
Abstract
Abstract
Aim:
Our aim was to perform a Bayesian network meta-analysis of short-term and long-term outcomes of open surgery (OS), laparoscopic surgery (LS), and robotic surgery (RS) after neoadjuvant chemoradiotherapy (nCRT) for rectal cancer.
Methods:
We searched randomized controlled trials (RCTs) and non-RCTs published up to October 2018 from PubMed, Embase, Cochrane Library, and Web of Science. We selected studies referencing the comparison between at least two of OS, LS, and RS. Short-term and long-term outcomes of different surgery procedures were evaluated. Mean differences or odds ratios and their 95% credible interval were pooled with Bayesian modeling.
Results:
In the network meta-analysis, 15 studies were identified through database searching and other sources that included three RCTs and nine non-RCTs enrolling 2360 patients. As for long-term outcomes, we did not find any significant difference among these surgery procedures after nCRT for rectal cancer in this network meta-analysis. As for short-term outcomes, no significant outcomes were obtained except for operative time, blood loss, length of incision, and time to pass first flatus. Our meta-analysis illustrated that RS had the longest operative time. However, LS had a significantly shorter operative time than RS, shorter incision than OS, shorter time to pass first flatus than OS, and less blood loss than OS.
Conclusions:
RS was regarded as the inferior surgery procedure after nCRT for rectal cancer. Meanwhile, LS might possibly be the most safe and feasible surgery procedure after nCRT for rectal cancer.
Introduction
Colorectal cancer is the third most common type of cancer and the fourth leading cause of cancer-related death in the world. 1 Colorectal cancer is a relative common cancer in China, especially for men in urban areas. Approximately one third of all colorectal cancers are localized in the rectum. 2 The management of rectal cancer has transformed gradually and continues to evolve. At present, radical surgery with total mesorectal excision after neoadjuvant chemoradiotherapy (nCRT) is the standard treatment for patients with locally advanced rectal cancer.3,4
Historically, radical surgery was the main treatment for rectal cancer and therapy is effective because of the improved surgical technique. 5 It is reported that laparoscopic surgery (LS) has progressively replaced open surgery (OS) in recent decades owing to favorable short-term outcomes, such as smaller wound size, less blood loss, faster recovery, and shorter postoperative hospital stays. 6
In addition, laparoscopic instruments have several limitations such as the anatomical confinement of the deep pelvis, amplification of the tremor from the fulcrum effect, unstable image provided by the hand-held camera, and inability to perform high precision suturing. Therefore, robotic surgery (RS) is gaining popularity. RS has the potential to overcome some of the limitations of LS, providing an immersive 3D field, articulating instruments, and a stable camera platform.7–9 Several small nonrandomized studies have supported RS safety and efficacy in rectal cancer surgery. However, the sample size of each study was small.
A Bayesian network meta-analysis can synthesize direct and indirect evidence to evaluate multiple factors. Therefore, we performed a Bayesian network meta-analysis of short- term and long-term outcomes of OS, LS, and RS after nCRT for rectal cancer.
Methods
Literature search
We searched randomized controlled trials (RCTs) and non-RCTs published up to October 2018 from PubMed, Embase, Cochrane library, and Web of Science. The key words included colorectal cancer, neoadjuvant therapy, OS, LS, and RS, which were combined with any derivatives of these terms. No language restrictions were used. In addition, manual searching of reference lists from existing review articles and identified additional studies was also performed.
Inclusion criteria
The inclusion criteria included the following: (1) the study was designed as RCTs or non-RCTs; (2) patients received and completed nCRT before surgery; (3) the study should reference the comparison between at least two of the three surgery procedures for rectal cancer; (4) the study should contain one of the short-term and long-term outcomes; (5) the short-term outcomes included operative time, blood loss, length of incision, lymph nodes harvested, number of patients with positive circumferential resection margin (CRM), time to pass first flatus, complications, local recurrence, and postoperative hospital stay; and (6) the long-term outcomes of study included 3- or 5-year overall survival rate and 3- or 5-year disease-free survival rate.
Extraction of data
Two reviewers extracted data independently, and a third reviewer resolved the discrepancies of the above reviewers. The extracted data included the following: author, year and country of publication, study design, arm, number in arm, surgical types, characteristics of the patients (age and gender), neoadjuvant therapy, interval between nCRT and surgery, American Joint Committee on Cancer stage, the short-term outcomes (operative time, blood loss, length of incision, lymph nodes harvested, number of patients with positive CRM, time to pass first flatus, complications, local recurrence, and postoperative hospital stay), and long-term outcomes (3- or 5-year overall survival rate and 3- or 5-year disease-free survival rate).
Assessment of methodological quality
All RCTs were assessed for the risk of bias with the Cochrane Collaboration's Risk of Bias Tool. 10 We evaluated the risk of bias of RCTs using the following items: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. Every parameter was classified into three categories (low risk, high risk, and unclear risk). All non-RCTs were evaluated with methodological index for nonrandomized studies (MINORS). 11 Twelve items were considered for inclusion in MINORS. The items were scored 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate). Then we summed all the item scores to obtain the global scores.
Statistical analysis
The network meta-analysis was performed using R software version 3.4.1 and Just Another Gibbs Sampler (JAGS) version 4.2.0. The rjags package version 4–6 was used to run JAGS, 12 and gemtc package version 0.8–2 was also used. Data on continuous variables reported as median and range were converted to mean and standard deviation according to the Hozo method. 13 We synthesized mean difference (MD) or odds ratio and their corresponding 95% credible interval (CrI) with Bayesian modeling. We computed the surface under the cumulative ranking curve (SUCRA) to get rank probabilities of each outcome. 14 SUCRA would be 1 when a treatment is certain to be the best and 0 when a treatment is certain to be the worst. 14
Results
Description of the studies included
A flow chart of the search strategy is given in Figure 1. Fifteen studies containing 12 trials were identified through database searching and other sources, which included three RCTs and nine non-RCTs enrolling 2360 patients. Table 1 shows the basic characteristics of the 15 articles included. Among the 15 articles, 8 studies only reported on short-term outcomes, 3 studies only reported on long-term outcomes, and 4 studies reported on both short-term and long-term outcomes. The risk of bias for RCT and MINORS score for non-RCT are given in Table 2.

Flowchart of literature search.
Description of Studies Included
AJCC, American Joint Committee on Cancer; APR, abdominoperineal resection; AR, anterior resection; CAA, coloanal anastomosis; ISR, intersphincteric resection; LAR, low anterior resection; LH, Low Hartmann; LS, laparoscopic surgery; nCRT, neoadjuvant chemoradiotherapy; NR, not report; OS, open surgery; RCT, randomized controlled trials; RS, robotic surgery; TP, total proctocolectomy.
Assessment of Methodological Quality of Studies Included
MINORS, methodological index for nonrandomized studies; RCT, randomized controlled trials.
Synthesis of results
Short-term outcomes
Twelve studies6–8,15–23 were enrolled in short-term outcomes of OS, LS, and RS after nCRT for rectal cancer. In this network meta-analysis, we analyzed nine short-term outcomes, including operative time, blood loss, length of incision, lymph nodes harvested, number of patients with positive CRM, time to pass first flatus, complications, and postoperative hospital stay (Fig. 2). According to our analysis, RS had a significantly longer operative time compared with OS or LS (MD = 95.0, 95% CrI: 42.0∼150.0; MD = 78.0, 95% CrI: 32.0∼120.0) (Table 3). OS was not different from LS in operative time (MD = −17.0, 95% CrI: −43.0∼9.4) (Table 3). As given in Table 3, OS had a significantly more blood loss than LS (MD = 67.0, 95% CrI: 21.0∼120.0). We also found that OS had a significantly longer incision than LS (MD = 9.4, 95% CrI: 0.068∼19.0) (Table 3). Furthermore, OS had a significantly longer time to pass first flatus than LS (MD = 0.7, 95% CrI: 0.064∼1.3) (Table 3). We did not get other significant results about the short-term outcomes of three surgery procedures after nCRT for rectal cancer.
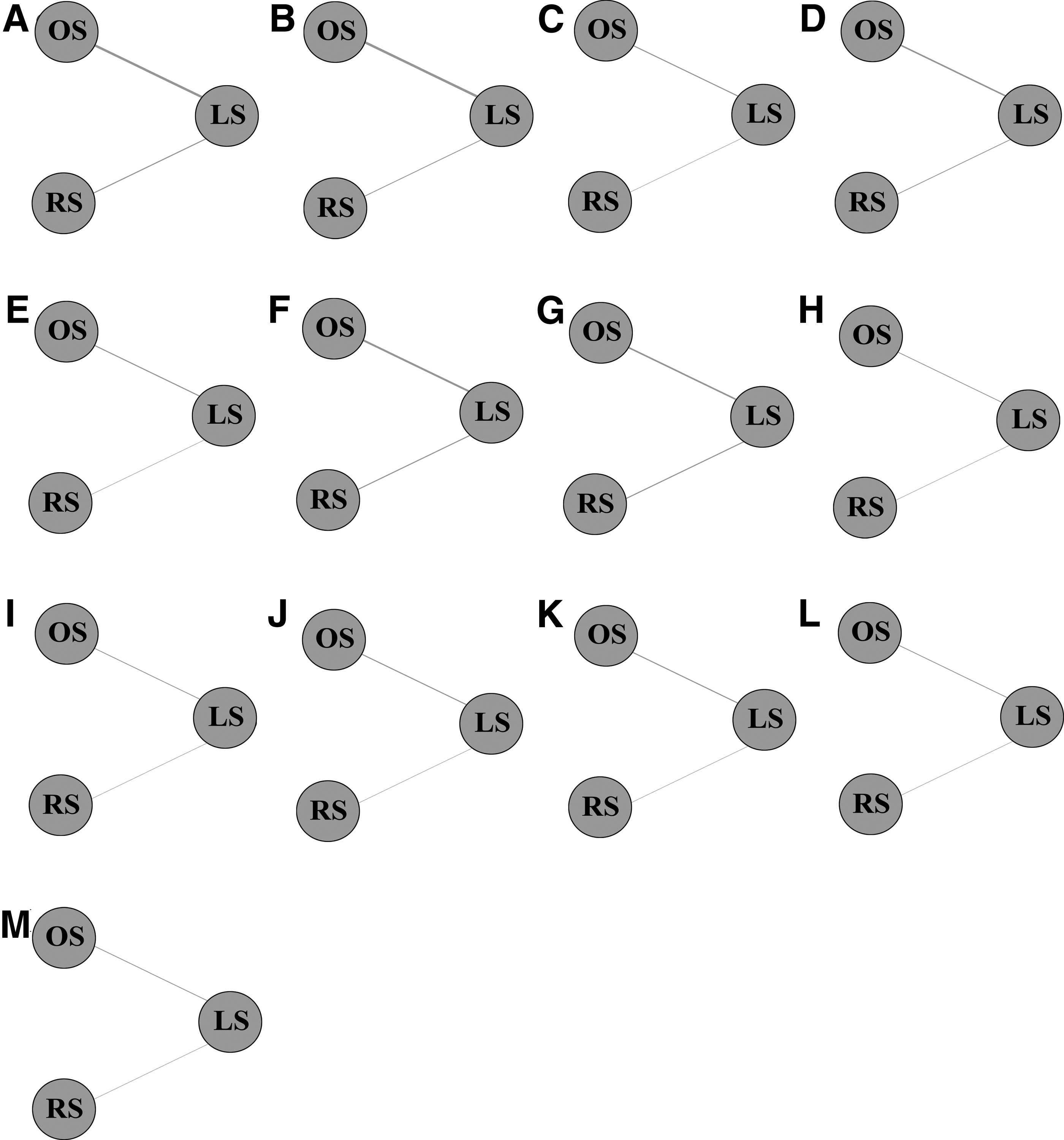
Network diagrams of eligible studies.
Synthesis of Results According to the Network Meta-Analysis (Odds Ratios or Mean Differences Corresponding 95% Credential Intervals)
P values in italics are significant.
CRM, circumferential resection margin; LS, laparoscopic surgery; OS, open surgery; RS, robotic surgery.
Long-term outcomes
Seven studies9,15,17,19,21,24,25 focused on the analysis regarding long-term outcomes that included local recurrence, 3-year overall survival rate, 3-year disease-free survival rate, 5-year overall survival rate, and 5-year disease-free survival rate. But no significant results were found about long-term outcomes.
Relative ranking of three surgery procedures
As given in Table 4, we calculated SUCRA of different surgery procedures to evaluate the rank probabilities. In this network meta-analysis, we found that OS ranked the highest in blood loss, length of incision, number of patients with positive CRM, time to pass first flatus, complications, local recurrence, and postoperative hospital stay and ranked the lowest in operative time, 3-year overall survival rate, 3-year disease-free survival rate, and 5-year disease-free survival rate. LS ranked the highest in 3-year overall survival rate, 3-year disease-free survival rate, 5-year overall survival rate, and 5-year disease-free survival rate and ranked the lowest in length of incision, number of patients with positive CRM, and lymph nodes harvested. RS ranked the highest in operative time, and lymph nodes harvested and ranked the lowest in blood loss, time to pass first flatus, complications, local recurrence, postoperative hospital stay, and 5-year overall survival rate.
Relative Ranking of Three Surgeries After Neoadjuvant Chemoradiotherapy for Rectal Cancer Evaluated by Using Surface Under the Cumulative Ranking Curve Values
CRM, circumferential resection margin; LS, laparoscopic surgery; OS, open surgery; RS, robotic surgery.
Discussion
In this Bayesian network meta-analysis, we systematically reviewed the short-term and long-term outcomes of OS, LS, and RS after nCRT for rectal cancer. As for long-term outcomes, we did not find any significant difference among these surgery procedures after nCRT for rectal cancer in this network meta-analysis. As for short-term outcomes, no significant outcomes were obtained except for operative time, blood loss, length of incision, and time to pass first flatus. Combined with SUCRA, our meta-analysis illustrated that RS might possibly be the most unsatisfying surgery procedure with the longest operative time. However, LS did perform well in our analysis. LS had a significantly shorter operative time than RS, shorter incision than OS, shorter time to pass first flatus than OS, and less blood loss than OS. That made it the most safe and feasible surgery procedure according to our network meta-analysis.
As we know, this network meta-analysis is the very first and largest review considering the short-term and long-term outcomes of different surgery procedures after nCRT for rectal cancer. In this analysis, OS was not different from LS in operative time, and OS had significantly more blood loss than LS, which was consistent with Chen's meta-analysis. 26 As Prete et al. 27 described in their meta-analysis, RS had longer operating time and similar lymph nodes harvested compared with LS. These results were confirmed in our meta-analysis. However, some results of our network meta-analysis were inconsistent with Chen's meta-analysis. For example, Chen et al. 26 found that LS had statistically less lymph nodes harvested than OS, whereas our meta-analysis indicated that there was no obvious difference between OS and LS. The reason for inconsistence between our meta-analysis and that of Chen may be that we ruled out studies of incomplete nCRT.
This network meta-analysis has several limitations. We cannot analyze the consistency from the direct and indirect evidence because there were no direct evidence between OS and RS, no indirect evidence between OS and LS, and no indirect evidence between LS and RS. In addition, different experience among the surgeons might affect outcomes during the surgical procedure. Third, hospital length of stay is a difficult metric because different countries have very different approaches to this. Fourth, the large number of non-RCTs may compromise the statistical power. Another limitation is that open surgeries may be selected for larger cancers that technically cannot be approached with minimally invasive operations. Finally, we included the Z0651 trial where 34 of 240 LS patients received robot approach,24,25 which may contribute to biases.
In conclusion, based on evidence from RCTs and non-RCTs, this network meta-analysis indicates that RS was regarded as the inferior surgery procedure after nCRT for rectal cancer with the longest operative time. Meanwhile, LS might possibly be the most safe and feasible surgery procedure after nCRT for rectal cancer because it had a significantly shorter operative time than RS, shorter incision than OS, shorter time to pass first flatus than OS, and less blood loss than OS. These results may help the surgeon in the selection of surgeries after nCRT for rectal cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.