
Abstract
Abstract
Aim:
To evaluate outcomes of surgical remediation for symptomatic or anatomic failure after a transoral incisionless fundoplication (TIF).
Methods:
This retrospective study was performed on 11 patients who underwent a remedial operation following TIF failure between June 2011 and September 2016 at the Mayo Clinic in Florida for persistent foregut symptoms. Upper gastrointestinal workup characterized 1 patient as having normal post-TIF anatomy and 10 as having anatomic failure. Ambulatory pH testing was performed in 7 patients and was abnormal in all. All patients underwent a laparoscopic takedown of the prior endoscopic fundoplication and removal of all accessible polypropylene T-fasteners.
Results:
All patients had esophageal salvage and have not required a reoperation. Anatomical findings included hiatal hernia (7), esophageal diverticulum (2), hiatal mesh erosion of esophagus (1), long-segment esophageal stricture (1), and normal anatomy (1). Remedial operations included laparoscopic explant of fasteners in all patients with conversion to fundoplication (7), resection/imbrication of esophageal diverticulum (2), Heller myotomy (1), and mesh explant and complex esophageal repair (1). Mean operative time was 177 minutes and median length of stay 3 days (range 2–13 days). At mean follow-up of 10.7 months (range 1–42 months), 7 patients had persistent complaints. Esophagogastroduodenoscopy was repeated in these 7 patients and was normal (n = 3), mild stenosis requiring dilation (n = 2), Los Angeles grade B esophagitis (n = 1), and Barrett's esophagus (n = 1).
Conclusion:
Anatomic distortion of the distal esophagus after TIF can be significant, making subsequent operations complex. After remedial surgery, few patients will continue to have troublesome symptoms such as dysphagia.
Introduction
G
In an effort to avoid operation and its potential complica tions, newer minimally invasive techniques for GERD have been developed. Transoral incisionless fundoplication (TIF, EsophyX; EndoGastric Solutions, Inc., Redmond, WA) is one such minimally invasive endoscopic technique for the management of reflux. The short-term outcomes of this technology seem encouraging. It affords some relief from reflux and a variable number of patients are able to stop PPIs.5,6,7 While Level I evidence is limited, one study suggests that 62% of TIF patients had elimination of regurgitation and extraesophageal symptoms compared with only 5% of patient on PPIs. 8 Hunter et al. in a prospective sham controlled trial randomized patients who underwent TIF versus those on omeprazole to assess its efficacy in treating regurgitation. 9 TIF was significantly more effective in eliminating regurgitation compared to PPI use (67% versus 45%, respectively), but 28% were categorized as symptomatic or TIF failures requiring reinitiating of PPI therapy (only 11% patients required PPIs at 3 months). No patient required another intervention. Available evidence suggests that TIF is more efficacious in controlling GERD particularly regurgitation, compared to PPIs in the short term.8,9
The intermediate-term outcomes of the TIF procedure are recently becoming available. Witteman et al. randomized 60 patients (40 TIF and 20 PPI) to evaluate its effectiveness in controlling GERD. 10 At 12 months, quality of life was significantly improved with TIF; normalization of distal acid exposure was achieved in 29%, but 61% of patients resumed PPIs. Testoni et al. followed 50 patients post-TIF for 6 years and reported that 86% of patients had stopped or halved their PPIs. 11 Hiatal hernia <2 cm, or absence of hiatal hernia, on preprocedure evaluation was noted to be a good prognostic factor.
Although the rate of anatomic failure of TIF is currently not known, there are few reports of surgical remediation for symptomatic or anatomic failure after TIF. Bell et al. reported a series of 28 patients who underwent a reoperation for TIF failure. Anatomic abnormality was noted in 75% on preoperative endoscopy. 12 We report herein our institution's experience managing patients with surgical remediation of symptomatic and anatomic failure after TIF.
Materials and Methods
Data were obtained by retrospective chart review of 11 patients with intractable foregut symptoms after TIF (EsophyX) who underwent surgical remediation between June 2011 and September 2016. All the patients had undergone the index TIF procedure at outside hospitals and were referred to our institution for recurrent symptoms. Five of these patients had undergone, under one anesthetic, a laparoscopic repair of hiatal hernia and TIF procedure. Two patients, after TIF-related perforation, had additionally undergone laparoscopic and open exploration with drainage, respectively. The patients (7 females and 4 males; mean age 56.9 years) underwent remedial operation after a median of 35.8 months (range 10–72 months) following TIF. Presenting symptoms included persistent reflux (n = 7), severe dysphagia (n = 5), and troublesome cough (n = 3). Contrast esophagram and esophagogastroduodenoscopy (EGD) characterized 1 patient as having normal post-TIF anatomy and 10 as having anatomic failure [hiatal hernia (n = 6), esophageal diverticula (n = 2), long distal esophageal stricture (n = 1), and erosion of polyester hiatal mesh into the distal esophagus and associated hiatal hernia (n = 1)] (Table 1). Ambulatory pH testing was performed in 7 patients and was abnormal in all. Esophageal motility study was obtained in 9 patients and revealed esophagogastric junction outflow obstruction/pseudoachalasia syndrome in 2.
HH, hiatal hernia; HHR, hiatal hernia repair; TIF, transoral incisionless fundoplication.
Patients were approached laparoscopically via standard five trocar placement for a Nissen. All patients underwent a takedown of the prior endoscopic fundoplication and removal of all accessible polypropylene T-fasteners, followed by upper flexible endoscopy to discern the anatomical landmarks. Patients undergoing conversion to fundoplication underwent hiatal closure with silk suture after mediastinal mobilization of the esophagus. Fundoplication was then performed over 54–56 F dilator. All patients underwent protocolized postoperative care, including postoperative contrast esophagram before initiation of liquid diet.
Results
There were no major perioperative complications and no mortality. Mean operative time was 177 minutes and median length of stay 3 days (range 2–13 days). Intraoperative findings included incorporation of the left crural pillar with at least one fastener in 8 patients. Five patients were found to have few inflammatory adhesions at the hiatus, however, 6 patients were found to have very dense adhesions. Of the 6 patients with dense adhesions, 5 had undergone prior surgical repair of hiatal hernia at the time of TIF procedure or post-TIF surgical exploration for a leak.
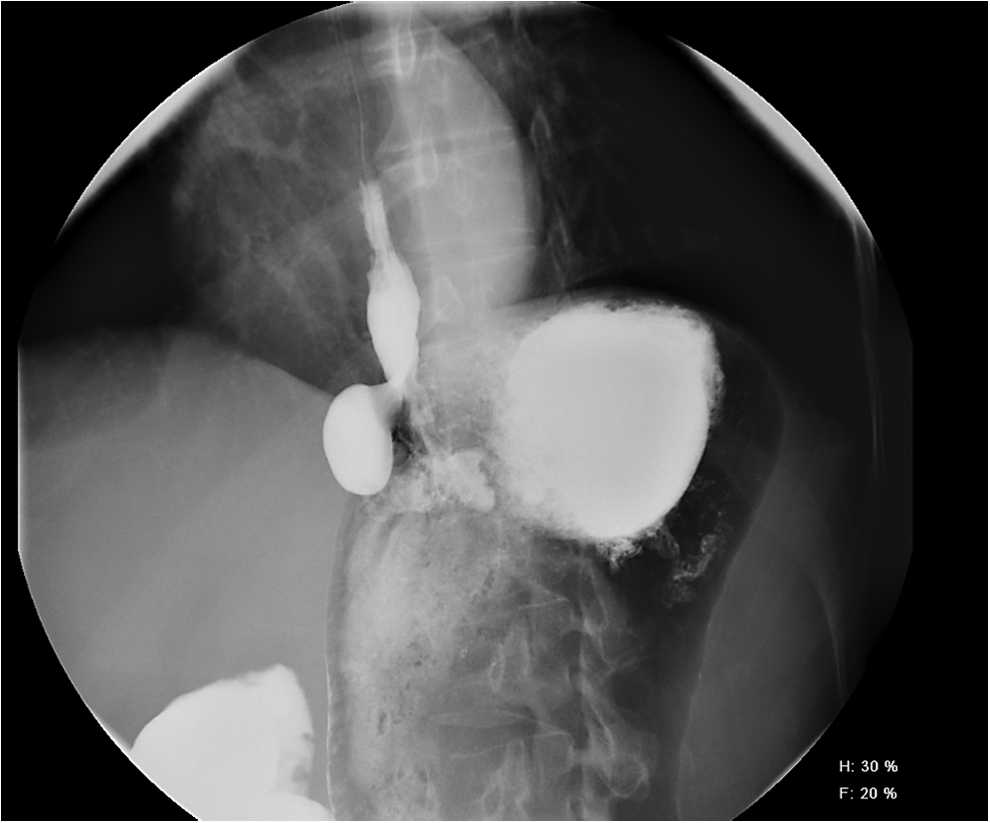
Four patients had severe anatomic distortion of the gastroesophageal junction relating to the prior TIF procedure. One patient underwent stapled resection of two traction esophageal diverticula (Fig. 1), each of which had a fastener at its apex. One patient with long esophageal stricture required myotomy of the thickened and stenotic esophageal wall (Fig. 2). Another patient with esophageal obstruction had pulsion diverticulum and underwent Heller myotomy with imbrication of the diverticulum. One patient with polyester mesh erosion of the esophagus required explant of the mesh along with repair of the esophagus and stomach along with Dor fundoplication—a fastener was found transiting from the stomach, through mesh, and into the esophagus (Fig. 3). The mesh was found to be colonized with actinomyces, requiring prolonged antibiotic therapy.
Swallow showing a traction diverticulum post-TIF. TIF, transoral incisionless fundoplication.

Swallow showing an esophageal stricture post-TIF leak. TIF, transoral incisionless fundoplication.
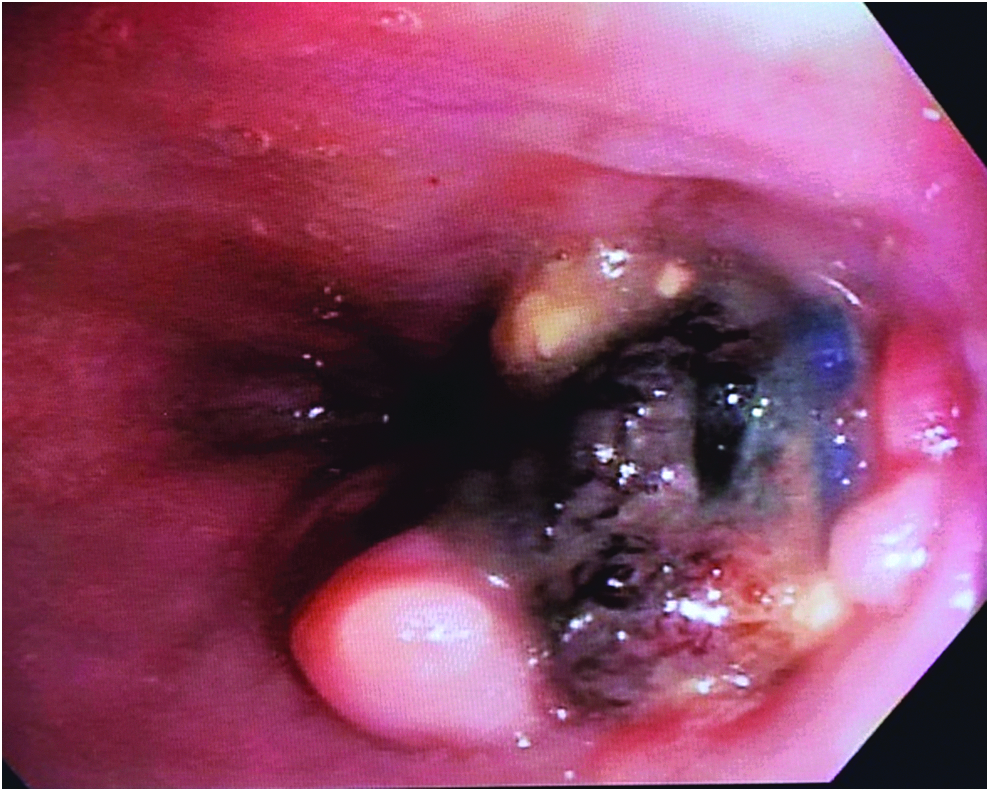
Endoscopy showing mesh erosion into the anterior esophagus and associated TIF fastener. TIF, transoral incisionless fundoplication.
At mean follow-up of 10.7 months (range 1–42 months), 7 patients had persistent complaints: dysphagia (n = 4), chest pain (n = 3), and cough and sinus type symptoms (n = 2). EGD was repeated in these 7 patients and was normal (n = 3), mild stenosis requiring dilation (n = 2), Los Angeles grade B esophagitis (n = 1), and Barrett's esophagus (n = 1). Ambulatory pH testing was performed in 1 patient with postoperative symptoms and was normal.
Discussion
TIF is a minimally invasive technique for the management of GERD by means of an endoscopically created fundoplication. Since its introduction about a decade ago, TIF has gained widespread popularity. The procedure endoluminally recreates a 270-degree fundoplication by anchoring the fundus to the distal esophagus using polypropylene T fasteners. As a full-thickness plication of the esophagogastric junction, it is expected that anatomical distortion may occasionally result from TIF. Many components of a surgical fundoplication such as esophageal and gastric mobilization and crural closure cannot be performed via this endoscopic technique. In patients who have moderate to large hiatal hernias, TIF is only applicable after simultaneous hiatal hernia repair. Five patients in our series had a laparoscopic hiatal hernia repair simultaneous with an endoscopic fundoplication. Two patients treated with simultaneous hiatal hernia repair and TIF sustained such resulting anatomical distortion of the foregut that esophagectomy was entertained at other centers before esophageal salvage at our center. In addition, dense adhesions were encountered in all patients who underwent these hybrid repairs. As such, we conclude that simultaneous hiatal hernia repair and TIF should be strongly discouraged.
Currently, four devices are approved by the FDA for endoluminal implantation-based antireflux therapy: EndoCinch (BARD Endoscopic Technologies, CR Bard, Billerica, MA), Endoscopic Plicator System (NDO Surgical, Inc., Mansfield, MA), MUSE™ (Medigus Ultrasonic Surgical Endostapler system Medigus Ltd., Omer, Israel), and EsophyX. TIF using the EsophyX device was approved by the FDA as a minimally invasive procedure for management of GERD in September 2007 following the seminal report by Cadière et al. 5 Their group reported 68% improvement in GERD-Health Related Quality of Life scores and a 67% improvement in the heartburn score at 12 months post-TIF; 56% of patients were reportedly “cured” and 24% of these “completely cured” (stopped all medication and free of heartburn and regurgitation) at 12 months. Three serious adverse effects were reported, which included two esophageal perforations at the time of performance of the TIF procedure that had to be repaired surgically. Post-TIF, bleeding was reported in 1 patient who required blood transfusions and endoscopic control. In subsequent short-term follow-up studies of 6–14 months, up to 80% of patients were reported to be off PPIs.7,8
The rates of surgical remediation in patients undergoing TIF range from 6% to 18%.11,13–17 Wilson et al. followed 100 patients for a year post-TIF. Esophageal acid exposure was normalized in half the patients. While relief from heartburn and regurgitation was reported to be 78% and 83%, respectively, 6 patients required revisions with 5 patients undergoing a laparoscopic fundoplication 13 Similarly, Muls et al. evaluated 66 patients in a prospective multicenter study and at 3 years of follow-up 18% patients had undergone revisional procedures (LNF in 2 and redo TIF in 10). 14
LNF as a revisional procedure post-TIF can be safely performed generally with good outcomes. Failure after a TIF was analyzed by Perry et al.; 7 patients underwent a laparoscopic fundoplication without reported postoperative complications. 15 All the patients were discharged the next day. While revision to LNF is feasible post-TIF, dysphagia can be problematic and may not respond as well as acid reflux. Witteman reported a series of 15 patients who failed TIF and underwent a revisional fundoplication for treatment failure; 33% of patients reported persistent dysphagia and 27% required endoscopic dilatations. 16 We noted a similar trend in our cohort with 36% patients reporting postrevision dysphagia. Two of these patients had undergone a concomitant laparoscopic hiatal hernia repair and TIF, while one had suffered a leak post-TIF and resultant mediastinitis. This patient developed a long distal esophageal stricture and required multiple dilatations postoperatively. While his esophagus appeared patent on EGD and barium swallow, he continued to have some chest pain and dysphagia.
Bell et al. followed 165 patients who underwent a TIF; 15% required laparoscopic antireflux surgery (LARS) for TIF failure. Of a total of 28 patients who underwent a laparoscopic revision after a TIF, 29% of patients reported post-TIF extraesophageal symptoms. Anatomical distortion after TIF was also found: 6 patients had a hiatal hernia and 5 were noted to have traction esophageal diverticula. 12 While 75% of these patients had evidence of a residual anterior fundoplication, a posterior fundoplication was not present in any patient. Postoperatively 2 patients required dilatation for dysphagia and 2 patients underwent another operation for a small paraesophageal hernia and refractory gas bloat, respectively. Furnee et al. reported similar findings; 11 patients underwent an LNF post-TIF for persistent symptoms. During the LNF, gastric perforation occurred in 2 patients. One patient continued to have daily heartburn and 3 had persistent dysphagia. 17 In our series, the vast majority of patients had anatomic failure with hiatal hernia, but significant anatomical distortion was found in 4 patients requiring a greater complexity of reoperation for remediation. As expected, these patients had a more protracted clinical course but eventually recovered well. No patient in our series required another surgical intervention although EGD was performed in 7 patients for recurrent or persistent symptoms.
Not much prospective data are available on TIF and LARS. A small case/control study with 20 patients in each arm compared TIF to a laparoscopic Nissen or Toupet fundoplication. 18 In a short-term follow-up, all arms showed similar reduction in frequency and severity of GERD; 83% after TIF, 80% after Nissen, and 92% after Toupet fundoplications reported symptoms less than once per month. Kaindlstorfer conducted a randomized control trial comparing the endoscopic fundoplication with the NDO Plicator device and LARS. There were 37 and 33 patients in the Plicator and LARS arm, respectively, with 18 patients undergoing a Toupet and 15 a Nissen fundoplication. Greater reduction in total reflux outcomes and reflux-specific esophageal acid scores was noted in the LARS group. At 3 months of follow-up, the mean DeMeester score decreased significantly from 25.8 to 1.1 in the LARS group but was not significantly reduced in the Plicator group (20.1 to 14.1). Gastrointestinal quality-of-life scores improved in both treatment groups. One patient in the Plicator group required transfusion and endoscopic intervention for bleeding. Based on persistent symptoms, 13 patients required reintervention, 11 underwent another endoscopic plication, and 2 underwent a Nissen. 19
TIF is a minimally invasive technique for managing GERD. A subset of patients who develop recurrent symptoms will require corrective surgery. Our small case series tries to highlight the potential challenges that are encountered during remedial surgery after TIF. We conclude from our experience that concomitant laparoscopic hiatal hernia repair with TIF appears to pose increased challenges for remediation, and thus, we cannot recommend this approach. Furthermore, we recommend that all patients with symptomatic failure of TIF undergo a comprehensive evaluation, looking for anatomic distortion of the GEJ. Remediation of patients with symptomatic TIF failure using LNF is effective for reflux symptoms, but may be less effective for post-TIF dysphagia.
Footnotes
Disclosure Statement
No competing financial interests exist.