
Abstract
Abstract
Background:
Since its introduction, the placement of percutaneous endoscopic gastrostomy (PEG) has been increasing in the Western countries. Nevertheless, it is not always possible to perform this operation. Laparoscopic-assisted endoscopic gastrostomy (LAPEG) is an effective alternative solution.
Materials and Methods:
Indication to PEG placement was established only for people who required a nutritional support of >4 weeks and without metastatic carcinoma. Sixteen patients underwent LAPEG after the failure of the original PEG operation. Two trocars of 5 mm and one of 12 mm were used, and a fourth trocar of 5 mm was placed when necessary to lift the liver. In four cases a gastrotomy was performed, in seven patients it was not necessary. When PEG was placed, the stomach was not fixed with stitches to the abdominal wall.
Results:
Sixteen patients were selected for LAPEG and were all successful; in one case it was necessary to replace the PEG, and the same procedure was performed again. Median age was 73 years. Placement of laparoscopic PEG was not associated with other surgical procedures. Nutritional feeding started the day after for patients with sutureless technique and 2 days after in patients with gastrotomy.
Conclusion:
LAPEG is a safe technique with a low complication rate. It should be considered a minimal alternative in all cases where the placement of PEG is not possible.
Background
T
LAPEG is a good option in those patients whom the traditional PEG placement has failed. The aim of this study is to review and disclose our results with LAPEG, in patients who failed traditional PEG placement.
Materials and Methods
Sixteen patients, from January 2010 to June 2016, who underwent LAPEG were reviewed. No patient was considered for LAPEG as first procedure. Classic PEG had failed in all sixteen patients. Patient demographics and history are reported in Table 1. All patients were operated by orotracheal intubation and 30° reverse Trendelenburg position. Antibiotic and thrombosis prophylaxes were carried out in all patients. Two techniques were considered. Trocar positioning and pneumoperitoneum were performed in the same way in both techniques (Fig. 1). Pneumoperitoneum was performed by Veress technique. Three trocars were positioned, two sized 5 mm and one sized 12 mm, and exceptionally, a fourth trocar sized 5 mm is placed to lift the liver (Figs. 1 and 2). At first, the abdominal cavity is inspected to allow safe PEG placement.
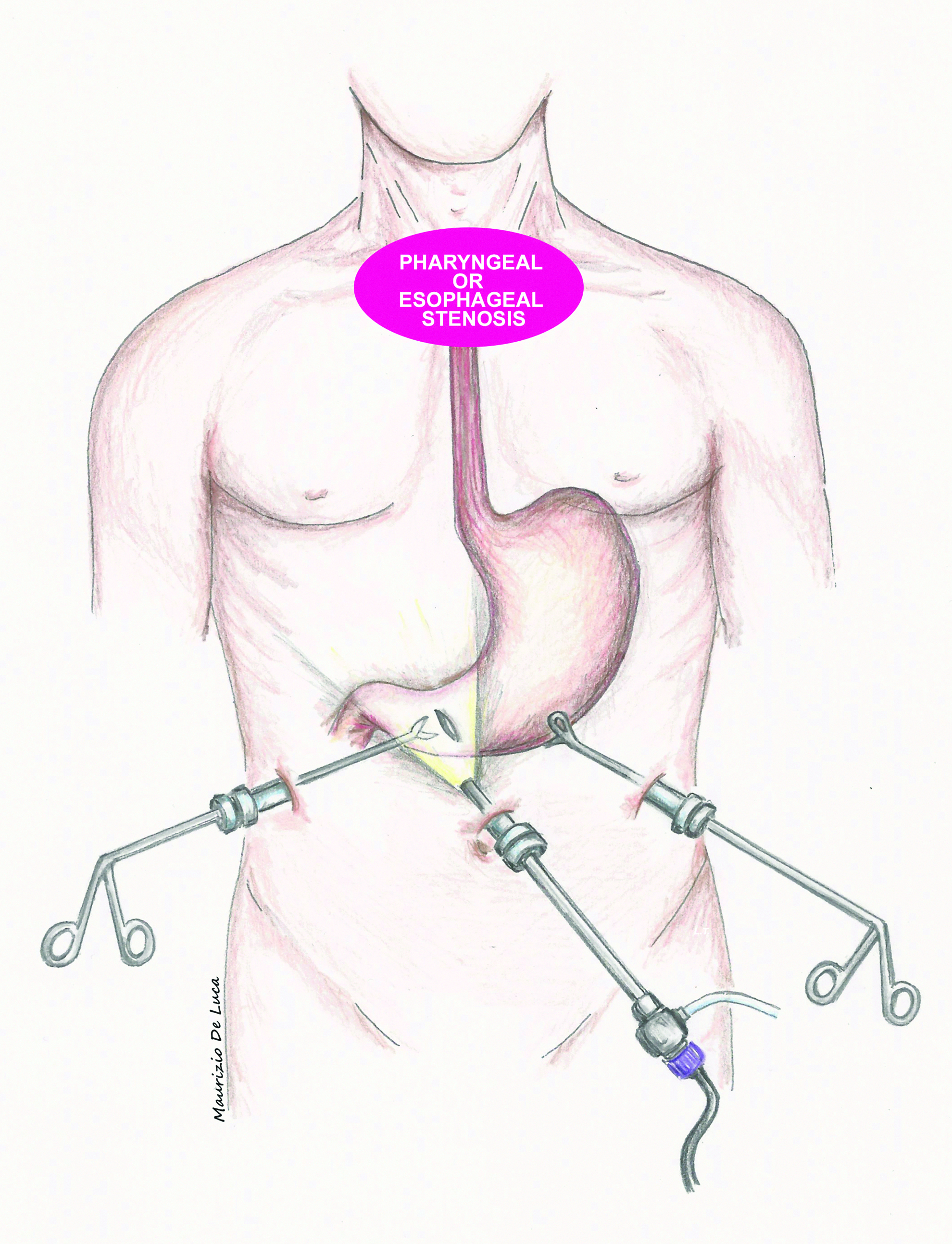
Trocars position.
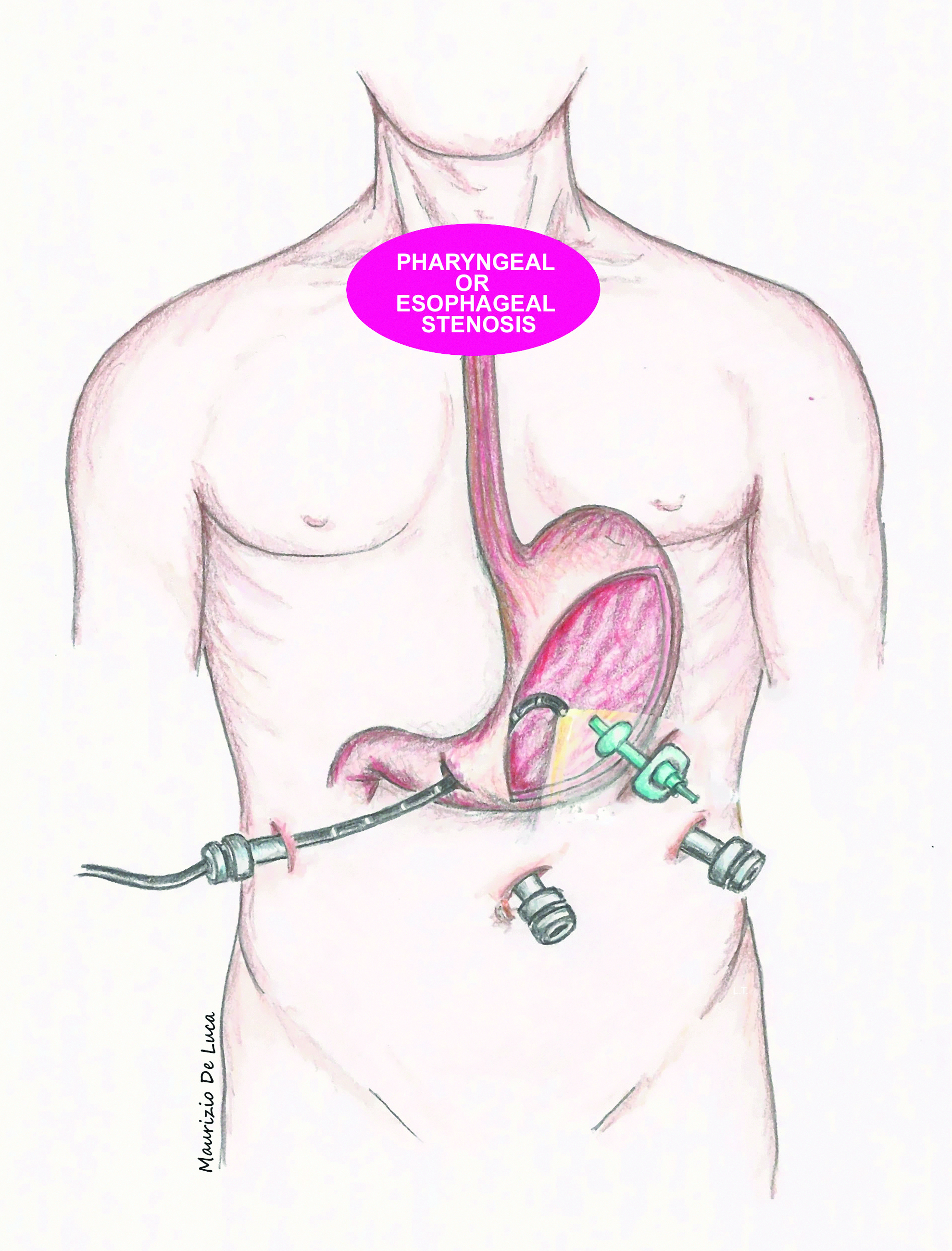
Second technique.
PEG, percutaneous endoscopic gastrostomy.
(1) Orogastric pathway, PEG, using the first technique, two stitches are positioned on the wall of the stomach for traction and transillumination. The site of gastrotomy is evaluated via gastroscopic and laparoscopic vision and supported by endoscopic insufflation of the stomach. PEG regularly positioned according to Ponsky technique. 1
(2) Trans-gastrotomy pathway, PEG, in case of pharyngeal, esophageal, or laryngeal carcinoma or esophageal stenosis, mainly for the cancer, gastroscopy is not performed by the normal orogastric pathway. In these cases, we approach the stomach by a second technique. After inspection of the abdominal cavity, 2 cm vertical gastrotomy is performed before the pylorus on the anterior wall of the stomach. The 12 mm trocar is positioned through the right hypocondrium and arranged close to the gastrotomy. Consequently, the endoscope enters in this 12 mm trocar and then through the gastrotomy in the stomach identifying the right place for PEG positioning (Fig. 2). Finally, PEG is normally positioned as in the Ponsky technique, with the difference that the endoscope reaches the stomach through a 12 mm trocar and not through the orogastric pathway. At the end of the procedure, the gastrotomy is closed by double running absorbable sutures. Other surgical procedures were not performed.
Results
Laparoendoscopic PEG was performed with success in all patients. In one case, it was necessary to replace the PEG with the same technique as it had been accidentally removed by the patient. In Table 1 are described the reasons for which the positioning of PEG was impossible. Mean age was 69.3 (60–78). Sixteen procedures were performed by laparoscopy and no conversion to open technique was necessary. Ten patients underwent surgery with the first technique and six with the second. In the first group, the most common reason for which the placement of PEG was not feasible was the impossibility to transilluminate the abdominal wall. Mean duration of LAPEG was 52 minutes with a range of 40–67 minutes. In these series, we did not observe any intraoperative complications. However, two postoperative complications were observed: respiratory distress and hemoperitoneum, treated with the positioning of a radiological drainage. Mortality did not occur. Long-term follow-up was not carried out. Follow-up ended when the patient was discharged from hospital. Nutrition via PEG started after 24 hours from the operation when gastrotomy was not necessary, and after 72 hours when it was. Mean discharge was 4 days. In all cases, no clinical complications were observed.
Discussion
In patients unable to intake food orally, PEG is the most suitable solution to long-term enteral nutritional support and, since its introduction, it has gained worldwide acceptance in nutritional support and management, and has resulted in being superior to jejunostomy. 10 Enteral feeding is usually preferred over parenteral nutrition because it does not compromise gut defense barrier and therefore decreases the risk of bacterial translocation. 4 At present, the placement of jejunostomy or PEJ (percutaneous endoscopic jejunostomy) is preferred in patients suffering Parkinson's disease because jejunostomy gives better small bowel absorption of levodopa/carbidopa. 11 Moreover, performing a laparoscopic jejunostomy is not considered simple, not even for an experienced surgeon, and the results are not always totally satisfactory; indeed, the rate of complications of PEJ was from 5% to 32% and mortality ranges from 0% to 11%. 12 PEG is a simple endoscopic procedure related to low mortality, and it does not require general anesthesia and the use of the operating room after the first report many authors published on safety of this procedure.13–15 PEG is not free of major and minor complications that can occur with a variable rate, from 0.5% to 22.5% of cases, and mortality attributable to upper endoscopy is 0.005%–0.01%.3,15–17
Alternatives of PEG are direct pharyngostomy or esophagostomy, but, at present, these techniques are rarely performed especially after the introduction of radiologic technique or LAPEG.18,19 Another endoscopic option to enteral feeding is endoscopic jejunal access, but, at present, placement of PEG is preferred because the first is more complicated. 3 LAPEG in children was described, at first, in 1995 by Lotan et al. using an approach similar to the Georgeson technique, but in 1993, Raaf et al. have described this technique for adult patients.20,21
The rate of PEG complications is not an indication to necessarily resort to the LAPEG technique, thanks also to its lower cost. 22 Beyond the costs of routine use of LAPEG, there are general contraindications for this technique such as the impossibility to use general anesthesia or make a pneumoperitoneum, or the presence of many adhesions restricting abdominal access.
Relative contraindication would be the need of a skill assistant competent to use the endoscope. At present, there are no studies that compare the results and rate of complications of PEG, LAPEG, or other invasive approaches in adult patients. Rate of complications appears similar to those reported for radiologic technique and lower than published for PEG in children. 23 In LAPEG operations, the stomach was not fixed to the abdominal wall as described by Takahashi, as he reported the clinical record of young people affected by cerebral palsy. 24 This condition is associated with high failure of adhesions to the abdominal wall. 24 Nevertheless, it was believed most suitable to fix the stomach to the abdominal wall in those patients with a big hiatal hernia. A surgeon with proper laparoscopic skills can perform LAPEG with less anesthesia compared with laparotomy, maintaining in any case the same advantages of PEG. In both groups, with or without sutures, the results were appreciable and the procedures were both diagnostic and therapeutic. The second technique via gastrotomy is an excellent alternative to classical jejunostomy. Therefore, the placement of LAPEG, with or without sutures, is a possible minimally invasive solution for all patients who require nutritional support for >4 weeks, yet are ineligible for the placement of a traditional PEG.
Authors' Contributions
A.S. was the lead author and conceived this study. M.D.L. contributed to data analysis and the writing of the article. All authors reviewed the article. All authors approved the final version of the article.
Footnotes
Disclosure Statement
No competing financial interests exist.