
Abstract
Abstract
Background:
Rectal cancer is now an increasing problem in both developed and developing countries. In the last 7 years, minimally invasive surgery for this disease has entered a new era of transanal resection with/without laparoscopic assistance.
Materials and Methods:
We present here a prospective study done in Egypt (probably the earliest experience) and Spain on the feasibility of hybrid NOTES in rectal cancer.
Results:
From September 2015 till November 2017, 18 cases underwent transanal total mesorectal excision with no detected mortality and with morbidities in 44% of cases, from which 5 were class III on Clavien–Dindo scale requiring intervention. Good quality total mesorectal excision was obtained in more than three quarters of our patients.
Conclusions:
In our experience, the technique was technically demanding with a long learning curve; however, the short term results were very good in alliance with other few similar reports.
Introduction
Colorectal cancer is the third commonest cancer worldwide, where in Spain it ranks the second just behind breast cancer in females and prostate cancer in males. 1 However, it is the seventh commonest cancer among both males and females in Egypt according to the first national cancer registry program in 2014. 2
Rectal cancer resection had been long renowned by the inherent high local recurrence rate until Heald 3 introduced the concept of the holy total mesorectal excision (TME) plane. In his article, he claimed that circumferential inadequate safety margin was the main cause of local recurrence. Since then, TME has been the standard of care in rectal cancer surgery.
Not far late, the German surgeon Gerhard Buess invented his rigid platform called transanal endoscopic microsurgery (TEM), which represented a solution for the problem of early rectal cancers that were difficult to access both abdominally and through the anus with Sim's retractors. 4
With the increased tolerance of laparoscopic colorectal surgery starting from the first case report in 1991, 5 the difficulty of reaching the deep pelvis for resection of mid-low rectal cancers together with the inflexibility of the current linear staplers (difficult angulations) to cut the distal margin perpendicularly arose to the surface. In the same year, a technique called transabdominal transanal (TATA) appeared for distal tumors where the anal part was done through open (i.e., nonendoscopic) approach. 6
Bearing in mind the necessity of following the TME plane, the added benefits of laparoscopy, the appeared limitations in current laparoscopic tools, the added experience from the TATA approach, and the presence of the transanal TEM port, a combined laparoendoscopic approach to those tumors was thought of. 7 Swine trials were initiated, but it was not until 2008 when Patricia Sylla published her first case of hybrid NOTES surgery using laparoscopy and TEM for rectosigmoid resection 8 and then in 2010 reported the first NOTES TME in humans, 9 what is later named TaTME.
Currently, there is small number of studies addressing the feasibility and short term outcomes of TaTME in rectal cancer; unfortunately, most of these studies are retrospective with no conclusive results. Herein, we present a two center prospective study to address this technique.
Materials and Methods
Patients
From September 2015 to November 2017, 18 patients (4 in Egypt and 14 in Spain) with rectal cancer were enrolled in a prospective pilot study to assess the short term outcomes of the down to up route of TME. The inclusion criteria endorsed medically fit patients of any age with pathologically proven rectal cancer without distant spread as confirmed by computed tomography scan of chest, abdomen, and pelvis. Patients were excluded if (1) American Society of Anesthesiologist score 4 and 5, (2) cardiac or chest problems that cannot withstand carbon dioxide (CO2) insufflation, (3) unresectable tumors (defined as those who cannot be resected without a high likelihood of leaving microscopic or gross residual disease at the local site because of tumor adherence or fixation), (4) obstructed or perforated cancer, and (5) incontinent patients.
Magnetic resonance imaging (MRI) pelvis was done routinely for all cases; those with locally advanced tumors or node positive were referred to neoadjuvant therapy before surgery. Patients were operated by senior colorectal surgeons; one of the authors (I.H.M.) attended all the operations. All patients were consented, and the study obtained ethics committee approval.
Operative technique
The procedure was done transanal first (3 cases in Egypt), laparoscopic first (1 case in Egypt), or concomitant Cecile approach (14 cases in Spain).
Transanal phase
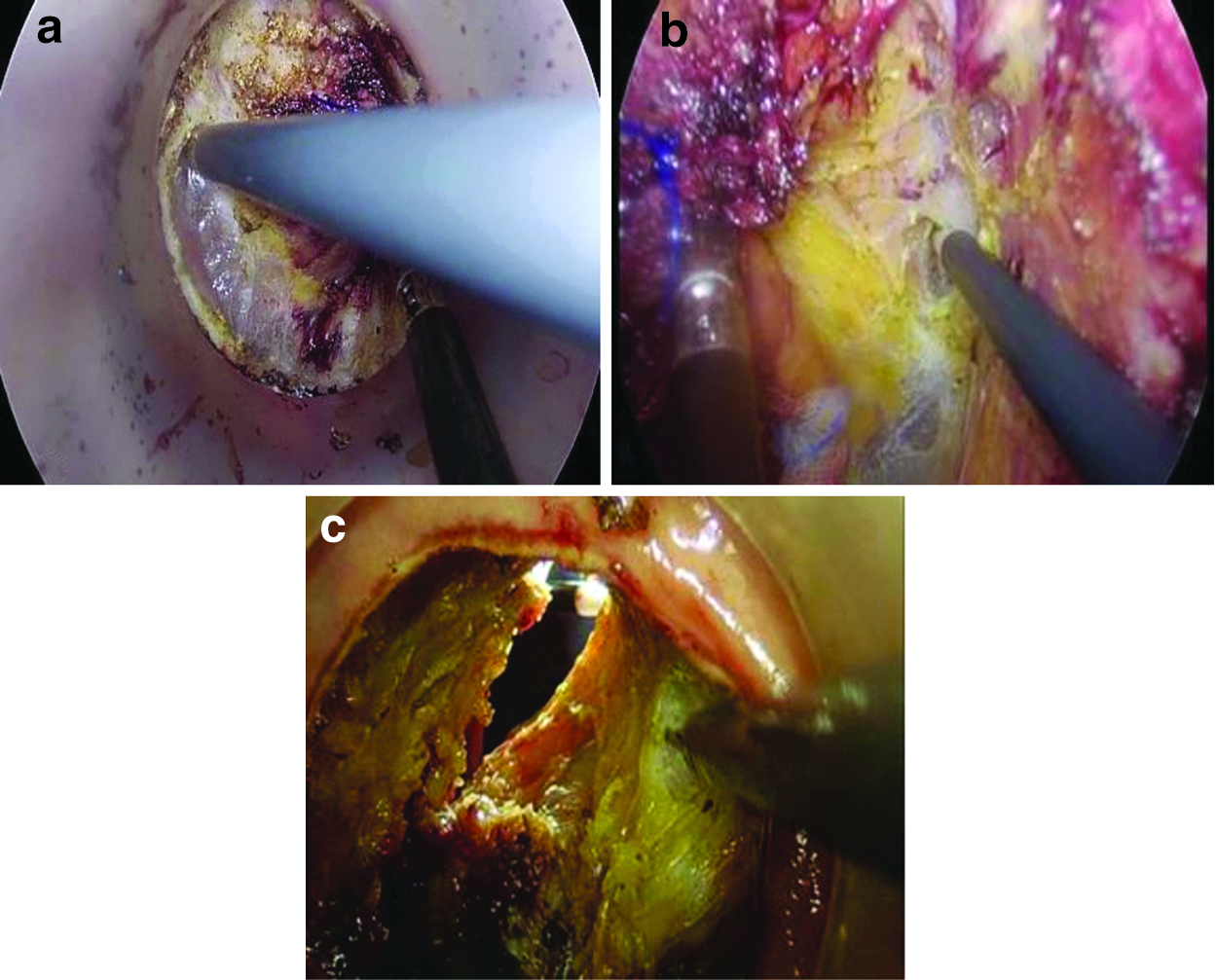
Transanal Endoscopic Operation (TEO) Proctoscope (Karl Storz, Tuttlingen, Germany) or GelPOINT path Transanal Access (Applied Medical, Rancho Santa Margarita, CA) was inserted into the rectum (Fig. 1), and CO2 pneumorectum was established. The lumen is occluded using a circumferential purse-string suture below the level of the tumor (Fig. 2a). About 1 cm distal to the occluding purse string, a circumferential incision is done using monopolar cautery (Fig. 2b). The avascular presacral plane was entered, followed by combined sharp and blunt dissection cephalad in all directions in the TME plane. Next, the abdominal cavity was carefully entered at the peritoneal reflection (Fig. 3).
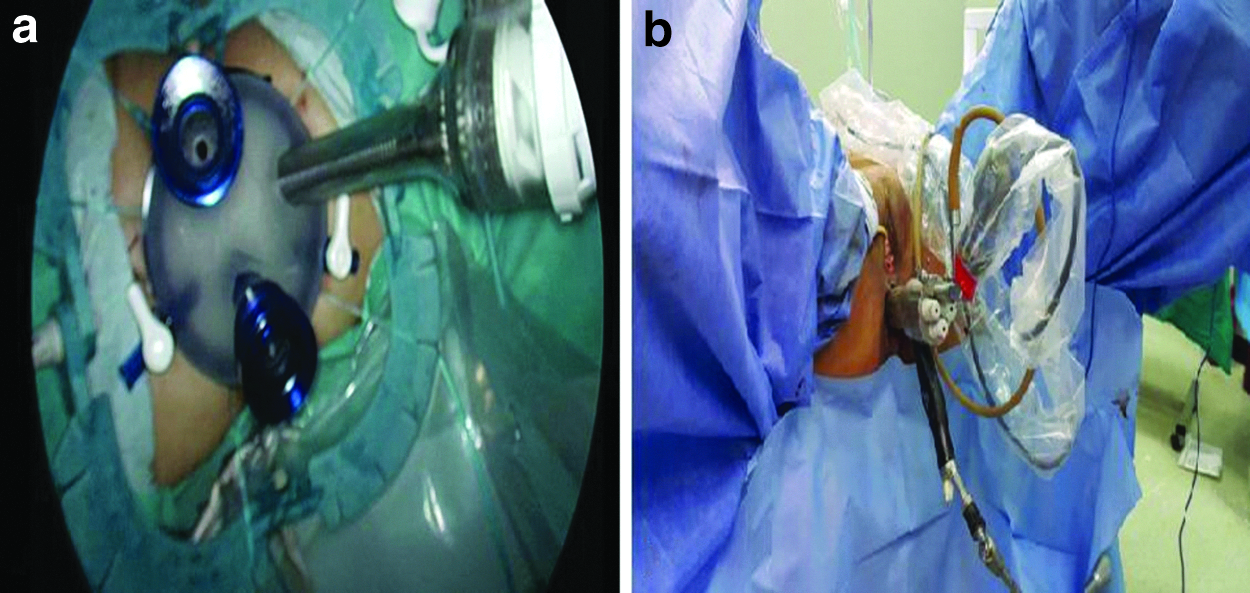
Shows the transanal platforms inserted
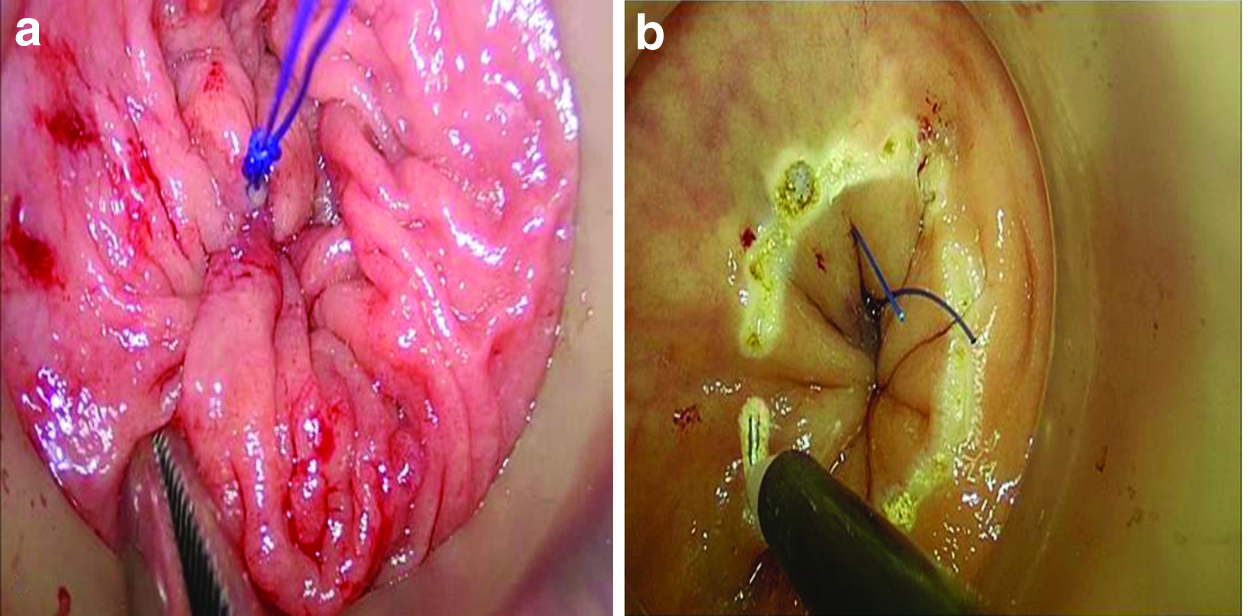
Shows
Dissection using hook in the total mesorectal excision plane.
Transabdominal phase
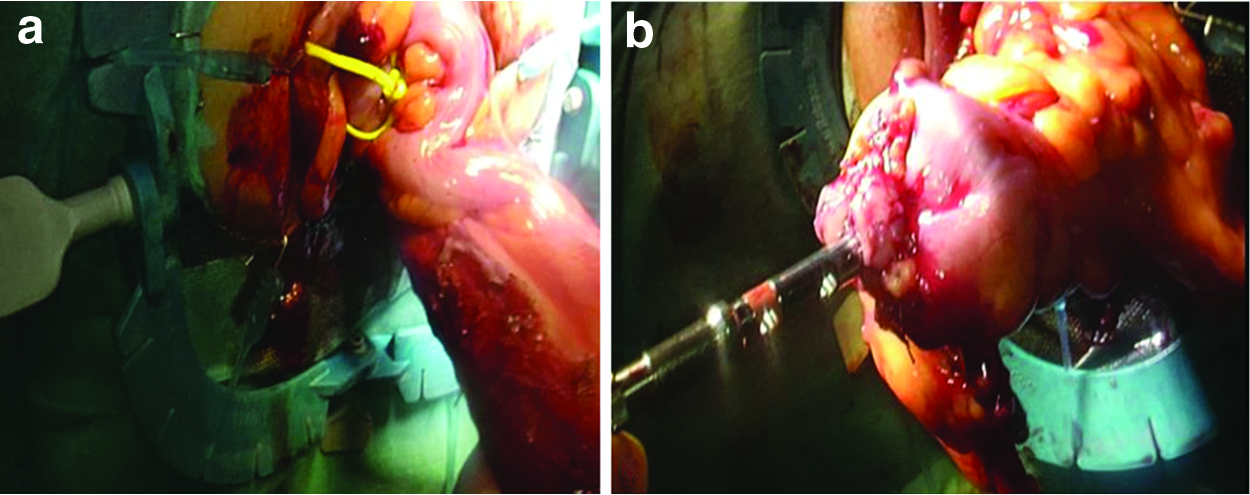
It was started by clamping or ligating the sigmoid colon to allow for rectal insufflation (Fig. 4a). Then, inferior mesenteric artery and vein ligation (Fig. 4b), colon dissection, and mesocolic excision were performed laparoscopically, followed by dissection in TME plane to meet the transanal team (Fig. 4c–e). Mobilization of the splenic flexure was done if needed.

Specimen retrieval
The specimen was either delivered transanally and proximal margin divided extracorporeally (Fig. 5a) or through Pfannenstiel incision. For anastomosis, direct hand-sewn anastomosis was implemented after intersphincteric resection, otherwise a stapled anastomosis was performed. In the latter, the anvil of the stapler was introduced into the proximal colon using a standard purse-string suture (Fig. 5b) with a rubber tube connected for later manipulation and connection to the stapler handle. Appropriate orientation of the colon was visualized, and the previously placed proximal anvil was delivered into the rectal stump using the rubber tube as a handle. A purse-string suture was placed at the end of the open rectum. The stapler was mated with the anvil shaft under direct vision of a laparoscope. The stapler was then fired and removed. Pneumorectum is reestablished, and the anastomosis is endolumenally inspected. All patients are followed at least for 1 month postoperative.
Primary outcome was the quality of mesorectal excision, while secondary outcomes were operative time, blood loss, and morbidities.
Statistical analyses
The data of these patients were analyzed, and statistical values were obtained using SPSS version 22 (SPSS Inc, Chicago, IL). Continuous variables are presented as mean when symmetrical or median and range when asymmetrical. Categorical variables are presented as proportions. Bivariate analysis was done using Pearson correlation, Student's t-test, Mann–Whitney test, and Chi-square test. P value <.05 was considered significant.
Results
The demographic data of the patients in the study are displayed (Table 1). Specimen extraction was done through the abdomen in most of the patients due to bulky rectum and/or surgeon preference, while through the anal canal in 5 cases (in one of them the colorectal anastomosis was found ischemic intraoperatively so a redo-anastomosis was done through Pfannenstiel). Conversion to conventional laparoscopy was needed in 2 cases (due to slow transanal progression in 1 and due to retrorectal nodal mass inaccessible transanally in the other), while conversion to open occurred in 3 cases (large tumor with difficult identification of the ureter in 1 case, early opening of pelvic peritoneum through excess dissection in the anterior plane transanally in the second, and inability to progress transanally with impossible distal cutting laparoscopically in the third case). No major intraoperative complication was encountered. Fourteen cases underwent primary anastomosis, all end to end. All cases did stoma as loop ileostomy, Hartmann's colostomy, or virtual ileostomy (Table 2). Only 4 patients needed intraoperative packed red blood cells (RBCs) transfusion (one to two packs). Pathologic details, completeness of mesorectal excision, and response to therapy are displayed (Table 3). Ten postoperative complications were detected in 9 patients and were classified by modified Clavien-Dindo classification of surgical complications as 5 grade III, 3 grade II, and 2 grade I (Table 4). Median hospital stay was 9.5 days (ranging from 4 to 34). Patients started oral between the first and the 7th day postoperative (median 2nd day). Minor leak occurred in 2 cases and was treated conservatively.
Shows a Descriptive Analysis of the Demographic Data of Our Patients
BMI, body mass index; DM, diabetes mellitus; HCV, hepatitis C virus; RFA, radiofrequency ablation; SD, standard deviation.
Shows a Description of the Operative Data
SD, standard deviation; TEO, Transanal Endoscopic Operation.
Shows a Descriptive Analysis of the Pathologic Data of Our Patients
AJCC, American Joint Committee on Cancer; CAP, College of American Pathologists; CRM, circumferential margin; SD, standard deviation; TME, total mesorectal excision.
Shows a Description of the Complications and Their Management in Our Study Group
As for comparing early 9 cases to the later group, it was found that the mean operative time dropped from 338 to 291 minutes, while the median blood loss dropped from 500 to 375 mL. In addition, no open conversion was needed in the later group with 1 case having completed dissection laparoscopically.
Primary outcome was quality of TME, for which neither age, sex, stage, size of the tumor nor distance from anal verge was a significant predictor factor. In addition, preoperative radiotherapy (RT) and response did not affect the quality. However, high body mass index (BMI) (>30) and the blood loss (>500 mL) significantly predict lower quality (P = .017 and .024, respectively).
Secondary outcomes were operative time, blood loss, and 30-day morbidity. The operative time was correlated significantly with the patient age with mean 152.5-minute longer time in patients younger than 40 years old (P = .018) and in those with blood loss >500 mL, who showed 109.5-minute longer operative time (P = .012).
Median blood loss was 500 (range 1300) mL. Only 4 patients needed intraoperative packed RBC transfusion (one to two packs). Blood loss was significantly correlated to operative time (P = .042) and stage groups (P = .027).
Finally the morbidity could not be predicted by any factor.
Discussion
The COLOR II trial proved noninferiority of the laparoscopic rectal surgery to open one in long-term outcomes. 10 However, in other trials, the results of laparoscopic surgery failed to prove noninferior to open resection, as in ALaCaRT and ACOSOG Z6051.11,12 To delineate this conflict, the COLOR III trial is currently in progress to assess the superiority of the TaTME technique over conventional laparoscopic rectal resection. 13
In general, TaTME is recommended mainly for obese, male (android pelvis), and postirradiated patients; together these factors suggest a difficult dissection both for open and laparoscopic approaches. Failure of abdominal progress during dissection of rectal tumors in any patient can be considered also as an indication for down to up surgery. 14 In concordance most of our patients were obese old males with low/mid tumors post long course chemoradiotherapy, except 1 patient who received chemotherapy followed by short course RT.
In Barcelona the largest known series of TaTME was published by Antonio Lacy, who afterwards assigned the 2 teams a technique called “Cecile approach” to reduce the time and effort in their surgery. 15 Fourteen patients in our study followed the same principle of 2 teams, while the other 4 patients were operated by 1 team.
However, the comparison of 1 to 2 teams in TaTME resection was addressed by some authors, without clear evidence of superiority. 16 Also in our study, no statistically significant difference was found, although time was shorter for the 2 teams group.
Good quality mesorectal excision as identified by complete and near complete TME specimen on pathologic examination was achieved in about 78% of our cases. These results are promising, although slightly lower than early results from other centers in United States (85%) and Denmark (100%).17,18 However, in the mentioned Danish study patients are almost all RT naive with BMI ≤30 explaining their excellent outcome.
In our study, the mean operative time was about 314 minutes and was correlated directly with the younger age and the amount of blood loss >500 mL. A figure that is slightly longer than reported by some authors. Also the median blood loss was 500 mL, which is greater than that encountered in similar studies; however, only 4 patients required intraoperative blood transfusion.7,17,19 This can be explained by the learning curve especially in cases operated in Egypt, where the technique is still in its infancy, and was improved in our later cases.
In our series, postoperative 30-day morbidity (excluding superficial wound infection) occurred in 44% of cases with no reported mortalities, a figure which is slightly higher than previous laparoscopic rectal surgery studies (32.6%). 20 One patient was complicated later by anastomotic stricture, for which redo combined anal and laparoscopic resection anastomosis was reported. 21
In the largest TaTME registry available, some factors were found affecting the efficiency of mesorectal excision and freelance of margins; those included positive circumferential margin (CRM) identified on pelvic MRI, low tumors at a distance <2 cm from the anorectal ring, and a transabdominal posterior dissection down to <4 cm from the anal verge. 7 However, in our study the BMI and intraoperative blood loss were the only significant predictors of the quality of CRM; the latter can be explained by the fact that more blood loss was encountered when we lose the avascular holy plane.
From our experience, we would like to raise some technical tips; first in our early Cecile cases a sixth port was used in the suprapubic region to clamp the sigmoid before developing pneumorectum which was latter omitted by suturing a rubber tape around the sigmoid early in the operation, second using monopolar diathermy should be the standard during transanal resection as the advanced bipolar tools seal rather than open the plane, and third after dissecting for a distance in the TME plane traction from the purse-string end becomes difficult so we insert a small gauze and use it to push rather than tract the closed end away from the plane.
We declare that yet small number of patients, working with two different platforms, and operation by different surgeons represent somehow limitations of our study.
Conclusion
TaTME is a feasible technique with comparable morbidity to conventional laparoscopy, low open conversion rate, and excellent short-term oncologic outcomes. In TaTME, high BMI and increased blood loss significantly predict lower quality of mesorectal excision. In addition, a long learning curve is needed to overcome the technical difficulties, shorten operative time, and decrease blood loss.
Footnotes
Disclosure Statement
The authors I.H.M., P.C.C., J.A.R., S.Z.K., M.A.F.H., and W.E. declare that they have nothing to disclose in this work. J.F.N. reports personal fees from Medtronic, and also from Johnson and Johnson, outside the submitted work.