
Abstract
Abstract
Objective:
To compare perioperative outcomes of robotic single-site (RSS) surgery with conventional single-port laparoendoscopic surgery for the treatment of advanced-stage endometriosis.
Materials and Methods:
This is a retrospective cohort study that included 120 patients who received single-port laparoendoscopic surgery or RSS surgery for the treatment of advanced-stage endometriosis at Ewha Womans University's Mokdong Hospital in Seoul, Korea between December 2014 and May 2017. Single-port laparoendoscopic cystectomy and adhesiolysis were performed in 52 patients (Single-port laparoendoscopic [SPL] group) and RSS cystectomy and adhesiolysis were performed in 68 patients (RSS group). Perioperative outcomes that we analyzed, included age, operative time, estimated blood loss, length of hospital stay, size of endometriosis, laterality of endometriosis, degree of endometriosis infiltration (i.e., deep versus not), and recurrence.
Results:
The patients in both groups were of similar ages. Longer operative times (107.8 ± 37.6 min for RSS group versus 76.9 ± 46.4 min for SPL group, P = .001) and more estimated blood loss (106.67 ± 171.67 mL for RSS group versus 57.1 ± 44.9 mL for SPL group, P = .001) were measured in the RSS group. However, the mean size of endometriosis was statistically larger (5.23 ± 2.53 cm for RSS group versus 4.37 ± 2.14 cm for SPL group, P = .030) and higher rates of more deeply infiltrative endometriosis (52 cases in RSS group, 76.5% versus 33 cases in SPL group, 63.5%) were observed in RSS group. Multicystic endometriosis occurred in 26 cases in the RSS group (38.2%). No significant differences were seen in terms of length of hospital stay (4.58 ± 0.61 of SPL group versus 4.59 ± 0.58 of RSS group, P = .862) or intraoperative and postoperative complications between the groups. Recurrence occurred in one case in the RSS group (1.9%).
Conclusion:
RSS surgery can be used in the treatment of advanced-stage endometriosis, especially in more complicated cases.
Introduction
Endometriosis is a chronic gynecologic disorder that involves one or several areas of the pelvis and abdomen, and this affects a significant number of women worldwide. 1 Endometriosis can negatively impact ovarian reserve by invading the ovarian cortex, cause pain by adhering the ovaries to the pelvis, and raise the suspicion of ovarian malignancy. To maintain the follicular reserve and ovarian function, safe and radical resection of endometriosis is necessary.
Single-port laparoendoscopic (SPL) surgery is a minimally invasive approach used nowadays, in which the entire procedure is performed through a single incision. 2 SPL surgery is safe and feasible in a wide variety of benign and malignant gynecologic conditions. However, there are some limitations associated with SPL removal of endometriosis due to the rigidity of the instruments used. It is difficult to identify an appropriate plane, especially in cases of deep-seated endometriomas that are thick and adhered to the cul-de-sac, to use to perform a complete excision via the single-port laparoendoscopic approach.2–4
Therefore, a robotic approach is often applied to the resection of deep-seated endometriomas found in the bladder and rectum, including with respect to the excision of ovarian cysts.5–7 Beginning with the introduction of a single-site platform to the da Vinci® System in 2013, the performance of robotic single-site (RSS) surgery has been increasingly prevalent to the field of gynecologic surgery due to the ability of single-port laparoscopy to reduce pain and improve the satisfaction of patients. 8
In this study, we aimed to compare perioperative outcomes of RSS surgery versus single-port laparoendoscopy, following the treatment of advanced-stage endometriosis, and to determine whether RSS surgery is feasible and safe with potential advantages for the treatment of advanced-stage endometriosis.
Materials and Methods
We retrospectively collected data on a total of 120 cases of RSS ovarian cystectomy and adhesiolysis (RSS group) using the da Vinci Si System with Single-Site™ platform or single-port laparoendoscopic cystectomy and adhesiolysis (SPL group) at Ewha Womans University Medical Center in Seoul, Korea between December 2014 and May 2017. There was not any clinical criterion on the choice for SPL and RSS approach. Patients who were planning to undergo either SPL or RSS approach were counseled about the two types of surgery, including the cost. The choice was not affected by a surgeon's factor, including surgeon's preference or a particular operation day. We included all the consecutive endometriosis cases that underwent SPL or RSS, therefore, the baseline clinical differences between the two groups (deep infiltrating endometriosis [DIE] and cyst size) were not intended.
The procedure of RSS cystectomy was as follows: after general anesthesia, the patient was prepared by placing a uterine mobilizer and a Foley catheter. For RSS ovarian cystectomy, we applied the da Vinci Single-Site platform with silicone Single-Site port, a curved cannula, and flexible Single-Site instruments. Transumbilical skin incision of vertical length 2.7 cm was made, and the fascia layer was opened using the open Hasson technique. Approximately 3 cm incision on the underlying fascia and peritoneum level was made for an adequate surgical movement. A wound retractor (MEDEN, Inc., Seoul, Korea) was inserted into the fascia opening to facilitate the specimen removal procedure near the end of the surgery. The silicon Single-Site port was inserted through the opening covered with wound protector. Afterward, pneumoperitoneum was created by infusing carbon dioxide gas up to 12 mmHg. While the patient was placed in a 20-degree Trendelenburg angle position, the 30-degree 8.5 mm da Vinci stereo laparoscope connected to the robotic system camera was inserted to confirm atraumatic placement of its primary port, and upon confirmation, camera was removed. Afterward, the robotic system was driven in and positioned between the patient's legs and docked at the camera port. After docking, the two 5 mm curved instrument cannulas were inserted into the robotic arms and the semirigid instruments were placed under careful stereo laparoendoscopic guidance. Flexible robotic monopolar hook and fenestrated bipolar forceps were mounted through the curved cannulas. The robotic system enabled a switching motion between right-hand and left-hand orientations. 9
We assessed the entire ovarian cysts with adhesion and the endometriotic spots to expose the ovarian capsule using the monopolar hook (Fig. 1). Extraction of endometriotic cysts from the ovary was done using the monopolar hook through repeated electrocauterization and cut, while the bipolar forceps and wristed needle driver were used to keep the cysts in traction. The remnant ovary was sutured with a wristed needle driver by continuous running stitches with 2-0 Vicryl® sutures (Covidien, Dublin, Ireland) (Fig. 1). The extracted endometriomas were placed into an Endopouch® specimen retrieval bag (Ethicon, Somerville, NJ), which was then easily removed through the wound retractor (MEDEN, Inc.). After the specimens were removed, the single-site port was reinserted and reusable straight robotic cannulas were placed for the final assessment of the pelvic cavity as well as for the irrigation of the blood. Absorbable continuous locking sutures were used to close the fascia and subcutaneous layer with 3-0 Vicryl sutures (Covidien).
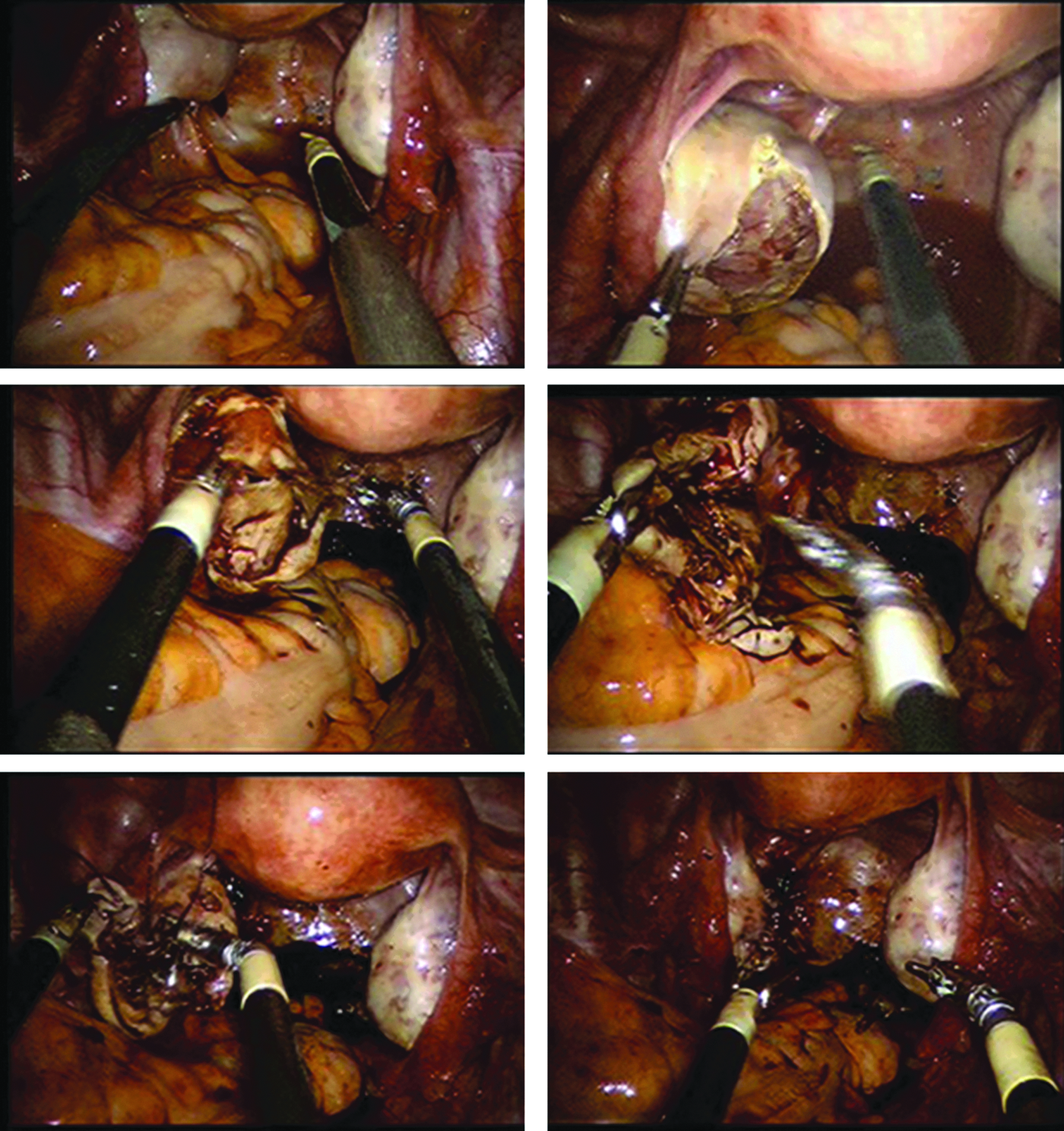
An example of an RSSC procedure. RSSC, robotic single-site cystectomy.
The methodology of SPL cystectomy was same as that of RSS cystectomy except with respect to the instruments used and the performance of the surgery. We performed SPLC through a GELPASS one-port system (MEDEN, Inc.) with two 5 mm trocars, one 1 cm trocar, a wound retractor, and a specialized silicone cover. We used traditional laparoendoscopic instruments such as ovarian forceps, monopolar metzenbaum scissors, and needle holders. The processes of cystectomy, adhesiolysis, and suture were the same.
All surgical steps were performed by 3 gynecologic surgeons who were well experienced in robotic and laparoendoscopic surgeries. At the time of this study, all 3 had participated in more than several 100 cases of robotic multisite surgery and had completed RSS surgery training and earned an RSS surgery certificate.
We enrolled data on patients' characteristics and perioperative surgical outcomes, such as age, parity, and body mass index (BMI). Also, we analyzed perioperative factors of the included subjects such as age, operative time, estimated blood loss, length of hospital stay, size of endometriosis measured by pelvic ultrasonogram, laterality of endometriosis, presence of DIE, and recurrence rate.
The criteria of discharge in our hospital are as follows: (1) the patient should be afebrile and no sign of complication, including postoperative infection, (2) the patient should have no problem in gas passing and be tolerable to soft oral diet, and (3) the patient should be able to return to daily life under oral nonsteroidal anti-inflammatory drugs (NSAIDs) without major limitation or severe pain.
We followed the definition of DIE of Donnez and Nisolle in 1995, that is the invasion of a very active peritoneal lesion deep in the retroperitoneal space, lateral peritoneal invasion in utero-sacral ligaments, as well as the anterior wall of the rectosigmoid bowel junction resulting in a retraction, adhesions, and secondary obliteration of the cul-de sac. The 5 mm invasion depth of DIE was confirmed pathologically, and we did not perform a preoperative MRI in all cases for evaluation of the presence of DIE.
We analyzed the data of 120 cases statistically with a Student's t-test, a chi-squared test, and Kruskal–Wallis test using SPSS Statistics version 20. We had received the approval of this study by the Institutional Review Board of our institute.
Results
All the patients underwent successful surgeries completely without conversion to other multiport laparoendoscopic cystectomy or robotic cystectomy in both groups. Parity was under one in each group (Table 1, 0.4 ± 0.8 for SPL group versus 0.2 ± 0.5 for RSS group). The mean BMIs (in kg/m2) of the subjects were not different between the two groups (21.1 ± 3.0 for SPL group versus 23.1 ± 3.4 for RSS group). The levels of CA 125 were similar in both groups.
The Clinical Characteristics of Cases in Both Groups
NS, not specific; RSS, robotic single-site; SPL, single-port laparoendoscopic.
The mean total operation time was longer in the RSS group (107.8 ± 37.6 minutes) with respect to docking time (not shown), than in the SPL group (76.9 ± 46.4 minutes, P < .01). The mean estimated blood loss in the SPL group (57.1 ± 44.9 mL) was less than that of the RSS group (135.6 ± 143.9 mL, P < .01), but the mean size of endometriosis in the SPL group (4.37 ± 2.14 cm) was smaller than that of the RSS surgery group (5.23 ± 2.53 cm, P = .030) (Table 2).
Perioperative Variables of Cases from the Two Groups
DIE, deep infiltrating endometriosis; EMS, endometriosis; RSS, robotic single-site; SPL, single-port laparoendoscopic.
The DIE rate was 76.5% in the RSS group and 63.5% in the SPL group. There was no statistically significant difference in the proportion of endometrioma in both groups. Endometrioma was all found in both groups. But DIE spots, which were the invasion of peritoneal lesion deep in utero-sacral ligaments as well as the anterior wall of the rectosigmoid bowel junction, resulting in adhesions and secondary obliteration of the cul-de sac, were differently found in both groups, and those DIE spots in peritoneum and ligament were almost removed.
The incidences of multiple cysts were 38.2% in the RSS group and 32.7% in the SPL group. In comparison with in the SPL surgery group, in the RSS group, the cases demonstrated more deeply infiltrating endometriosis and more cysts were present. Laterality was the same in both groups (25.5%). There was just one recurrent case in the RSS group. The recurrence in pain and endometrioma during US surveillance were regarded as the recurrence of endometriosis. The visualization of round-shaped homogeneous hypoechoic cyst of low-level echoes within the ovary was defined as characteristic ultrasonographic finding of endometrioma. The recurrence was confirmed by reoperation. Everyone got same surveillance. All the patients who underwent surgery for endometriosis in our hospital have been scheduled to have a follow-up visit every 6 months.
The duration of hospital stay was similar among the two groups. Postoperatively, no complication was associated with both groups such as infection or dehiscence, and all patients were satisfied with the cosmetics.
In this study, all cases were tolerable of routine patient-controlled analgesics (PCAs) or nonsteroidal anti-inflammatory drugs administered intravenously (IV) for postoperative 2 days. In terms of postoperative pain evaluation, most patients who undergo surgery under general anesthesia use the PCAs system in our hospital. In PCAs, 0.5 μg per body weight (kg) of fentanyl was IV injected as a rescue analgesic. Then, intravenous analgesics were switched to oral analgesics. Pain was scored by a blinded observer using a verbal numerical rating scale (VNRS: 0 = no pain, 10 = the most severe pain imaginable) at rest, while coughing at 1, 6, 12, 24, and 48 hours after postanesthesia care unit admission.
None of the patients in the study complained about postoperative pain.
Discussion
Due to medical and technological developments, minimally invasive surgery is currently a safe option. The introduction of a robotic surgical system has helped surgeons to overcome the technical challenges of laparoendoscopy by improving surgeon dexterity, surgical precision, and visualization.10,11
Laparoendoscopic single-port surgery presents an opportunity for potentially scarless, minimally invasive surgery. However, there are technical and surgical difficulties due to limitation of space and movement, which lead to conflict among instruments.12–14 In contrast to laparoendoscopic single-port surgery, the da Vinci Single-Site robotic surgical system solves this problem of the conflict among instruments with better visualization and depth perception. Therefore, surgeons can perform the removal of endometriosis by RSS surgical technique easier than by SPL surgical technique, even though we cannot compare the variables statistically in both groups.
In comparison with SPL surgery, surgeons can guide the stereo laparoscope to the operative target site very closely with more magnification and can perform adhesiolysis of the endometriotic tissues by maintaining the original planes by curving the da Vinci Single-Site robotic flexible instruments. This enables surgeons to perform adhesiolysis of the endometriotic tissues much easier than using a conventional laparoendoscopic system. Because the RSS system is also ergonomical and more comfortable for surgeons to use, we can also position the tip of the da Vinci Single-Site robotic instrument parallel to capsules of endometrioma and separate the ovarian tissues or capsules from endometriomas more easily without unintended rupture of such in the RSS surgery group. Therefore, we can perform the removal of endometriosis much easier and more completely without loss of normal ovarian tissues.
For endometrioma over 3 cm, the tense capsule of endometrioma in unruptured state make it difficult to grasp and hold with laparoendoscopic forceps during operation. Therefore, we recommended surgical technique for endometrioma over 3 cm, make a small incision on endometrioma and suction out the cyst contents offer a more easy to grasp the capsule of endometrioma. However, the spilled endometriotic fluids can trigger inflammation in other tissues, even though the endometriotic fluid contents were suctioned out completely in the pelvic cavity. With RSS cystectomy, we can create an adequate hole and suction the contents out through the hole in the endometrioma's pocket after peeling off the capsules so as not to spread the contents out. This method is very helpful to maintain a clear operative field and refrain from enflaming other nearby tissues. It is reported that inflammasome is a key pathogenic mechanism in endometriosis with regulating innate and adaptive host response that surveys the cytosol and other compartments into the cell. Endometriosis has been related with IL-1β and another Noll-Like Receptor (NLR) proteins NLR, Nlrp7 of four inflammasomes, which activate the production of IL-1β and IL-18 that induce a host response such as pyroptosis, a proinflammatory cell death, and the secretion of leaderless cytokines and growth factors. Those factors are correlated with myometrial invasion in human endometrial cancer tissue. 15
In this study, when we compared the perioperative variables between both groups, the following findings were realized. First, the mean total operation time in the RSS group (107.8 ± 37.6 minutes) was longer than that in the SPL group (76.9 ± 46.4 minutes, P < .01). The DIE rate and multiple cyst rate were 76.5% and 38.2% in the RSS group, which were higher than those in the SPL group. The longer total operation time in the RSS group could be related with the complexity of endometriotic cyst and DIE rates even though docking time was added to the operative time. In the RSS group, there were larger cysts removed (5.23 ± 2.53 cm, P = .030), compared with those removed in the SPL group (4.37 ± 2.14 cm). The longer total operating time also could be related with the size of endometriosis as well. To define which surgery shows better perioperative outcomes, we must study more complicated endometriotic cases treated by RSS surgery and SPL surgery further.
In addition, the laparoendoscopic single-port surgery technique places limits for suturing, while RSS surgery is better for the meticulous suturing of ovarian tissues with flexible and rotated instruments. Restoring ovarian features with suturing edges is very easy using RSS cystectomy and may help preserve ovarian follicles as well.
In our study, DIE rates were higher in RSS group than that in SPL group (76.5% versus 63.5%). We removed most of DIE spots except that in bowel in both groups. With RSS surgery, we could remove DIE spots with easy near approach of its location and more magnification.
This is true despite the one case of recurrence that occurred in the RSS surgery group in this study. In the future, we will also evaluate the recurrence rate by including more cases, so as to determine which surgery is ideal for reducing the recurrence rates. The findings of this study, however, suggest that RSS surgery can be used in the treatment of advanced-stage endometriosis, especially in more complicated cases.
This study has limitations regarding obtaining a good conclusion because we enrolled endometriotic cases treated via RSS surgery or SPL surgery performed by 3 different surgeons with more SPL experience than RSS surgical experience. To compare the operative benefits of the two procedures, we must enroll a larger number of endometriotic cases so that the perioperative variables will not be affected by operative experience. Therefore, we will continue to study further for defining the advantages of RSS surgery and SPL surgery.
There are many benefits to the use of RSS surgery and SPL surgery. In terms of better cosmetics for RSS surgery, we mean that RSS surgery is superior in cosmetics comparing multiport laparoendoscopic or robot-assisted laparoendoscopic surgery and a lesser degree of pain due to just the one wound.
Nevertheless, these surgeries have limits. First, the two systems have limited range of motion compared to multisite robotic surgery or laparoendoscopic surgery, but the da Vinci Single-Site robotic system provides a wider range of transverse motion compared with the SPL surgery system (Fig. 2). We can further improve the instrumental range of motion in RSS surgery by choosing the adequate cannula modifying the distance from location of the target tissues. Second, most of the instruments used in the two systems are bended without joint, which prevents perfect triangulation and makes intracorporeal suturing more difficult. But, with the wristed needle driver in RSS surgery, we can do perform more meticulous suturing of ovarian tissues than is possible with the SPL surgery system even though the bending of the semirigid instruments prevents the surgeon from administering enough power handling the tissue. In addition, both the da Vinci Single-Site system and single-port laparoendoscopic system have limitation of instrumental movement ranges and gas evacuation power. Thus, further instrumental development is needed to maximize the effect of RSS surgery and single-site laparoendoscopic surgery.
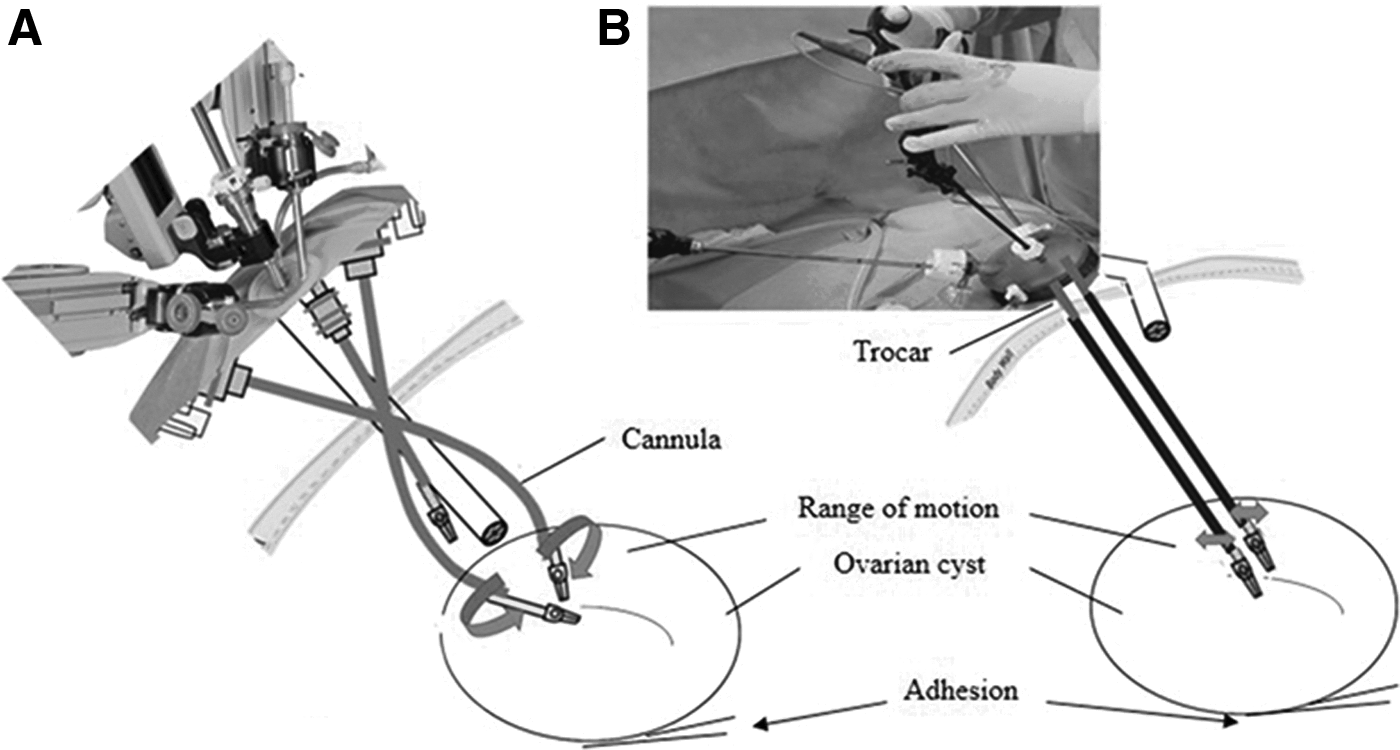
Comparison of RSSC
Even though there are still some limitations of the da Vinci Single-Site system, this study suggests that RSS surgery is feasible, safe, and effective for the treatment of advanced-stage endometriosis.
Footnotes
Acknowledgment
We thank Dr. Ami Rho for statistical analysis of data after collection.
Disclosure Statement
No competing financial interests exist.