
Abstract
Abstract
Background:
Uniportal video-assisted thoracic surgery (VATS) is gaining popularity among thoracic surgeons, but the limited space in the thorax of children makes uniportal VATS difficult to perform. The purpose of this study was to evaluate procedural and outcome differences between a modified uniportal VATS (MU-VATS) and three-port VATS (TP-VATS) for peripheral lung nodule biopsy in pediatric cancer patients.
Materials and Methods:
This is an Institutional Review Board-approved retrospective analysis of all consecutive MU-VATS and TP-VATS peripheral lung nodule biopsies performed at a single institution between June 2014 and December 2016. Patients with diffuse lung disease who underwent a lung biopsy were excluded.
Results:
Over a 30-month period, 22 patients with a median age of 12 years (range, 7–21) underwent MU-VATS or TP-VATS for excisional biopsy of a peripheral lung nodule. MU-VATS lung biopsy was attempted in 11 patients and TP-VATS lung biopsy in the remaining 11. Both groups were comparable with regard to demographics, primary diagnosis, purpose of biopsy, and lung nodule location. MU-VATS demonstrated no difference when compared with TP-VATS lung biopsy in operative time (54 versus 62 min, P = .899), estimated blood loss (14 versus 15 mL, P = .587), pain score (2.8 versus 2.9, P = .717), and discharge day (1.3 versus 1.2 days, P = .572). No difference existed between groups with regard to conversion, need for intraoperative blood transfusion, and duration of chest tube. Complications including pneumothorax (n = 2) and subcutaneous emphysema (n = 1) were only seen in the TP-VATS group.
Conclusions:
MU-VATS can be safely utilized for biopsy of peripheral lung nodules in pediatric cancer patients without increasing procedural duration, hospitalization, pain scores, or need for intraoperative blood transfusion. Further studies need to evaluate the theoretical cosmetic advantage from a single surgical scar.
Introduction
U
Materials and Methods
After obtaining Institutional Review Board approval, hospital records of consecutive patients who underwent MU-VATS and TP-VATS peripheral lung nodule biopsies at our institution between June 2014 and December 2016 were retrospectively reviewed. Patients with diffuse lung disease who underwent a lung biopsy were excluded. Operative reports, daily progress notes, and clinic notes after discharge were reviewed for all patients. Demographics included gender, age at procedure, primary diagnosis, nodule location, and purpose of biopsy (diagnostic versus therapeutic). Perioperative data consisted of surgical technique (MU-VATS versus TP-VATS), instance of conversion, operative duration, estimated blood loss, need for intraoperative blood transfusion, chest tube removal day, postoperative length of stay, pathology, average pain score, and complications.
MU-VATS technique description
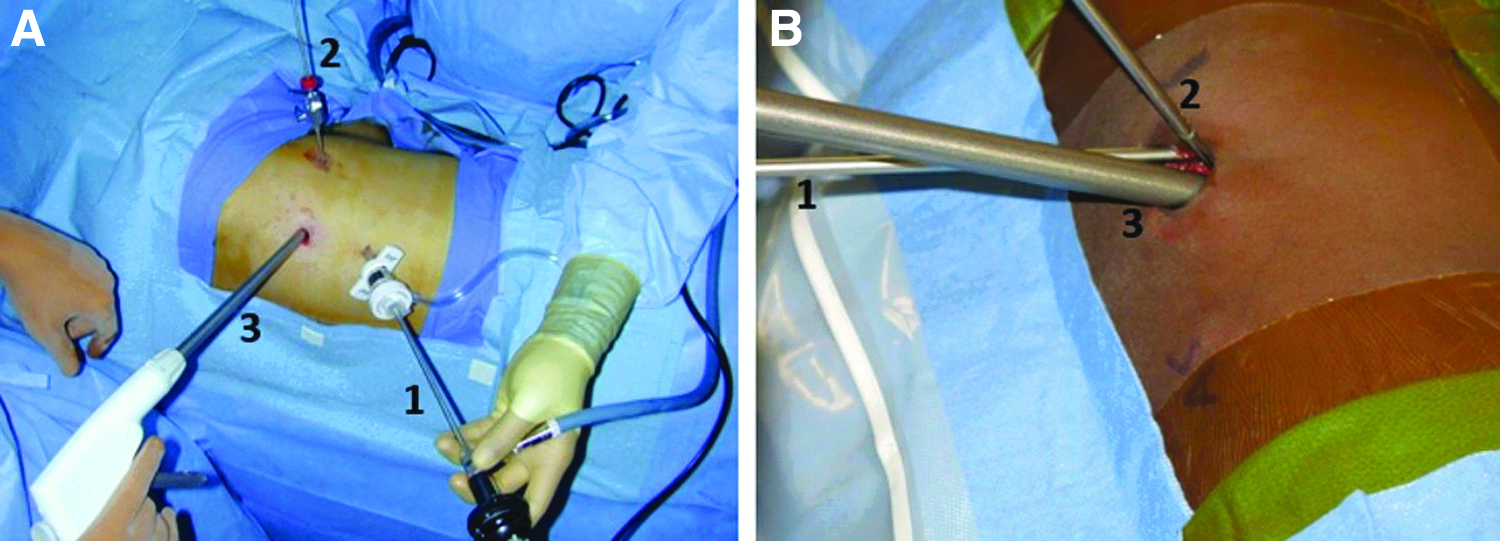
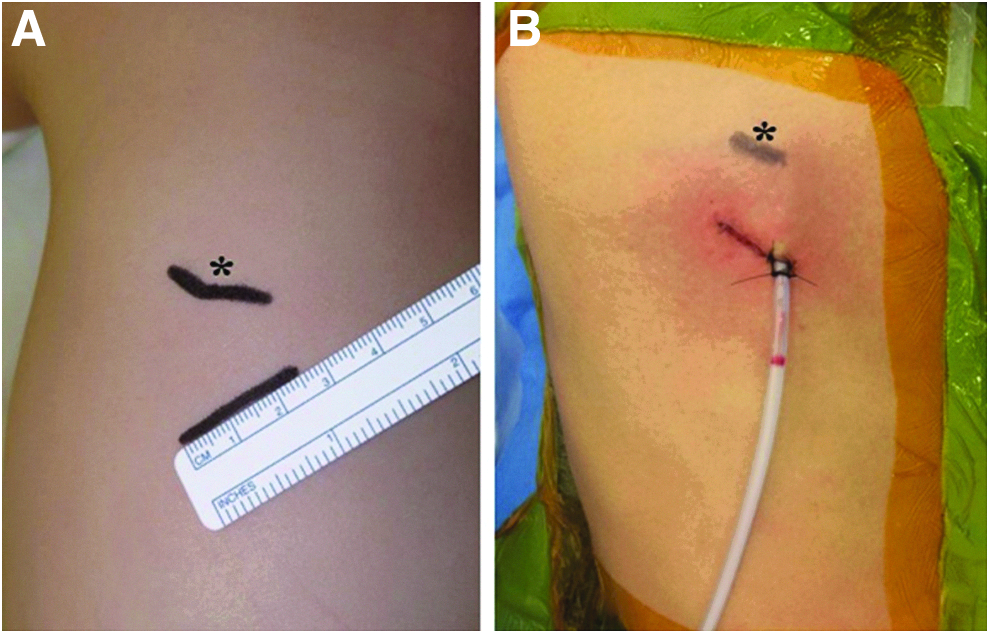
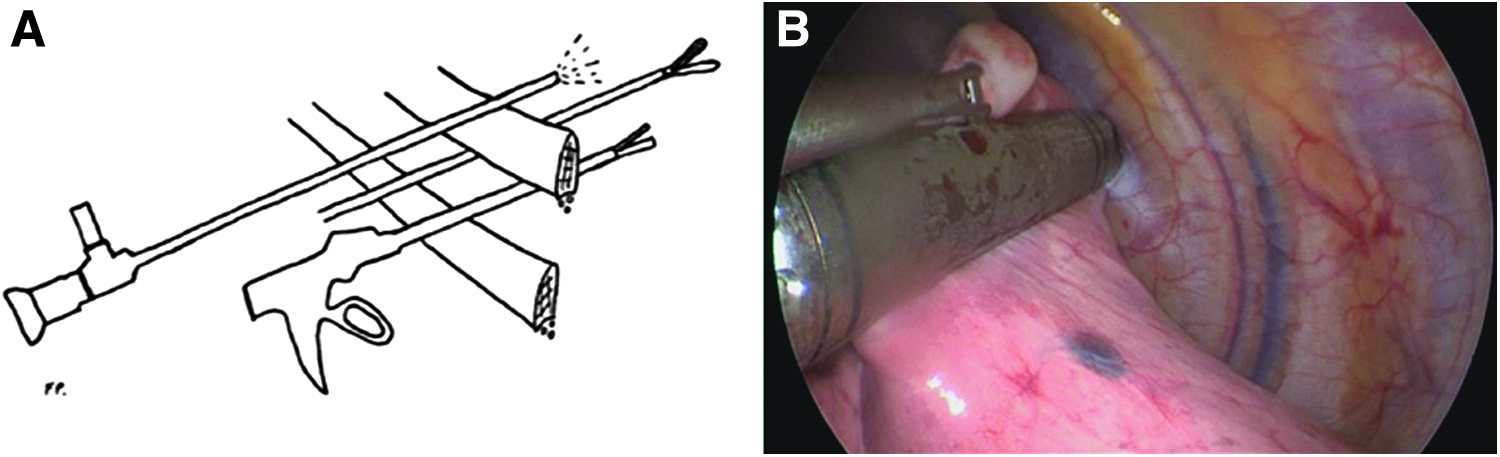
After implementation of one lung ventilation, the patient is placed in the lateral decubitus position. A 2.5 cm incision is made in an intercostal space to accommodate the thoracoscopic instruments; a 5 mm 30-degree endoscope is passed through the superior intercostal space relative to the working instruments. Because of the size of the uniportal approach incision, CO2 gas may leak through the incision and insufflation is not used. Single lung ventilation becomes critical for uniportal approach. The lung nodule is identified and grasped so that an endostapler can be used to perform wedge resection. A thoracostomy tube is then introduced through the superior muscular defect, where the endoscope has been, and is brought out of the incision. The chest wall is closed and the thoracostomy tube secured with a suture (Figs. 1–3).
Modified uniportal VATS approach
TP-VATS technique description
After implementation of one lung ventilation, the patient is placed in the lateral decubitus position. A 5 mm port is first placed inferior to the tip of the scapula and a 5 mm 30-degree endoscope is passed through this port (Fig. 1). CO2 gas insufflation is used, with a pressure of 5 mmHg. Another 5 mm port is placed close to the lung nodule target, and an endostapler for the wedge resection is directly inserted into the thorax without an additional trocar. A thoracostomy tube is then introduced through one of the port sites and secured with a suture.
Statistical analysis
Summary statistics for continuous variables and percentage for categorical variables were used.
To test the difference between MU-VATS and TP-VATS groups, a Wilcoxon rank-sum test was used for continuous variables and Pearson chi-square test was used for categorical variables.
Results
Twenty-two consecutive pediatric cancer patients underwent peripheral lung nodule biopsy by the same surgeon over a 30-month period (June 2014–December 2016). Median age at the time of operation was 12 years (range, 7–21). Of these cases, 11 were performed using MU-VATS technique and traditional TP-VATS procedure was used in the remaining 11 cases. Both groups were evaluated for differences in gender, age at procedure, nodule location, and primary diagnosis (Tables 1 and 2). Female-to-male distribution ratio was 1:1 for both groups, and no gender difference existed between MU-VATS and TP-VATS cases (P = .67). Age at procedure was similar for both groups and was not statistically significant (12.3 versus 12.6 years; P = .873).
CT, chest tube; ESFT, Ewing sarcoma family of tumors; HCC, hepatocellular carcinoma; HL, Hodgkin lymphoma; LLL, left lower lobe; LUL, left upper lobe; MU-VATS, modified uniportal video-assisted thoracic surgery; OS, osteosarcoma; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe; SCS, spindle cell sarcoma.
CT, chest tube; ESFT, Ewing sarcoma family of tumors; LLL, left lower lobe; LUL, left upper lobe; MU-VATS, modified uniportal video-assisted thoracic surgery; OS, osteosarcoma; RLL, right lower lobe; RML, right middle lobe; RMS, rhabdomyosarcoma; RUL, right upper lobe; SCS, spindle cell sarcoma; SS, synovial sarcoma.
The indication for lung nodule biopsy was to obtain a diagnosis in most of patients (n = 20, 91%). Lung nodule locations were similar between both groups, although six patients in the TP-VATS group required chest tube-guided needle localization for subpleural nodules. Osteosarcoma was the most common primary diagnosis (n = 12, 54.5%), followed by Ewing sarcoma family of tumors (n = 5, 22.7%).
Operative duration, estimated blood loss, and discharge by the first postoperative day were compared between MU-VATS and TP-VATS groups, with respective P values of .899, .587 and .572 (Table 3). No difference existed between groups with regard to instance of conversion, need for intraoperative blood transfusion, and timing of chest tube removal. Although median postoperative pain scores were lower in the MU-VATS group, this was not statistically significant (3.1 versus 4.2; P = .717). Pathology review showed malignancy in 13 (59%) patients and benign conditions in 9 (41%) patients.
F, female; M, male; MU-VATS, modified uniportal video-assisted thoracic surgery; TP-VATS, three-port video-assisted thoracic surgery.
Complications only occurred in the TP-VATS group and these included more than 10% residual pneumothorax (n = 2) and significant subcutaneous emphysema (n = 1). None of these complications required treatment. No postoperative unplanned admissions within 30 days of lung biopsy were recorded. No wound infections or dehiscences were observed in either group. Mean duration of follow-up was 10.5 months (range, 4–20) for MU-VATS and 14.7 months (range, 7–30) for TP-VATS. Five (22.7%) of 22 patients died of disease progression.
Discussion
VATS has become the standard of care for surgical conditions in the thorax over the past 2 decades.6,7 This approach has been traditionally performed by using one 3–5 cm utility thoracotomy with two additional working ports. 8 This three-port approach (TP-VATS) has been shown to be safe and feasible for complex thoracic procedures, including lobectomies, pneumonectomies, and resection of mediastinal masses. In an effort to be less invasive, a two-port VATS technique was developed and showed excellent results with regard to oncologic outcomes and complications. 9 To avoid intercostal neuralgia secondary to nerve compression because of a thick thoracoscope, a needlescopic VATS using a thin scope through a needle was described and resulted in less postoperative pain and better cosmesis. 10 One of the advantages of this approach is that it results in less interference between thoracoscope and working instruments. This is particularly important in patients with narrow intercostal spaces often encountered in the pediatric population. The main limitation of needlescopic VATS is the narrow field of view and the poor image brightness because of the scope size.
Over the past 5 years, the two-port approach has been refined to a single-site or uniportal VATS approach that utilizes a single skin incision and one intercostal space to accommodate the thoracoscope and the working instruments. 11 Uniportal VATS was first described for the treatment of palmar and axillary hyperhidrosis. 12 In 2004, Rocco et al. reported uniportal VATS pulmonary wedge resection in 15 patients. 13 In 2011, Gonzalez-Rivas et al. reported the first upper lobectomy performed by uniportal VATS. 14 Since then, this technique has gained popularity among thoracic surgeons worldwide and complex cases using this approach have been reported.15,16 One of the major advantages of uniportal VATS is the parallel instrumentation between the thoracoscope and the working instruments that mimics the maneuvers performed during open thoracotomy. Less incisional pain/intercostal neuralgia and improved cosmesis have also been associated with uniportal VATS. 17
Reduced port and single-site laparoscopy in children is becoming more common among pediatric surgeons for certain procedures, including appendectomy, cholecystectomy, and splenectomy. 18 The use of a single incision in the thorax is not as well established, and this may be secondary to (1) lower incidence of lung malignancies requiring surgical intervention relative to those affecting adults, (2) space limitation because of narrow intercostal spaces and small chests, and (3) inadequate single-lung ventilation techniques in neonates and young children. Pediatric uniportal VATS cases reported in the literature include sympathectomy, lung biopsy, and empyema debridement.2,19 Two major uniportal VATS procedures including middle lobectomy for the treatment of a pulmonary aspergilloma and an extralobar sequestration resection have been recently published.3,4
Competition and interference among thoracoscope and working instruments within the same intercostal space have been described as limitations of uniportal VATS. 11 To minimize this competition, we have described MU-VATS using a single skin incision but placing a long thoracoscope in the superior intercostal space relative to the working instruments. This allows increased instrument range of motion and less competition because the hands of the assistant surgeon are remote relative to those of the operating surgeon. The scope intercostal incision can be utilized as an exit site for the thoracostomy tube that permits a better closure of the larger intercostal incision. Our results suggest that MU-VATS can be safely utilized for biopsy of peripheral lung nodules in pediatric cancer patients without increasing procedural duration, hospitalization, pain scores, or need for intraoperative blood transfusion. From a patient perspective, the theoretical advantages associated with less pain anticipated with fewer sites of trauma to the chest wall and better cosmesis should be validated in further prospective studies. From the surgeon standpoint, the procedure allows the surgeon to use parallel instrumentation with less competition among the working instruments (Table 4).
MU-VATS, modified uniportal video-assisted thoracic surgery; TP-VATS, three-port video-assisted thoracic surgery; VATS, video-assisted thoracic surgery; +, advantage; −, disadvantage; ±, inconclusive.
Although MU-VATS has proven to be as useful as TP-VATS in our experience, there are some limitations to consider. Tissue trauma may be greater because multiple instruments are being passed through a limited space with a higher theoretical risk for wound complications. In addition, a selection bias might exist because MU-VATS has only been used for peripheral lung nodules that did not require image-guided localization. This technique needs to be validated for the resection of image-guided localized lesions.
In conclusion, we have added a modification to conventional uniportal VATS that may help facilitate operations in children by increasing degrees of freedom with regard to the range of motion. This technique is demonstrated to be as good as the conventional three-port VATS approach for biopsy of peripheral lung nodules in children with cancer. Potential advantages associated with less pain and better cosmesis should be validated in further prospective studies.
Authors' Contributions
Each author listed in the article has seen and approved the submission of this version of the article and takes full responsibility for the article.
Footnotes
Disclosure Statement
No competing financial interests exist.