
Abstract
Abstract
Objective:
To conduct a systematic review of the published studies concerning laparoscopic pediatric hydrocele (PH) repair and summarize the surgical details and operative outcomes of this procedure.
Materials and Methods:
A PubMed search was performed for all studies concerning laparoscopic repair of hydrocele in children. The search strategy was as follows: (laparoscop* OR coelioscop* OR peritoneoscop* OR laparoendoscop* OR minilaparoscop*) AND hydrocele* AND (child* OR pediatric*). Inclusion criteria included (1) children with hydrocele as the study participant; (2) laparoscopic PH repair as the main surgical procedure; and (3) operation time and complications as the outcomes of interest. Reviews, studies with insufficient information or reporting the outcomes of abdominoscrotal hydrocele, and duplicate patient series were excluded.
Results:
Overall, 20 studies fulfilled the inclusion criteria of this review and 15 studies were included in the final analysis. These studies comprised at least 2920 patients undergoing laparoscopic repair for various PH subtypes, of which most were conducted in Asia. Most authors repaired PH laparoscopically through an extraperitoneal approach, while only a few studies applied a laparoscopic intraperitoneal method. The majority of the studies used nonabsorbable sutures to ligate hydrocele sac, while very few studies used absorbable materials. Hydrocele sac was resected or transected in only five studies, but left alone in the majority. Mean operation time was between 15.6 and 43.2 minutes for unilateral laparoscopic PH repair and between 16.9 and 53.2 minutes for bilateral surgery. Operative complications were not very common, with a highest recurrence/persistence incidence of 1.4%. Subgroup analysis showed that hydrocele subtype, surgical approach, suture material, and management of hydrocele sac did not significantly influence the operative complications.
Conclusions:
laparoscopic PH repair seems to be a safe and effective procedure. Given the limitations of this review, our conclusion needs to be confirmed by more well-designed studies.
Introduction
Pediatric hydrocele (PH) is a common disease among children.1–3 It is a collection of fluid in the inguinoscrotal/labial canal, which presents a reducible or nonreducible painless swelling.2,4 It is generally considered that PH is associated with the patent processus vaginalis (PPV).2,3,5 Some PHs can spontaneously resolve by the first few months of life, while surgical intervention is recommended for those unresolved after a certain age (e.g., 1–2 years old).1–3,6
Traditionally, PH was repaired through an open approach, involving an inguinal incision, exposure of the inguinal canal and complete ligation of the PPV.1–3 However, the open approach may carry a higher risk of complications, such as vas and vessel damage and wound infection.2,3 Nowadays, open repair is being challenged by the laparoscopic approach, which has the advantages of minimal invasiveness, improved cosmetic results, and simultaneous management of the contralateral PPVs.1–3
PH and inguinal hernia were believed to have the similar cause and therefore share the same principle of surgical correction.2,3 Although laparoscopic herniorrhaphy has been increasingly used to manage pediatric inguinal hernia, there were few reports regarding the effectiveness of laparoscopy for the treatment of PH.1–3 In this study, we conducted a systematic review of all the published studies, and summarized the surgical details and operative outcomes of laparoscopic PH repair.
Materials and Methods
Search strategy
A systematic literature search of the MEDLINE/PubMed (National Library of Medicine and NIH) database was conducted to identify all studies concerning laparoscopic repair of hydrocele in children, which were published up to December 18, 2017, without the lower date limit. The search strategy was as follows: (laparoscop* OR coelioscop* OR peritoneoscop* OR laparoendoscop* OR minilaparoscop*) AND hydrocele* AND (child* OR pediatric*). Furthermore, reference lists of all relevant reviews were also examined manually to identify any additional relevant studies.
Study selection
The selection of studies was restricted to those published in English. All titles and/or abstracts were reviewed to initially exclude the studies, which were significantly irrelevant to laparoscopic PH repair. After that, the full text of potentially relevant studies or those with relevance was unclear according to the titles, and/or abstracts only were retrieved and carefully assessed for inclusion. The inclusion criteria were as follows: (1) children with hydrocele as the study participant; (2) laparoscopic PH repair as the main surgical procedure; and (3) operation time and complications as the outcomes of interest. Reviews and studies with insufficient information were excluded from this review. Studies reporting the outcomes of abdominoscrotal hydrocele were also excluded due to a different etiology. If the same cohort with identical endpoints was published in more than one study, only the most comprehensive information was included. The PH in this review included both “communicating” and “non-communicating” hydrocele according to the medical history and physical examination. The prediagnosed “non-communicating” hydroceles were not excluded initially because they were probably found with an ipsilateral PPV during the operation.
Surgical method
Laparoscopic PH repair had the same principle of surgical correction with open surgery, that is, high ligation of PPV. After general anesthesia, the patient was placed in the supine or Trendelenburg position. Then, a CO2 pneumoperitoneum was established at 8–10 mmHg. According to the surgical approach and surgeon's experience, one to three working ports/trocars were set on the abdominal wall, through which the laparoscopic lens and working instruments were introduced. If a PPV was present under laparoscopic exploration, the periorificial peritoneum at the level of the internal ring was ligated or sutured by a purse-string suture. If there was no PPV, the procedure would be converted to an open transinguinal or transscrotal hydrocelectomy, which was mainly used for hydrocele of the spermatic cord or scrotal hydrocele, respectively. The purse-string suture could be placed percutaneously by a puncture needle or via peritoneal cavity by a laparoscopic needle holder. The distal sac of PPV could be either resected intracorporeally or via a scrotal incision or left alone without resection. The fluid in the sac was squeezed into peritoneal cavity if possible or aspired by a needle syringe through the scrotum.
Postoperatively, the patients were followed with physical examination and/or scrotal sonography if necessary to detect any complications. The potential complications included hydrocele recurrence/persistence, testicular atrophy, contralateral occurrence, scrotal edema, hematoma, wound infection, suture site abscess, subcutaneous emphysema, and umbilical hernia. The strategy and length of follow-up usually varied according to the surgeon's preference among the included studies.
Data extraction
Data were extracted from each study using a predefined extraction form. The extracted data included general characteristics of the studies and patients (i.e., author's name, publication year, location, design and duration of study, number, age, and gender of patient, and type and laterality of disease), the surgical details (i.e., number and site of incisions, surgical approach, suture material, and management of the fluid and sac of hydrocele) and surgical outcomes (i.e., operation time, recurrence, other intra- and postoperative complications, and length of follow-up). Level of evidence was assessed according to the Oxford Center for Evidence-Based Medicine. 7
Statistical analyses
The outcome measures were operation time and complication rate. We assumed that the surgical outcomes were probably influenced by the type of hydrocele, surgical approach, suture material, and management of hydrocele sac. Given this, subgroup analyses of the outcome measures were performed across these potential influencing factors. The significance of differences between the subgroups was evaluated by t-test for continuous data and by chi-squared or Fisher's exact test for dichotomous data, respectively. All analyses were conducted using Stata 13.0 software (StataCorp, College Station, TX), and a two-sided P < .05 was considered statistically significant.
Results
Selection of the studies and the level of evidence
Figure 1 shows the study selection process of this review. From the 204 records initially identified, 35 studies1–3,8–39 fulfilled the predefined inclusion criteria. Subsequently, five reviews,1–3,8,9 one study with insufficient information, 10 three studies with duplicate data,11–13 and six studies reporting the outcomes of abdominoscrotal hydrocele14–19 were excluded. Finally, the remaining 20 studies were included in this review, comprising 12 case series23,25–30,32,34,36,38,39 (level 4) and 8 retrospective comparative studies20–22,24,31,33,35,37 (level 3).
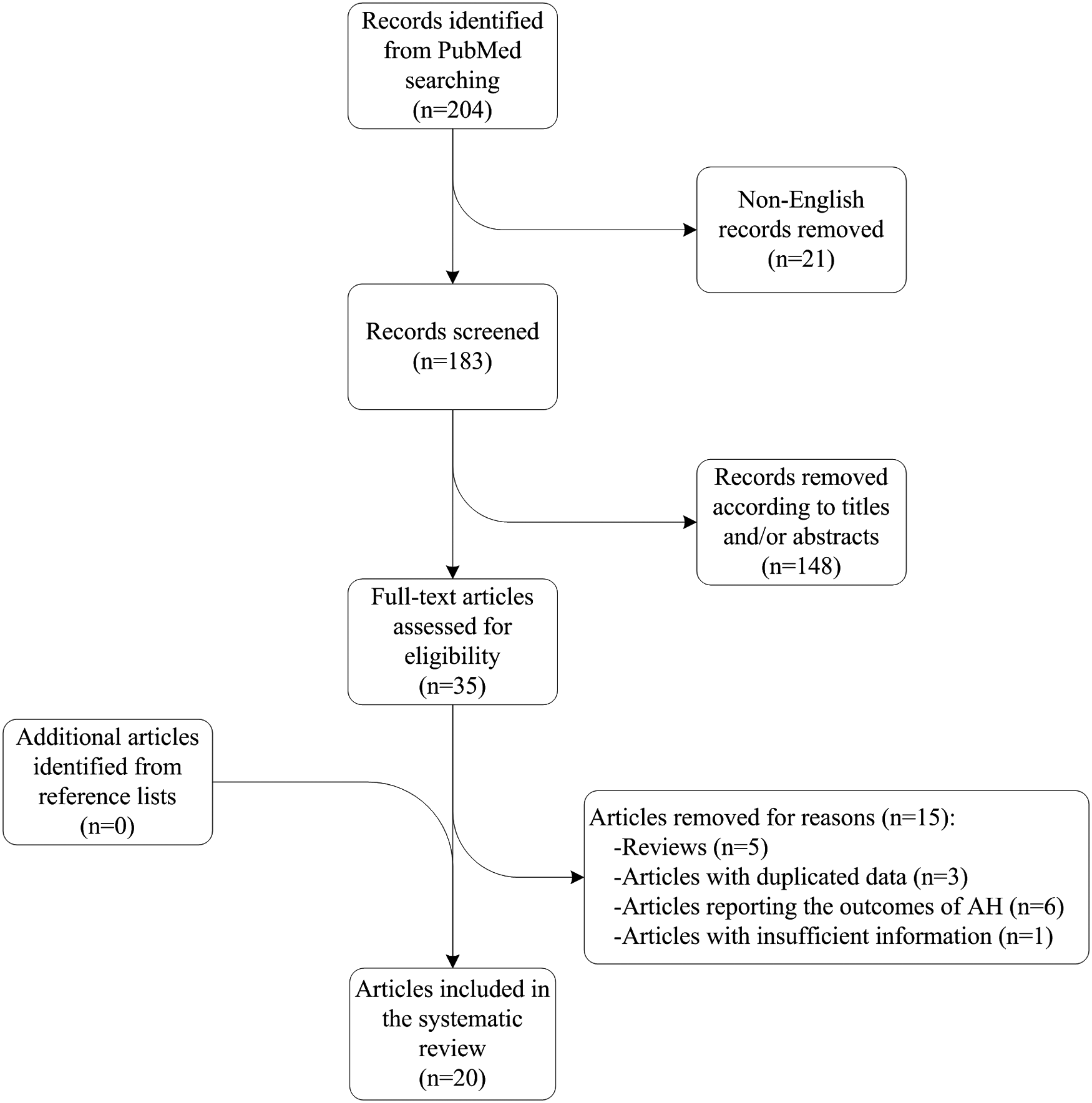
Flowchart of the search process.
General characteristics of the studies and patients
Publication dates of the included studies ranged from 1999 to 2017 (Table 1). Nine studies26,27,29,30,32–34,37,39 were conducted in China, four studies20,22,28,31 in Japan, two studies in Korea35,38 and United States21,36 each, and one study in Portugal, 24 Turkey, 23 and Austria 25 each. These studies comprised at least 2920 patients who underwent laparoscopic PH repair. Patients' age ranged from 1 month to 18 years. One study 38 only included patients with hydrocele of the canal of Nuck and two studies27,35 only with hydrocele of the spermatic cord. Five studies21,23,24,27,36 only included patients with communicating hydrocele, while the others with both communicating and noncommunicating hydrocele.
General Characteristics of the Included Studies and Patients
N/A, not available.
Surgical details of laparoscopic PH repair
Most authors repaired PH laparoscopically via a percutaneous extraperitoneal approach with transperitoneal visualization (i.e., extraperitoneal approach), while only a few studies25,26,35,38,39 performed laparoscopic repair through peritoneal cavity (i.e., intraperitoneal approach) (Table 2). One port incision at umbilicus and one or two stab incisions at the lower abdomen were mandatory for the extraperitoneal approach. Another incision for the grasping forceps was not necessary, but could greatly facilitate the operation. The laparoscopic intraperitoneal approach usually used three port incisions on the abdominal wall although it also could be performed via one or two umbilical incisions. 39 The majority of studies used nonabsorbable sutures to ligate the hydrocele sac, while very few studies21,25,26 used absorbable materials. The hydrocele fluid was squeezed into the peritoneal cavity or aspired by the syringe in almost all cases. However, the hydrocele sac was resected or transected in only five studies25–27,35,38 but left alone in the majority.
Surgical Details of Laparoscopic Pediatric Hydrocele repair
If the hydrocele cannot be manually emptied into the peritoneal cavity, the fluid is percutaneously aspirated by a syringe needle.
One stab skin incision was made at the level of internal ring for unilateral repair and two incisions for bilateral operation.
N/A, not available.
Operative outcomes of laparoscopic PH repair
Among the 20 studies included in this review, five studies20–24 were excluded from the statistical analysis because of reporting the combined results of PH and inguinal hernia rather than the isolated outcomes of PH. The operation time of laparoscopic PH repair was reported in 10 studies and varied greatly from 8 to 105 minutes. The mean operation time was between 15.6 and 43.2 minutes for unilateral repair and between 16.9 and 53.2 minutes for bilateral surgery (Table 3).
Surgical Outcomes of Laparoscopic Pediatric Hydrocele Repair
N/A, not available; TLH, totally laparoscopic hydrocelectomy; SIH, scrotal incision hydrocelectomy.
The follow-up ranged from 1 to 78 months postoperatively. The highest incidence of hydrocele recurrence/persistence among the included studies was 1.4%. 33 Other complications included conversion (1.79% 30 ), hematoma (1.35% 35 ), subcutaneous emphysema (3.52% 33 ), scrotal edema (0.72% 30 ), wound infection (0.70% 33 ), suture site abscess (0.36% 30 ), umbilical hernia (0.36% 30 ), and contralateral occurrence of hydrocele (0.46% 33 ). Subgroup analysis showed that the type of hydrocele, surgical approach, suture material, and management of hydrocele sac did not significantly influence the operative complications (Table 4).
Potential Risk Factors and Operative Complications
Discussion
It was generally believed that PH and inguinal hernia had the same etiology (i.e., PPV) and then shared a similar surgical principle of correction (i.e., high ligation of PPV).2,3 For communicating hydrocele which was confirmed preoperatively, most authors usually reported the outcomes with those of inguinal hernia together. 3 Furthermore, the two pathologies always had the same treatment methods, including open and laparoscopic repair. 3 Open inguinal repair had been regarded as the standard approach over many years, while laparoscopic technique had gained increasing popularity with the development of minimally invasive surgery.2,3 For the patients with noncommunicating hydrocele or PH not diagnosed as “communicating” before surgery, however, most pediatric surgery specialists only recommended an open groin exploration instead of the laparoscopic surgery.1,2 We speculated that they probably considered the very few noncommunicating hydroceles which did not have a visible PPV and were difficult to process by laparoscopy.
The current review showed that recurrence and other complications were relatively rare after laparoscopic PH repair, with a highest incidence of 1.4% and 3.52%, respectively. 33 The outcomes of comparative studies indicated that the recurrence incidence after laparoscopic repair was not higher but the incidence of other complications was significantly lower than that following open surgery.31,33 These outcomes demonstrated that laparoscopic surgery was a safe and effective approach for PH repair. The included studies reported the excellent outcomes of various PH subtypes (e.g., communicating hydrocele, noncommunicating hydrocele, hydrocele of the spermatic cord, and hydrocele of the canal of Nuck), which showed that laparoscopic repair was not only suitable for communicating hydrocele but also for other PH subtypes in children. Yang et al. 33 found that the vast majority (187/188) of preoperatively diagnosed noncommunicating hydroceles were coexisted with an open internal ring under laparoscopic exploration, and the PPV was also confirmed by injection of methylene blue into internal ring and aspiration of the blue-stained fluid from scrotum. Therefore, the concern of the most specialists which we speculated was just a very small probability event, and it could also be found during the surgery and repaired by a converted open inguinal surgery.
There were several effective techniques of laparoscopic PH repair in the literature. The laparoscopic surgery could be performed through either an intraperitoneal or extraperitoneal approach.2,3 It seemed that surgical approach did not significantly affect hydrocele recurrence as well as other complications. The intraperitoneal approach was usually adopted in the traditional laparoscopic surgery, which warranted mastery in the intracorporeal suturing and knot tying and therefore technically more demanding for the surgeon. Differing from that, the extraperitoneal approach usually required a special device (e.g., hernia needle) to suture the PPV percutaneously and tie the knot extracorporeally.2,3,8 Therefore, it did not need skilled laparoscopic manipulations and could be carried out easily even by the beginners. Nowadays, the extraperitoneal approach had gained more popularity in laparoscopic PH repair.
The site and number of port incisions were usually set according to the surgeon's experience and preference and also presented the trends of increasingly minimal invasiveness and cosmetic effect. Management of the hydrocele sac did not dramatically increase the complication rate, but we did not suggest a routine dissection or transaction of the hydrocele sac because of the potential injury risk to the spermatic cord and testis. Subgroup analysis also showed that the suture material (absorbable versus nonabsorbable) did not significantly affect hydrocele recurrence and other complications. Interestingly, it was not consistent with the results of laparoscopic inguinal hernia repair in children in the literature.8,21,40 However, due to the small number of patients who were treated with absorbable suture, our conclusion tended to be conservative and needed to be confirmed by studies with large sample size in the future.
The current review had several limitations. First, very few studies were included in this review. There were only 20 relevant studies according to the predefined criteria, although it was long since laparoscopy was first used to repair PH in 1994. 11 Second, level of evidence of the included studies was relatively low. Of these studies, most were case series (level 4), and few were retrospective comparative studies (level 3). So far, there were no well-designed prospective studies concerning laparoscopic PH repair. Then, clinical heterogeneity among the included studies was significant. These studies included not only various subtypes of PH but also different surgical techniques and follow-up periods. Finally, the area where the included studies derived was very limited. Most (75%) of the included studies were conducted in Asia (e.g., China, Korea, and Japan), and therefore it was questioned whether our conclusions could be applied to other areas.
In conclusion, laparoscopic PH repair seems to be a safe and effective procedure. Given the limitations of this review, our conclusion needs to be confirmed by more well-designed studies.
Footnotes
Acknowledgments
The authors acknowledge Ningbo Municipal Bureau of Science and Technology (grant number: 2016A610177) for funding the study.
Disclosure Statement
No competing financial interests exist.