
Abstract
Abstract
Purpose:
Approximately one quarter of children with complicated appendicitis develop postoperative abscess, leading to additional procedures and increased length of stay (LOS), but the optimal timing of postoperative imaging to detect abscess is unknown.
Methods:
The Pediatric Health Information System database was reviewed, and children who underwent laparoscopic appendectomy in 2013–2014 with postoperative LOS ≥5 days were included. Demographics, imaging, drainage procedures, LOS, and 30-day readmission were analyzed. Chi-squared analysis was performed.
Results:
A total of 21,985 patients underwent laparoscopic appendectomy and 3332 met inclusion criteria. A total of 1174 (35.2%) patients underwent postoperative imaging, among whom 38.4% underwent ultrasound and 75.0% underwent computed tomography scan. Timing of first imaging varied significantly between hospitals, ranging from 0% to 76% on postoperative day (POD) 5. Initial imaging was performed on POD 5, 6, and 7 in 19.7%, 31.3%, and 36.2%, respectively. Imaging on POD 5 compared with POD 7 was associated with shorter LOS (10.6 ± 5.7 versus 11.8 ± 4.4 days), but also lower rates of intervention (42.4% versus 50.8%), increased repeat imaging (10.8% versus 5.2%), and higher readmission rates (35.9% versus 28.2%) (P < .05).
Conclusion:
Timing of postoperative imaging for complicated appendicitis is variable across hospitals. While earlier imaging was associated with a decreased LOS, these children also had lower rates of subsequent intervention coupled with higher rates of repeat imaging and readmission. These findings suggest that delaying imaging until at least POD 6 may maximize the diagnostic yield of imaging while decreasing radiation exposure and readmission. Prospective investigation should be undertaken to guide the development of standardized clinical practice guidelines for the management of perforated appendicitis.
Introduction
A
Materials and Methods
Data for this study were obtained from the Pediatric Health Information System (PHIS), an administrative database that contains inpatient, emergency department, ambulatory surgery, and observation encounter-level data. The PHIS hospitals are 49 of the largest and most advanced children's hospitals in America, and constitute the most demanding standards of pediatric service in America. These hospitals are affiliated with the Children's Hospital Association (Overland Park, KS). Data quality and reliability are assured through a joint effort between the Children's Hospital Association and participating hospitals. Portions of the data submission and data quality processes for the PHIS database are managed by Truven Health Analytics (Ann Arbor, MI). For the purposes of external benchmarking, participating hospitals provide discharge/encounter data, including demographics, diagnoses, and procedures. Nearly all of these hospitals also submit resource utilization data (e.g., pharmaceuticals, imaging, and laboratory) into PHIS. Data are deidentified at the time of data submission, and data are subjected to a number of reliability and validity checks before being included in the database. For this study, data from 49 hospitals from January 1, 2013 through December 31, 2014 was included.
The study included all patients <18 years of age who underwent laparoscopic appendectomy for perforated appendicitis with postoperative LOS ≥5 days. Demographic data were captured, including age, sex, race, and ethnicity. First occurrence of postoperative imaging with either ultrasound (US) and/or CT on postoperative days (PODs) 5, 6, 7, and 8–10 was determined. The primary outcome measures were imaging rates, drainage procedures, reoperation, postoperative LOS, and 30-day readmission. Rates of intervention were calculated as the proportion of imaging that was followed by percutaneous drainage procedures or reoperation on days 5–10 of the postoperative period. Imaging was identified as US by Clinical Transaction of Care (CTC) codes 441141, 441142, 441241, 444741, 455041, 457040, 457041, 457042, or ICD-9 procedure codes 88.76, and as CT scan using CTC codes 441051 or ICD-9 procedure codes 88.01, 88.02, or 88.38. Drainage procedures were identified with ICD-9 procedure codes 54.91 and CTC codes 495200, 495000, 495022, 495041, 495042, 495051, 495052, or 495099, reoperation was identified with ICD-9 procedure codes 47.2, 54.0, 54.11, 54.12, 54.19, 54.21, 54.25, 54.4, 54.51, 54.59, 54.61, 54.62, 54.95, 86.04, 86.28, 86.59, or 95.59. Descriptive and Chi-squared analyses were performed using IBM SPSS Statistics for Windows, version 19.
Results
A total of 21,985 children underwent laparoscopic appendectomy and 3332 met inclusion criteria. The median age was 9 years (interquartile range 6–12) and the majority of patients were male (62.0%), white (62.4%), and non-Hispanic (53.8%).
Imaging utilization
A total of 1174 (35.2%) patients had postoperative imaging studies performed; among whom 38.4% underwent US and 75.0% underwent CT, with a subset having both types. First postoperative imaging was performed most frequently on POD 7. Among the 1174 patients who underwent imaging, 19.7%, 31.3%, 36.2%, and 12.7% were initially imaged on POD 5, 6, 7, and 8–10, respectively (Table 1). There was considerable hospital variability in the timing of imaging (Fig. 1). For example, the proportion of imaging that occurred on POD 5 ranged from 0% to 76% across hospitals. There were 78 patients who required repeat imaging. Notably, the rate of repeat imaging was higher in patients who were first imaged on POD 5, with 10.8% requiring repeat CT scan compared with 5.2% on POD 7 (P = .04).
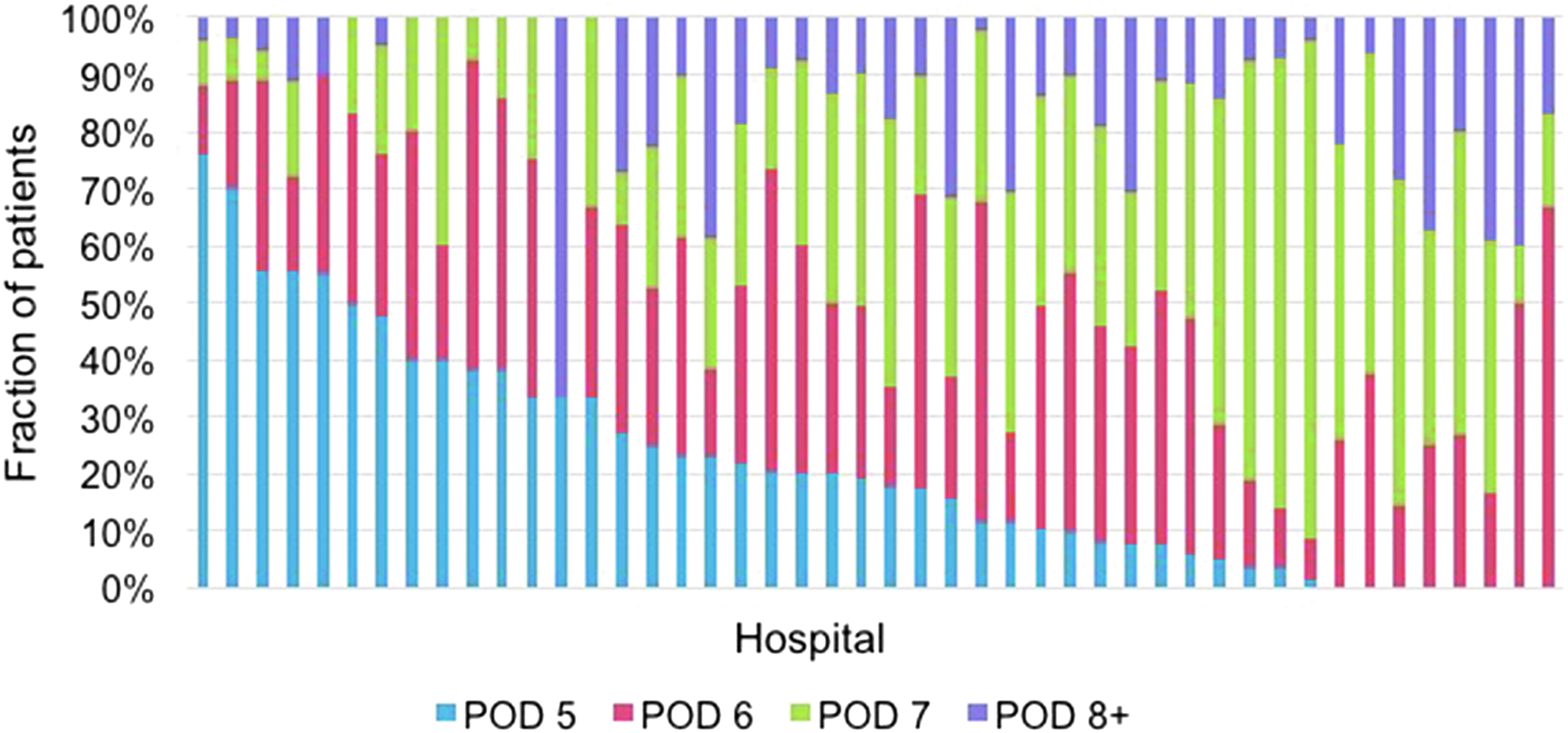
Hospital-level timing of first postoperative imaging study.
Some patients underwent both IR and OR intervention.
This includes imaging beyond day 10.
Same P < .001 if limited to just those patients who underwent imaging.
P = .152 if limited to just those patients who underwent imaging.
CT, computed tomography; IR, interventional radiology; LOS, length of stay; OR, operating room.
Postoperative intervention
Postoperative intervention was performed in 619 patients (18.6%) between POD 5 and 10, with 562 (16.9%) having percutaneous drain placement and 153 (4.6%) undergoing reoperation with a small number of patients having both interventions. The majority of interventions (67.9%) were performed between POD 6 and 7. Additionally, the proportion of patients who had an intervention following imaging was highest on POD 6 (59.5%) followed by POD 7 (50.8%) and POD 5 (43.4%). This difference was statistically significant (P < .001); suggesting the yield of imaging is greater after POD 5. Ninety-five percent of patients who underwent postoperative intervention had prior imaging.
LOS and readmissions
Postoperative LOS was significantly shorter in patients who did not undergo imaging compared with those who did (Table 1). Additionally, there was a significant increase in LOS for each day imaging was delayed. The average postoperative LOS was 10.6 ± 5.7 days for those imaged on POD 5 compared with 14.9 ± 7.0 on POD 8–10 (P < .001). While patients imaged earlier had a shorter LOS, readmission rates for these patients were significantly higher than those imaged later. Thirty-day readmission rates were 35.9%, 30.7%, 28.2%, and 26.7% for those first imaged on POD 5, 6, 7, and 8–10, respectively (P < .001). Of note, the readmission rate for patients who were observed without imaging entirely was 24.5%, comparable to those with the longest hospitalizations.
Discussion
There is significant practice variability in the timing of postoperative imaging following appendectomy for complicated appendicitis. While earlier imaging was associated with a decreased LOS, these children also had lower rates of subsequent intervention coupled with higher rates of repeat imaging and readmission. Additionally, children who did not require imaging had shorter LOS and a lower rate of readmission. Delaying postoperative imaging until at least POD 6 may maximize the diagnostic yield of the study while minimizing radiation exposure and risk of readmission.
The timing of postoperative imaging varies significantly both between and within institutions. The variation in practice between different institutions is highlighted by the finding herein that the proportion of imaging on POD 5 ranged from 0% to 76% at different hospitals. While acknowledging the influence of individual patient factors, practice variation may be partially attributable due to an underutilization of standardized clinical practice guidelines. A survey of American Pediatric Surgical Association members found that only 17% of pediatric surgeons use formal clinical practice guidelines for the management of perforated appendicitis. 13 Lack of standardization results in variation not only for the timing of imaging, but also in duration of postoperative antibiotic coverage, clinical parameters used for decision making, and discharge criteria. 14
The development and implementation of standardized guidelines requires the availability of high-quality data to guide on best practices. Data on the optimal timing of postoperative imaging to detect abscess is limited. The Surgical Infection Society broadly recommends that in “patients who have persistent or recurrent clinical evidence of intra-abdominal infection after 4–7 days of therapy, appropriate diagnostic investigation should be undertaken, [which] should include CT or US imaging.” 15 The challenge lies in determining where in that POD 4–7 range is optimal. In the early postoperative period, distinguishing benign free fluid from a walled-off collection or abscess is difficult. Historical data demonstrated poor sensitivity of CT scan for intra-abdominal abscess before POD 8. 16 However, modern thin-slice CTs may now potentially detect abscesses as early as POD 3, suggesting earlier imaging may be considered. 11 Expeditious identification of postoperative fluid collections is important to facilitate early treatment, as up to 75% of children with postoperative abscess will require intervention with drainage or reoperation. 6 A single-institutional retrospective review by Nielsen et al. found that early CT scanning (POD <7) resulted in higher rates of intervention and recurrent CT scans, but did not affect LOS. Additionally, those investigators found that 50% of those who avoided imaging within the first 7 days had resolution of symptoms and were discharged without intervention or CT. 12
The findings of the current study support delaying imaging until at least POD 6, and are in congruence with the conclusions of Nielsen et al. 12 Within the current study cohort, 21% of patients hospitalized for at least 5 days postoperatively underwent drainage or reoperation. The lower rate of intervention for patients who underwent imaging on POD 5, compared with later imaging is likely because in the earlier postoperative period some children will still exhibit symptoms of nausea, poor appetite, pain, or fever even in the absence of intra-abdominal abscess. However, the limitations of imaging to detect benign fluid from developing abscess in the earlier postoperative period may also contribute to this finding.
While unavailable for analysis in this administrative data set, there may be other clinical factors that can aid in identifying patients with a high pretest probability of intra-abdominal abscess that would benefit from early imaging versus those with a lower risk in whom imaging should be delayed or deferred. A number of clinical and laboratory predictors have been studied, including fever, pain, oral intake, white blood cell count (WBC), and C-reactive protein.14,17,18 The value of these markers in guiding management has been shown to be variable, but fever, elevated WBC, and time to full oral intake have been found to be positively associated with postoperative abscess development.9,17,19
It is important to acknowledge the limitations of this study in the interpretation of its findings. Administrative datasets such as PHIS are not designed for clinical decision making. Clinical markers such as those listed above were therefore unable to be included in the analysis and their effect on management decisions cannot be estimated. Additionally, there were no data on the indications for the imaging performed or for postoperative intervention. Future prospective studies should factor in these important elements that impact decision making. It is also important to note that some patients undergo intervention or reoperation for complications other than abscess, such as early postoperative bowel obstruction. However, relative to the rate of postoperative abscess, those other complications are very low following laparoscopic appendectomy.20,21
The results of this study suggest there is a role for clinical management pathways in the treatment of perforated appendicitis. When utilized, clinical pathways have been shown to decrease the rates of abscess drainage and readmissions. 20 Specifically, the implementation of a clinical pathway in one institution in which postoperative imaging was delayed until at least POD 7 resulted in lower rates of CT utilization, fewer recurrent CT scans, and decreased LOS without an increase in 30-day readmission. 12 This is consistent with findings from the current study that demonstrate imaging on POD 6 or 7 may maximize the diagnostic yield of the study while balancing longer LOS with decreased likelihood for repeat scans and readmission.
Conclusions
The timing of postoperative imaging for complicated appendicitis is variable. While associated with a shorter LOS, earlier imaging is also associated with lower diagnostic yield, more repeat imaging, and higher readmissions. For a proportion of patients, expectant management allowed for discharge without any additional imaging or procedures. This suggests that for the clinically stable patient, delaying imaging until later in the postoperative course may maximize the diagnostic yield of imaging while decreasing radiation exposure and risk of readmission. These findings are consistent with other retrospective studies, however, the nature of the data limit the ability to make a specific recommendation on the timing of imaging. These results highlight the potential value of further investigation to prospectively evaluate outcomes associated with the timing of postoperative imaging and the development of standardized clinical practice guidelines in the management of perforated appendicitis.
Footnotes
Disclosure Statement
No competing financial interests exist.