduled to right hemicolectomy first, then liver resection 2 months later.
Bleeding due to incidental injury to the splenic capsule necessitated splenectomy in 1 patient. This procedure was completed laparoscopically (bleeding—1300 mL, operative time 320 minutes). This injury was not related either to laparoscopic colectomy or to liver resection and happened due to incautious manipulation by the assistant.
Median operative time and blood loss was 276 minutes (168–439 minutes) and 200 mL (0–1300 mL), respectively. Perioperative outcomes are summarized in Table 2.
Postoperative complications occurred in 6 (33%), including 2 (11%) major complications requiring reoperation. Postoperative morbidity is listed and classified in Table 3. R0 resection was achieved in all cases. Median number of the lymph nodes harvested was 40 (25–86), including 11.5 (4–35) in the D3 zone. Six patients (33%) had positive nodes. In 3 patients, metastases affected the D2 zone only, in 2 cases, metastases affected both the D2 zone and the D3 zone, and in 1 case, metastases affected the D3 zone alone (so called skip metastasis). Oncologic parameters are summarized in Table 4.
There was no perioperative mortality. The postoperative hospital stay was 5 days (3–13 days). The majority of patients started to consume fluids and solid food on the day of surgery or on the first postoperative day.
Seven patients received adjuvant chemotherapy in the form of FOLFOX in 3 cases and FLF in 3 cases and in 1 case FOLFLOX was initiated but the chemotherapy regime was shifted to FLF due to intolerance of FOLFLOX. Then, 12, 11, and 6 cures were administrated in 3, 1, and 3 patients, respectively.
One patient, who initially received adjuvant chemotherapy with 12 FLF, developed distant lymph node metastases both intra-abdominally (para-aortic) and in the mediastinum initially diagnosed on a CT scan 8 months after operation. The metastases in the mediastinum were later confirmed by the endobronchial ultrasound-guided aspiration biopsy. This patient received supplementary chemotherapy treatment in the form of five FOLFLOX cures. She is alive 22 months after operation and the affected lymph nodes have decreased significantly in size, there are no signs of the development of new metastases on the control CT scan. Another patient with known resectable liver metastases at the time of colon surgery was operated with liver resection 2 months after primary resection. She underwent repeated two stage liver resection 1 year after primary resection due to metastatic recurrence. She has been symptom free thereafter.
Discussion
Laparoscopic approach for right colectomy with D3 mesenterectomy is challenging, requiring advanced laparoscopic skills as well as comprehensive 3D understanding of vascular anatomy.6–9 Laparoscopic surgery for colorectal cancer has been widely accepted as equal with regard to feasibility and safety compared with open surgery. 16
At the same time, the role of extended lymph node dissection has been in dispute for years, with many Asian surgeons believing that extended lymphadenectomy may lead to a survival benefit, whereas European and American surgeons have been inclined to doubt oncologic benefits while focusing on assumed high morbidity of more radical approach. 17 Even though there is reasonable anatomic and oncologic basis for extension of mesenterectomy and lymphadenectomy, there are no randomized controlled trials to state confident conclusions.17,18 Such a study focusing on survival would require hundreds of included patients in each arm and many years of follow-up. Thus, it is judged appropriate, while waiting for conclusive studies, to replace conventional D2 techniques with D3/complete mesocolic excision procedures in patients with otherwise expected long life expectancy in many institutions.
Encouraged by the improved survival after adoption of total mesorectal excision for the treatment of rectal cancer, many colorectal surgeons have attempted to develop new technical solutions to enhance oncologic outcomes after right hemicolectomy too. The concepts of complete mesocolic excision and D3 lymphadenectomy were developed.1,2 The surgical techniques needed to achieve these two concepts may be used without risk of compromising the best result of either concept. This is achieved by skeletonizing of the SMV and SMA in the D3 area and a central ligation of vessels feeding the colonic segment with special consideration of adequate colonic and mesenteric resection along the embryonic dissection plane. 19 In our series, this was the approach used.
A new era in evaluation of radicality of mesenterectomy and lymphadenectomy has started with the introduction of standardized histopathologic evaluation of surgical specimen as well as with laparoscopic access, enabling both intraprocedural precise visual control and postoperative documentation of the extent and quality of mesenterectomy and lymphadenectomy.20,21 The latter factor enables us to compare particular techniques applied in different institutions and reveals a considerable variation in interpretation of own techniques. There seems to be a frequent overestimation of actual extent of performed mesenterectomy and lymphadenectomy.12,22
We proved the feasibility and safety with regard to D3 anterior posterior extended mesenterectomy (D3APEM) with 11% major complication, none of them in the laparoscopically completed cases. Operative time for laparoscopic right D2 hemicolectomy corresponds to its open counterpart.16,23 However, operative time of reported laparoscopic D3 right hemicolectomy is higher than time reported for open D3 hemicolectomy.2,24 This may change with accumulation of experience. Median blood loss and operative time were 320 minutes and 100 mL in laparoscopically completed cases in our series. Blood loss in our patients is considerably lower than what is typically reported for open surgery, and corresponds to values reported by other groups with regard to laparoscopic D3 right hemicolectomy.6–9 Operative time in our series is higher than reported by other groups for laparoscopic D3 right hemicolectomy (133–244 minutes)6–9,23; however, our technique enabled harvesting 40 lymph nodes as a median value, including 12 in the D3 region. This corresponds to number of lymph nodes harvested in our open D3 right hemicolectomy series. The minimal number of harvested lymph nodes was 25 in total and 4 in the D3 region. All other reports of laparoscopic D3 hemicolectomy archived only 15–17 lymph nodes on average, except Liang and coauthors who reported about 34 harvested lymph nodes on average, including 6 in D3 region. 8 One of 3 cases (33%) with positive lymph nodes in the D3 region had a skip metastasis in our series. Similarly, Liang and coauthors reported 19.8% skip metastases in their series. These observations represent a strong factor in justification of the application of the D3 versus the D2 approach for right-sided colonic cancer. Harvesting of these lymph nodes safely is possible due to evasion of the pitfalls already described through preoperative awareness of the individual patient anatomy.
We believe that a reconstructed 3D anatomy map derived from the preoperative staging abdominal CT angiography, used as a road map at surgery, was a key to the supreme lymph node harvesting both in the D3 region and totally. This prerequisite to achieve truly complete D3 lymph node harvesting without considerable compromising of perioperative morbidity has been our routine since 2011. 25
The main challenges of performing laparoscopic D3APEM include the lack of tactile sensation and complicated anatomical variations in the relevant areas. Therefore, effective landmarks guiding the dissection are critical to keep the dissection secure. Intraoperative navigation with the help of 3D reconstructed anatomy may enable us to obtain a reliable perception of arteriovenous spatial relationship in the superior mesenteric tree. This is especially crucial due to the great number of known normal variations and vascular abnormalities.25–27 This allows us to ensure completeness of D3 lymph node harvesting regardless of complex vascular anatomy and especially with regard to the crossing pattern of the ICA. Dissection of lymph nodes located in the posterior ileocolic compartment is often performed inadequately. 28 The knowledge of relations regarding this compartment is simplified by the use of a 3D CT-derived anatomy map, and may enable to improve lymph node harvesting by up to five to six nodes.28,29 Laparoscopic access itself may improve exposure of the D3 region and vascular branching. In open surgery, it is sometimes difficult to completely expose the surgical trunk of the SMV, especially when patient is obese. Although it is known that obesity may slightly hamper laparoscopic operation, this factor is much more challenging in open surgery.30–33
In our series, we experienced a high rate of conversions, reaching 38%. The cases for laparoscopic surgery were not selected based on anatomical disposition, but rather on the availability of surgeons, that is there was not a selected group of patients. Besides, the threshold for conversion was low in this introductory stage. There were seven conversions, three due to bleeding and four due to challenging dissection. The MCA, the jejunal arterial branches, and the terminal ileal vessels presented major concerns. With accumulation of experience, we have observed reduction in operative time and conversion rate. However, it appears that a learning curve for lymphatic dissection in proximity of the mesenteric vessels is quite thorny compared with a learning curve for open lymphatic counterpart dissection. Therefore, the technical complexity of the procedure presents a limitation of this procedure. Inclusion of obligatory requirements for training in vascular dissection into a curriculum for residency in general surgery may contribute to better readiness of general surgeons to start technically complex vascular dissection in the mesenterial basin. In Norway, such obligatory training in vascular surgery has been a part of surgical curriculum for residents in general surgery during many decades; however, requirements and system of education in general and gastrointestinal surgery vary substantially in different countries worldwide. 34
The modern principle of oncologic radicalism has also been a desk strategy with regard to management of colorectal liver metastases in our institution. Presence of resectable colorectal liver metastases was not considered as a factor to omit application of laparoscopic D3APEM in our series, which is consistent with modern knowledge and trends in treatment of colorectal liver metastases.35,36 In our series, lymph nodes in the D3 zone were affected in 1 of 2 patients with synchronous colorectal liver metastases. This confirms that the choice of right colectomy with D3APEM was justified. Both patients are symptom free at 23 months of follow-up. However, further research is necessary to refine knowledge about association between presence of colorectal liver metastases and likelihood as well as potential location and extent of lymph node affection.
There is very scanty knowledge with regard to application of different laparoscopic energy devices. LigaSure, Harmonic Ace, and Thunderbeat have been on the market for many years and are at present the most used devices for laparoscopic dissection in colorectal and hepatopancreatobiliary surgeries in Western countries. However, few comparative studies have been reported, and all of them were of an experimental nature.37–39 Although Thunderbeat is advocated to provide faster dissection, procedures performed by Thunderbeat as main instrument failed to show this. Besides, the active branch of the instrument reaches a high temperature, which theoretically could transfer to a higher rate of intraoperative complications than LigaSure. Our series could neither confirm nor dismiss this assumption, we believe accurate dissection is possible with both Thunderbeat and Ligasure. One may deduce that choice of dissection instrument should be based on personal preference and experience.
This study showed rapid postoperative recovery with reduced need for postoperative pain medication and shorter postoperative stay (5 days as median) compared with reports for open surgery, despite the fact that laparoscopic D3APEM was associated with considerably longer operative time. Our hospital stay was half the time reported by other authors with regard to laparoscopic right D3 hemicolectomy (10–12 days). However, this corresponds to hospital routines in Norway with a tradition for shorter hospital stay than those typically seen for instance in China and Japan.6–9
A drawback of this study was a relatively small number of patients, and long-term data are not yet available.
Conclusion
This study suggests that, in cases of procedural guidance by preoperative 3D abdominal CT-angiography and standardized techniques, laparoscopic right colectomy with D3APEM is a feasible procedure associated with low morbidity and fast reconvalescence. This procedure is applicable for introduction in specialized colorectal institutions.
Documentation of extent and quality of dissection by means of high-resolution photography is highly advised to enable comparison of results with regard to completeness of D3 mesenterectomy since considerable variations in its interpretation exist in the colorectal surgical community.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.