
Abstract
Abstract
Background:
Minimally invasive surgery in elderly patients with colorectal cancer remains controversial. The study aimed to compare the operative, postoperative, and oncologic outcomes of robotic (robotic colorectal resection surgery [RCRS]) versus laparoscopic colorectal resection surgery (LCRS) in elderly patients with colorectal cancer.
Methods:
Propensity score matching (PSM) was used to compare patients aged 70 years and more undergoing elective RCRS or LCRS for colorectal cancer between 2010 and 2017.
Results:
Overall, 160 patients underwent elective curative LCRS (n = 102) or RCRS (n = 58) for colorectal cancer. Before PSM, the mean preoperative Charlson score and the tumor size were significantly lower in the robotic group. After matching, 43 RCRSs were compared with 43 LCRSs. The RCRS group showed longer operative times (300.6 versus 214.5 min, P = .03) compared with LCRS, but all other operative variables were comparable between the two groups. No differences were found for postoperative morbidity, mortality, time to flatus, return to regular diet, and length of hospital stay. R0 resection was obtained in 95.3% of procedures. The overall and disease-free survival rates at 1, 2, and 3 years were similar between RCRS and LCRS patients. The presence of more than one comorbidity before surgery was significantly associated with the incidence of postoperative complications.
Conclusion:
In patients aged 70 years or more, robotic colorectal surgery showed operative and oncologic outcomes similar to those obtained by laparoscopy, despite longer operative times. Randomized trials are awaited to reliably assess the clinical and oncological noninferiority and the costs/benefits ratio of robotic colorectal surgery in elderly populations.
Introduction
M
The role of robotics and its theoretical superiority over laparoscopy is under investigation. A recent meta-analysis by Zhang et al. 21 showed that in the general adult population robot-assisted colorectal resection is associated with a lower conversion rate, lower intraoperative blood loss, and shorter hospital stay compared to laparoscopic-assisted surgery. However, no subgroup analysis was done for the specific subset of elderly patients, and data in the literature are scarce and mostly contradictory about the outcomes of robotic colorectal surgery in patients older than 65 years.9,22
The present study aimed to evaluate the operative and oncologic outcomes of robotic colorectal resection surgery (RCRS) compared to laparoscopic colorectal resection surgery (LCRS) in elderly patients (aged 70 years or more) using a propensity score matching (PSM) analysis.
Materials and Methods
Study design and study population
This monocentric PSM study was conducted at the Henri Mondor University Hospital of Créteil (France). Patients underwent surgery between January 2010 and March 2017. To be included in the study analyses, the following criteria should be met: solitary adenocarcinoma of the colon or the rectum, American Joint Committee on Cancer tumor, nodes, and metastasis stage I to IVa, 23 and elective curative-intent colorectal resection by either laparoscopic or robotic approach. Demographics, perioperative oncological treatments, and intraoperative, operative, and postoperative outcomes were prospectively recorded into the colorectal database of the surgical unit. The study was conducted in accordance with the ethical principles described in the Declaration of Helsinki.
Surgical techniques
The decision to perform LCRS and RCRS was taken for each individual patient in a multidisciplinary meeting. Both laparoscopic and robotic surgeries were completely refunded by the national insurance system and not associated with extra costs for the patient. Two senior colorectal surgeons experienced in minimally invasive surgery performed all LCRS and RCRS using the same oncological and technical principles, with pure laparoscopic and robotic techniques. Based on tumor location, the appropriate surgical procedure was selected, including right colectomy, extended right colectomy, transverse colectomy, left colectomy, and “up-to-down” anterior rectal resection with partial or total mesorectal excision (TME).24,25 All laparoscopic and robotic colorectal resections were performed according to standard techniques developed for laparoscopic surgery using a medial-to-lateral approach for radical operations, as previously reported.26–31 The ileocolic and colorectal anastomoses were performed either intracorporeally or extracorporeally. 32 Tumors infiltrating the external sphincter muscles were managed by abdominoperineal resection. Temporary loop ileostomy was performed for patients undergoing rectal resection with TME, with ileostomy closure 2 months afterward. Hartmann's operation or colonic resection with stoma diversion (i.e., double-barreled ileocolostomy and double-barreled colostomy) was performed in patients presenting with risk factors contraindicating colorectal anastomosis (e.g., poor nutritional status). Conversion was defined as the need to shift from laparoscopy to open surgery or from robotic to laparoscopic or open surgery to complete the procedure. 33
Operative and short-term outcomes
Operative outcomes included operative time, conversion to laparoscopy, conversion to laparotomy, intraoperative blood loss, intraoperative blood transfusion, and intraoperative complications. Short-term outcomes included postoperative morbidity and mortality (recorded up to 90 days after surgery), reoperation rate, time to flatus, time to resume a regular diet, postoperative blood transfusion, length of hospital stay, and readmission within 60 days. Type and severity of postoperative complications were assessed by Dindo-Clavien classification, 34 and it included the following: cardiovascular complications, respiratory and urinary tract infections, wound infection, kidney failure, prolonged ileus, stoma-related complications, intra-abdominal abscess, and anastomosis-related complications. In rectal cancer patients, anastomotic leakage was categorized as grade A, B, or C according to the International Study Group of Rectal Cancer (ISGRC) classification. 35
In addition, the total costs per patient, including the surgery-related costs (e.g., costs of anesthesia, consumable, surgical materials, and instruments), plus the hospitalization-related costs (e.g., length of hospital stay) were analyzed and compared between LCRS and RCRS.
Pathologic outcomes
The involvement of the resection margins (i.e., R0 versus R1) and the number of lymph nodes harvested were evaluated on the surgical specimen. In rectal cancer patients, the quality of the mesorectum was scored as “complete,” “nearly complete,” or “incomplete.” 36 The circumferential resection margin (CRM) was considered as adequate if >1 mm, 37 whereas the distal resection margins (DRM) should be at least 5 cm below the tumor for lesions of the colon and high rectum, 38 at least 2 cm below the tumor for lesions of the mid-rectum and >1 mm below the fixed section of the distal margin for lesions of the low rectum. 39
Survival outcomes
The oncologic follow-up program was planned every 3 months for the first 2 years and every 6 months thereafter, and it consisted of blood tests (e.g., carcinoembryonic antigen levels) and imaging studies (e.g., total body computed tomography [CT] scans or abdominal ultrasound). A full colonoscopy was scheduled within the first 2 years after surgery. Magnetic resonance imaging and/or positron emission tomography-CT were performed when cancer recurrence was suspected. Overall survival (OS) and disease-free survival (DFS) rates were compared between LCRS and RCRS groups. Cancer recurrence was classified as local when involving the anastomosis or any structure in the pelvis or distant when occurring outside the pelvis.
Statistical analyses
Patients who required conversion from laparoscopic to open surgery or from robotic to laparoscopic or open surgery were retained in their original group (LCRS or RCRS) based on an intention-to-treat analysis.
The PSM was used to minimize potential selection bias and compare the treatment effects by taking into account all covariates that may influence the selection of the surgical approach,40,41 namely laparoscopy or robotic surgery. Propensity scores were estimated using logistic regression and including in the model the following covariates: age, gender, body mass index, American Society of Anesthesiologists score, tumor size, tumor location, type of surgical procedure, American Joint Committee on Cancer stage, preoperative treatments, multivisceral resection, and year of surgery. The year of surgery was added to control for potential historical bias. A 1:1 “nearest neighbor” case–control match without replacement was applied, 42 meaning that each patient treated by robotic surgery was matched with 1 patient treated by laparoscopy who had the closest estimated propensity score.
According to the type of variable, chi-squared test, Fisher's exact test, or Mann–Whitney U test were used for the bivariate two-sided comparisons between the LCRS and RCRS groups. Univariate and multivariate analyses were run to identify factors significantly associated with postoperative complications. OS and DFS rates were estimated at 1-, 2-, and 3 years after surgery using Kaplan–Meier method and compared between LCRS and RCRS using the log rank (Mantel–Cox) test. Statistical significance was set at P < .05. SPSS (Statistical Package for Social Science, IBM SPSS Statistics, Version 23 for Macintosh; IBM Corp., Armonk, NY) was used.
Results
Overall, a total of 160 patients aged 70 years or more who underwent elective curative LCRS (n = 102) or RCRS (n = 58) for colorectal cancer were selected. Demographic, clinical, and histopathological characteristics of the entire study population are outlined in Table 1. The mean preoperative Charlson score and the tumor size (largest dimension) were significantly lower in the robotic group.
Bold or italic numbers identify significant p values.
AJCC, American Joint Committee on Cancer; APR, abdominoperineal resection; ASA, American Society of Anesthesiology; BMI, body mass index; CEA, carcinoembryonic antigen; LCRS, laparoscopic colorectal resection surgery; PME, partial mesorectal excision; RCRS, robotic colorectal resection surgery; SD, standard deviation; TME, total mesorectal excision; TNM, tumor, nodes, and metastasis score.
Study population after PSM
After matching, no covariate had a standardized mean difference of >0.25 between the LCRS and RCRS groups, suggesting an accurate model. Thus, the PS-matched LCRS and RCRS groups were compared with respect to the study endpoints (Table 2). No significant difference was observed in the demographic, clinical, or histopathological characteristics. Similarly, no differences were found for tumor location and type of surgical procedure. The majority of the tumors were located in the right colon (51.2%), in the left colon (19.8%), or mid-rectum (10.5%). Temporary diverting loop ileostomy was performed in 9 (20.9%) patients in the LCRS group and 7 (16.3%) patients in the RCRS group (P = .782). No multivisceral resection was required. Tumor stage, tumor grade, tumor size, and the rates of lymphovascular and perineural invasion were similar between groups. Overall, 27.9% of patients were administered with adjuvant treatments.
AJCC, American Joint Committee on Cancer; APR, abdominoperineal resection; ASA, American Society of Anesthesiology; BMI, body mass index; CEA, carcinoembryonic antigen; LCRS, laparoscopic colorectal resection surgery; PME, partial mesorectal excision; RCRS, robotic colorectal resection surgery; SD, standard deviation; TME, total mesorectal excision; TNM, tumor, nodes, and metastasis score.
Operative, postoperative, and pathologic outcomes
Operative time was significantly longer in the RCRS group (214.5 for LCRS versus 330.6 minutes for RCRS; P = .034) (Table 3). No conversion occurred. The estimated intraoperative blood loss was similar between the LCRS and RCRS patients, with no need for blood transfusion. No intraoperative complication occurred.
Bold numbers identify significant p values.
LCRS, laparoscopic colorectal resection surgery; NA, not applicable; RCRS, robotic colorectal resection surgery; SD, standard deviation.
The overall postoperative morbidity rate was 40.7%; no difference was found for the type and severity of postoperative complications between the LCRS and RCRS groups. The incidence of severe complications (Dindo-Clavien >2) was 8.1%. Medical complications occurred in 17.4% of patients. Anastomotic leakage occurred in 9 patients (10.5%). Three patients had anastomotic leak after right colectomy, treated by antibiotics (n = 1) or laparotomy (n = 2) with abdominal cavity lavage and drainage in one case and surgical drainage of an intra-abdominal abscess in the latter. The remaining six anastomotic leakages occurred in patients who had undergone anterior rectal resection with TME. Three of these were classified as ISGRC grade A and no active therapy was required, whereas the other three were classified as ISGRC grade B and were treated by antibiotics and radiologic drainage. Two other patients in the LCRS group required reoperation: 1 patient who underwent right colectomy was reoperated for umbilical trocar evisceration; and the other one, who underwent anterior rectal resection with TME, was reoperated for abdominal aortic aneurysm repair. The length of hospital stay was 14.8 days in the LCRS group versus 11.7 days in the RCRS group (P = .08). The overall 90-day mortality rate was 1.2%.
The mean number of lymph nodes harvested was not different between the two surgical approaches, with 12 or more lymph nodes harvested in the majority of patients (n = 62, 72%). R0 resection was obtained in the majority of procedures (n = 82, 95.3%). Concerning the patients with rectal cancer (n = 23), no difference was found concerning the quality of mesorectal excision between the two groups. In the LCRS group (n = 13), 10 patients (76.9%) had a complete mesorectal excision, 2 (15.4%) nearly complete, and 1 (7.7%) incomplete. In the RCRS group, all 10 patients (100%) had a complete mesorectal excision (P = .265). Positive CRM was found in 2 patients (15.4%) in the LCRS group and 2 patients (20%) in the RCRS group (P = 1). The mean distance of the CRM was 5.34 mm (standard deviation [SD]: 4.34) for the LCRS group and 8.5 mm (SD: 6.7) for the RCRS group (P = .257). Positive DRM were found in only 1 patient (7.7%) in the LCRS group. The mean distance of the DRM was 32.53 mm (SD: 18.21) for the LCRS group and 32.1 mm (SD: 19.25) for the RCRS group (P = .648).
Overall, adjuvant therapy was administered in 24 patients (13 LCRS and 11 RCRS patients; P = .292). Based on the histopathological specimen examination, 7 additional patients (22.5%) should have received adjuvant treatments, but they were unfit for it.
In the multivariate regression analysis, only the variable “more than one comorbidity” appeared to be an independent factor significantly associated with the incidence of postoperative complications (Table 4).
Multivariate analysis included the variables that reached a significant P value on the univariate analysis.
Bold italic numbers identify significant p values.
AJCC, American Joint Committee on Cancer; ASA, American Society of Anesthesiology; BMI, body mass index; CI, confidence interval; LCRS, laparoscopic colorectal resection surgery; RCRS, robotic colorectal resection surgery.
Regarding the healthcare cost analysis, the RCRS cost a mean of 19,116 euros (SD: 10,622), whereas LCRS cost 16,162 euros (SD: 11,656). No significant group difference was found (P = .104).
Survival outcomes
The mean follow-up time was 24.6 (SD: 18.6) months for the LCRS group versus 24.3 (SD: 12.6) months for the RCRS group (P = .606). The OS rate at 1-, 2-, and 3 years was, respectively, 87.6%, 78.5%, and 70.7% for the LCRS group and 89.9%, 85.4%, and 74.7% for the RCRS group (P = .213) (Fig. 1). The DFS rate at 1-, 2-, and 3 years was, respectively, 86.3%, 77.4%, and 62.4% for the LCRS group and 84.7%, 80.3%, and 76.5% for the RCRS group (P = .520)(Fig. 2). Over a mean follow-up time of 24.44 months, disease recurrence was observed in 7 (18.4%) LCRS patients and 6 (14.6%) RCRS patients (P = .765). One patient (1.3%) presented with local recurrence and 12 patients (15.2%) with distant metastases, including solitary pulmonary metastasis (n = 3, 3.9%), solitary liver metastasis (n = 1, 1.3%), pulmonary + liver metastases (n = 1, 1.3%), peritoneal carcinomatosis (n = 3, 3.9%), and systemic metastasis disease (n = 4, 5.2%). No group difference was observed.
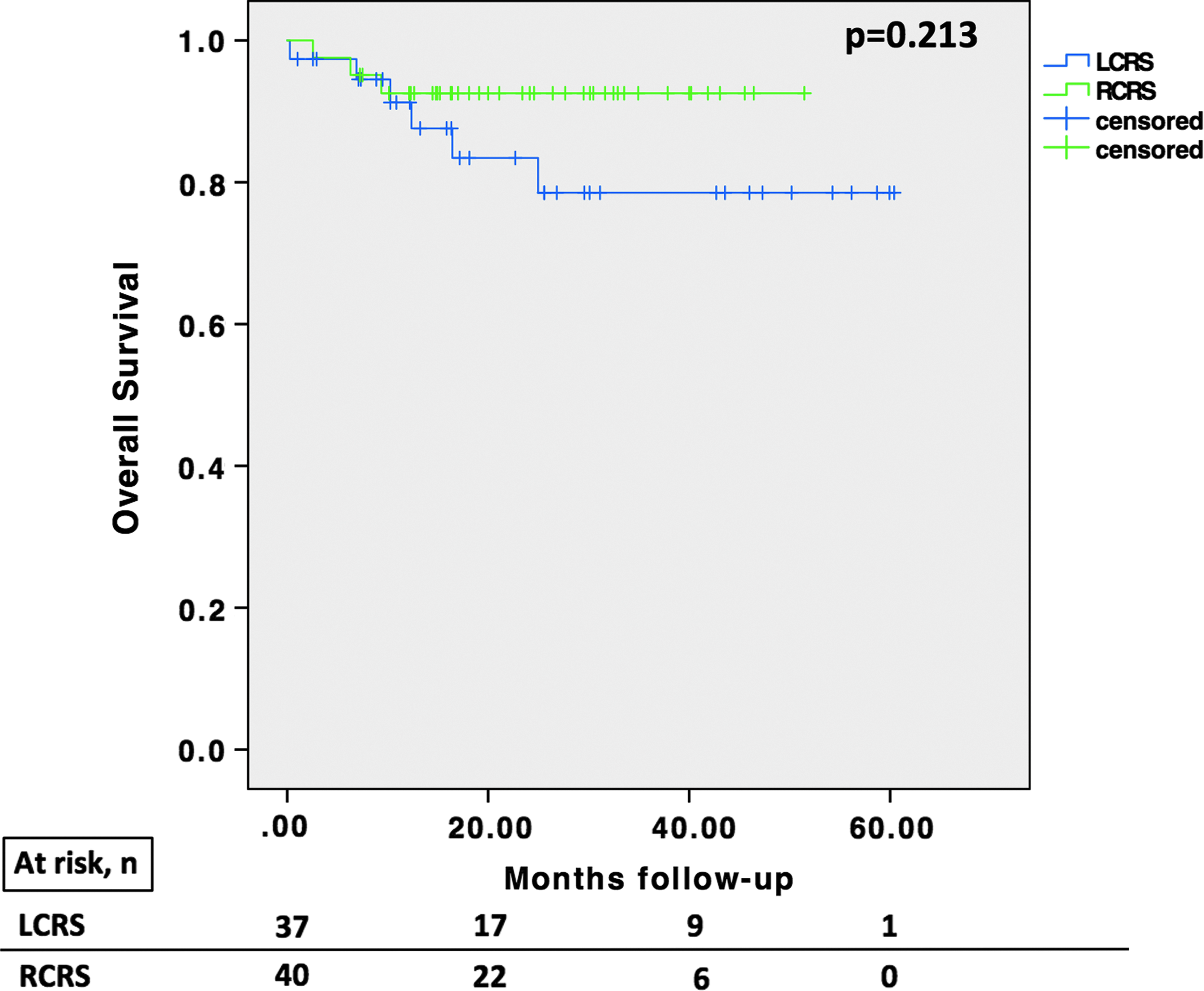
Overall survival of elderly patients undergoing RCRS or LCRS. LCRS, laparoscopic colorectal resection surgery; RCRS, robotic colorectal resection surgery.
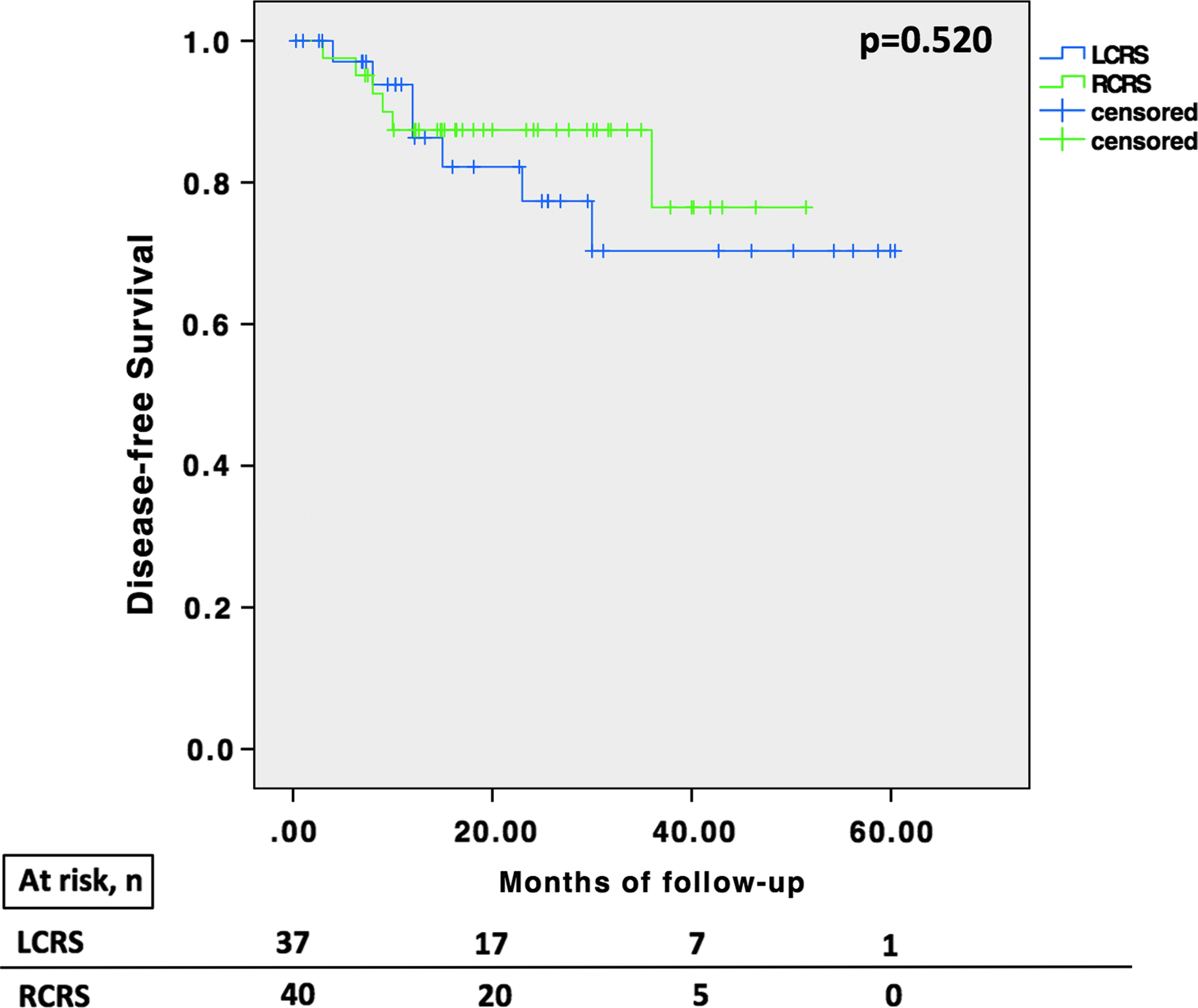
Disease-free survival of elderly patients undergoing RCRS or LCRS. LCRS, laparoscopic colorectal resection surgery; RCRS, robotic colorectal resection surgery.
Discussion
The present study showed that robotic surgery is a safe and feasible approach for colorectal cancer resection in patients aged 70 years or more. By applying a PSM analysis, RCRS and LCRS are associated with similar operative, postoperative, and oncologic outcomes, except for operative times that are longer for RCRS. The patient's age and the type of surgery were not predictors of worse postoperative outcomes; conversely, the presence of more than one comorbidity significantly increased the risk of postoperative complications.
In the literature, age was often found as an independent risk factor for postoperative mortality and morbidity in surgical oncology 43 ; however, evidence supports that it is not the actual age of the patient to constitute a risk for surgery, rather the quality of aging and the functional status that define the condition of frailty.44–46 In geriatrics, frailty is the syndrome of decreased physiologic reserve and increased vulnerability that limit the ability of the patient to respond to stress while increasing the risk for poor health outcomes, including falls, incident disability, hospitalization, and mortality. 47 The present results confirm that age per se is not a risk factor for worse postoperative outcomes, rather the presence of multiple comorbidities before surgery, which can be considered as an indicator of frailty, is a risk factor for the development of postoperative complications. This is of high importance because it has been shown that a complicated postoperative course in elderly has a drastic impact on survival in the first year after surgery. 48 Then, for survivors of this early postoperative period, cancer-related survival of elderly appeared to be comparable to younger patients who had undergone colorectal surgery.2,49 In this prospective study, the choice of the surgical approach and technique acquires a cardinal role to minimize the surgical invasiveness and improve recovery.8,10 Moreover, it must be considered that a high proportion of patients older than 70 years (estimated in this study at 22.5%) may be unfit to receive adjuvant treatments3,6; this highlights once more the importance of achieving optimal oncologic results with surgery in elderly patients.
If clinicians and researchers agree that curative—intent surgery should not be denied exclusively based on age, which is the best surgical approach to apply in elderly, is still a matter of debate. Robotic colorectal surgery may be considered as an evolution of conventional laparoscopy with a computer interface that facilitates intuitive movements similar to open surgery. 22 Indeed, it is characterized by improved depth perception, improved dexterity and movement control, and improved surgeon ergonomics compared to laparoscopy.21,29,50–52 Particularly for colorectal resections, recent studies supported a lower rate of conversion and a faster learning curve when performing robotic-assisted procedures.29,53,54 However, these technical advantages may not directly or yet translate into improvements of clinical outcomes. Indeed, the present results showed that there are no differences between RCRS and LCRS in the intraoperative variables and incidence of complications; although supporting the safety and feasibility of robotics in elderly patients, there is not clear advantage over conventional laparoscopic surgery. Moreover, RCRSs are significantly longer operations than LCRS. This may be only partially explained by the robotic docking and installation time that are added up to the effective procedure duration.55,56 Operative time remains a critical issue because a longer operative time means longer anesthesia time and longer pneumoperitoneum time, which may have an impact especially in elderly and frail patients.57–59 In this study, however, no differences in postoperative outcomes were noted between the two groups, despite longer operative times for the RCRS procedures. It must be mentioned that both surgical approaches are characterized by a minimally invasive access and the induction of pneumoperitoneum. The eventual positive and negative effects of these techniques are very similar, such as the adverse hemodynamic effects related to the pneumoperitoneum or the required steep Trendelenburg and tilt patient positions.58,60 Interestingly, both techniques were well tolerated by elderly patients; no conversion to laparotomy was required, and no anesthesia-related complication occurred.
Overall postoperative morbidity, including surgical and nonsurgical complications, and 90-day mortality were equivalent between RCRS and LCRS and in accordance with the ranges reported in the literature.7,9,22,59,61 Laparoscopy has been shown to be associated with decreased times to flatus and time to regular diet16,62 compared to the open colorectal surgery. These results were not clearly evaluated or confirmed for the robotic approach.20,63,64 However, it may be advocated that robotic and laparoscopic approaches may have a similar surgical impact that leads to similar effects on gastrointestinal functions, postoperative pain, and recovery, as supported by similar time to flatus, time to resume regular diet, and length of hospital stay between RCRS and LCRS. Similarly, for the oncologic outcomes of surgery, robotics appeared to lead to an optimal quality of oncologic resections (adequate number of harvested lymph nodes and complete mesorectal excision in rectal cancer). This translated in good 1, 2, and 3-year OS and DFS that are comparable to those observed in elderly patients operated on by laparoscopy.65,66 In addition, RCRS and LCRS appeared to be comparable also for the related healthcare costs. This may be explained by the optimization of surgical materials by a surgical team expert in minimally invasive surgery and by a slightly lower hospital stay in the RCRS group.29,67,68 This result, however, should be interpreted with caution since the present cost analysis underestimates the global costs of surgery due to the fact that the acquisition costs, maintenance costs, and amortization period were not taken into account. It is clear that robotic surgery is not a cost-saving alternative 64 ; indeed, to identify the advantages and indications of robotics, future studies should evaluate patient- and surgeon-centered endpoints, which might be more sensible to highlight the potential benefits of this minimally invasive surgical technique that is gaining global utilization.
The present study has strengths and limitations. In our knowledge, this is the largest study evaluating robotic colorectal surgery in elderly patients and comparing it to laparoscopy.9,22 The retrospective nature of the study embeds potential bias. However, the PSM method is considered the best statistical analysis to manage retrospective data from nonrandomized controlled trials, minimize selection bias, and compare 2 homogeneous groups of patients.28,30, 69–71
In conclusion, the present results show that in patients aged 70 years or more, robotic colorectal surgery can achieve operative and oncologic outcomes similar to those obtained by laparoscopy, despite longer operative times. Further randomized controlled trials are needed to assess the noninferiority of robotic surgery in terms of clinical and oncological outcomes and to reliably evaluate the costs/benefits ratio of robotic surgery for elective and potentially curative colorectal cancer resections in elderly patients.
Footnotes
Disclosure Statement
No competing financial interests exist.