
Abstract
Abstract
Background:
Treatment of totally endophytic renal tumors is a technically demanding surgery. While few studies show promising perioperative and short-term outcomes of robot-assisted partial nephrectomy (RAPN), its long-term outcomes remain undetermined.
Materials and Methods:
A retrospective analysis of 89 patients with totally endophytic renal tumors undergoing either RAPN (n = 52) or open partial nephrectomy (OPN; n = 37) in a tertiary-care institution between 2005 and 2015 was performed. Primary endpoint was to describe our transperitoneal RAPN surgical technique, while secondary endpoint was to compare the 5-year chronic kidney disease (CKD)-free survival, cancer-specific survival (CSS), and metastasis-free survival (MFS) rates between RAPN and OPN.
Results:
The median follow-up was 59 and 53 months for RAPN and OPN, respectively. Apart from increased prevalence of high complex tumors among RAPN cases (RAPN, 38.5% versus OPN, 16.2%; P = .037), and lower median eGFR (RAPN, 86 versus OPN 96 mL/minute/1.73 m2; P = .032), the remaining demographic characteristics were similar between the groups. At latest follow-up, the rates of local recurrence (P = .577), distant metastasis (P = .854), and cancer death (P = .187), and CKD upstaging ≥stage 3 (P = .728) did not differ between groups. The 5-year CKD upstaging-free survival was 96.2% versus 94.6% (log-rank, P = .746), MFS was 95.8% versus 97.1% (P = .876), and CSS was 100% versus 93.8% (log-rank, P = .102) when stratified by RAPN and OPN, respectively.
Conclusion:
RAPN is a safe and feasible option for treatment of totally endophytic renal tumors. Despite the increased prevalence of high tumor complexity and lower baseline renal function in the RAPN group, it achieved equivalent long-term oncologic control and functional outcome compared to OPN.
Introduction
According to the guidelines of renal cell carcinoma (RCC), partial nephrectomy (PN) has been recommended for the treatment of T1 renal tumors whenever technically feasible. 1 PN can be performed using open, laparoscopic, or robotic approach depending on the surgeon's experience. Recently, robot-assisted PN (RAPN) has been found to be an efficient alternative to open PN (OPN) with the advantage of lower perioperative complication rates. 2 With the wide application of robotic technology in treatment of RCC, the indications of RAPN have been extended to include treatment of larger 3 and high complex renal tumors.4,5 Recently, the feasibility and safety of RAPN for treatment of totally endophytic renal tumors have been studied.6–9 However, its long-term outcomes remain to be determined.
To the best of our knowledge, there is no study evaluating the long-term oncological and functional outcomes of RAPN for totally endophytic renal tumors. In this study, we aimed to describe the long-term outcomes of our RAPN techniques, as well as to compare outcomes between RAPN and OPN cohorts.
Materials and Methods
This retrospective comparative study was approved by our ethics committee institutional review board (IBR number: 2014-0090-001). All patients were fully informed with regard to the surgical approach (RAPN or OPN) and its possible complications. We retrospectively reviewed the records of 850 consecutive patients undergoing PN in our prospectively maintained database between 2005 and 2015. We extracted patients with totally endophytic renal tumors who received either RAPN (n = 52) or OPN (n = 37). Patients with incomplete data, <12 months of follow-up, solitary kidney, and bilateral renal masses were excluded. The R.E.N.A.L. nephrometry scoring system was used to score the complexity of the tumors 10 (Fig. 1).
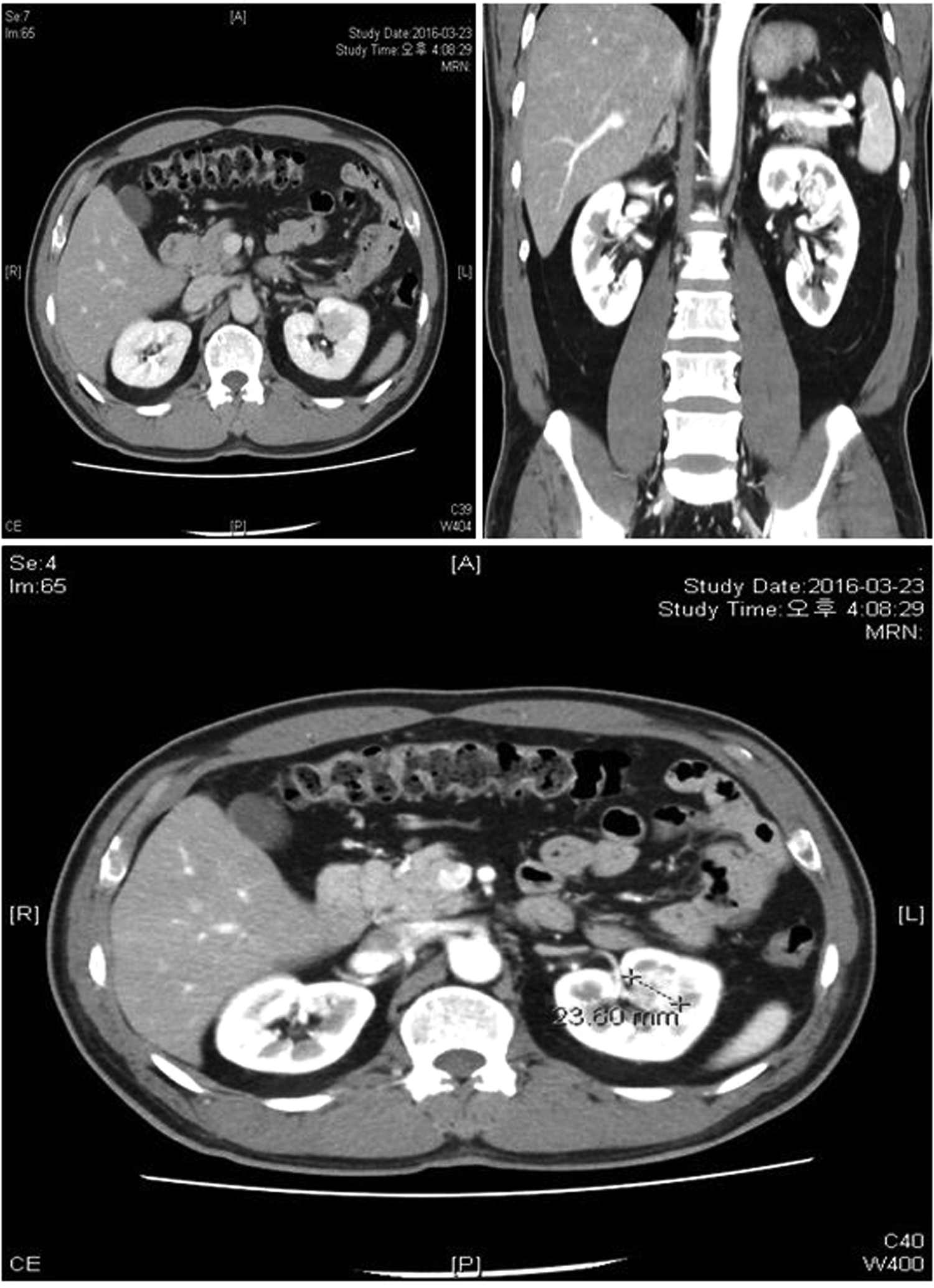
A 2.4 cm totally endophytic enhanced renal mass in the left kidney. The mass is of intermediate complexity with R.E.N.A.L. score = 9a “R = 1 point, E = 3 points, N = 3 points, and L = points.”
Patient's demographic characteristics and perioperative data were analyzed, including age, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, preoperative estimated glomerular filtration rate (eGFR), preoperative chronic kidney disease (CKD) stage, R.E.N.A.L. score, tumor size, clinical stage, operative time (OT), warm ischemia time (WIT), and estimated blood loss (EBL). Postoperative outcomes included complications (based on Clavien-Dindo Classification), length of hospital stay (LOHS), and postoperative CKD stage. Surgical specimens were processed in standard manner and pathological data were registered (pathological tumor size, TNM stage, Fuhrman grade, positive surgical margin (PSM), and histological subtypes).
The eGFR was calculated using the Modification of Diet in Renal Disease (MDRD) formula. The CKD stage was classified using the National Kidney foundation definition and CKD upstaging was defined as new-onset CKD ≥3 for at least 2 subsequent measurements. 11 Renal function, that is, “eGFR measurement,” was assessed at regular intervals: 1 month, 3 months, 6 months, 1 year, and then yearly. Events of local recurrence, distant metastasis, disease progression, death due to cancer, and all causes of death were reviewed. Oncological outcomes and patients with PSM are followed up according to the standardized clinical protocol at our institution. Generally, follow-up includes physical examination, chest radiographs, and kidney imaging (CT scan and/or MRI) every 6–12 months during the first 5 years and annually thereafter. Longevity of follow-up was determined from the date of operation until the last clinical follow-up.
Outcome measurements
The primary endpoint was to describe our step-by-step RAPN technique for the treatment of totally endophytic tumors. The secondary endpoint was to evaluate the long-term functional and oncological outcomes, as well as, to compare them to similar tumors undergoing OPN.
Surgical technique
OPN was performed using a previously described technique by our group. 12 RAPN surgical steps are discussed below. Choosing RAPN or OPN was based on surgeon and patient preference. All surgeries were carried out by three high-volume surgeons, OPN by (B.H.C. and Y.D.C.) and RAPN by (K.H.R.).
RAPN surgical technique
All RAPN procedures were performed with da Vinci Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA) through the transperitoneal approach.
Anesthesia
General anesthesia
Patient position
The patient is placed in the lateral flank position with no table flexion (Fig. 2), secured to the table with adhesive tape, and gel support with padding is applied to all pressure points.

The patient is placed in the lateral flank position with no table flexion, secured to the table with adhesive tape, and gel support with padding is applied to all pressure points.
Port placement
We establish the pneumoperitoneum with a Veress needle. Port sites are not uniform; instead they are based on the da Vinci model (Si or Xi) (Fig. 3). For da Vinci Si, we insert a midline supraumbilical 12-mm camera port, two 8-mm robotic ports in the midclavicular line at an 8–9 cm distance from the camera port, and an 8-mm robotic port at 10–12 cm from the lower robotic port directed toward the anterior superior ischial spine. A 12-mm assistant port is placed in the midline below the umbilicus and at an 8-cm distance from the lower robotic port. For right-sided renal tumors, we insert an additional 5-mm port for liver retraction (Fig. 3A). In the da Vinci Xi model, we used our modified port placement technique (Fig. 3C), instead of the universal linear port placement (Fig. 3B). 13 The modified port placement of da Vinci Xi is ideally for patients who tend to have low BMI and/or short height. 13
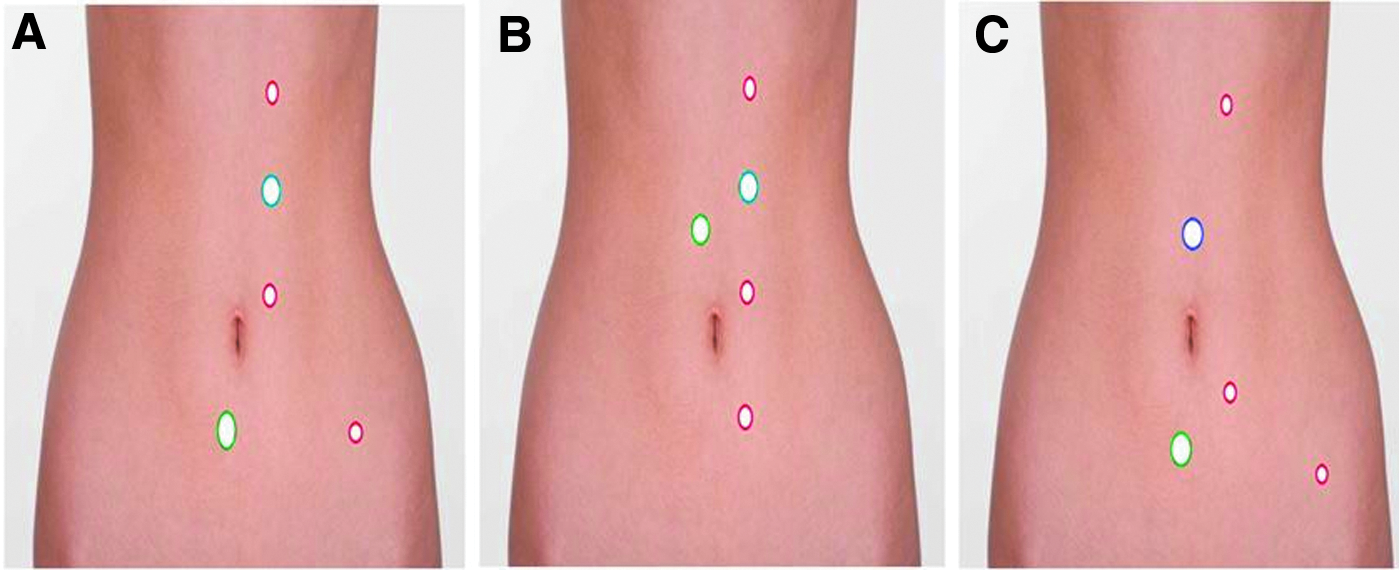
Showing the port placement for da Vinci Si model
Robotic instruments
We use the following robotic instruments: a laparoscopic 30-degree downward lens, ProGrasp® forceps, Hot Shear™ Monopolar curved scissors, two large needle drivers, and fenestrated bipolar forceps (Intuitive Surgical, Inc., Sunnyvale, CA).
Surgical steps
Watch the Supplementary Video S1 (Supplementary Data are available online at www.liebertpub.com/lap):
The colon is reflected medially away from the Gerota's fascia to expose the kidney. The gonadal vein and ureter are identified, and the gonadal vein (left side) or the ureter (right side) is traced up to the renal hilum. The renal pedicle is dissected and exposed, to allow easy access in case of uncontrollable bleeding. The kidney is mobilized and we incise the Gerota's fascia overlying the tumor. The renal tumor is defatted from the surrounding perinephric fat, while preserving the peritumoral fat for oncological safety. The tumor depth and extension are determined by using intraoperative ultrasonography (US) to demarcate peritumoral margins. Intravenous injection of mannitol (12.5 g) is carried out by the anesthesiologist. The renal artery is clamped using two, short straight bulldog clamps. Before tumor excision, we introduce a 3/0 Vicrylon SH needle with a length of 20 cm, laparoscopic specimen bag, and Surgicel® (Ethicon US, LLC.). We excise the tumor circumferentially by sharp cutting “cold-scissor excision,” while the fenestrated bipolar forceps aid in blunt dissection of the tumor off renal parenchyma. The ProGrasp forceps is used to elevate the tumor with its peritumoral fat upward to facilitate the dissection. The bedside assistant uses suction to maintain a clear vision, apply counter traction as necessary during tumor excision, and control any bleeding points with direct pressure. Mobilization of the tumor is continued circumferentially until complete excision of the tumor is achieved. Bleeding from the resection site is usually controlled by the following: monopolar scissor cautery, direct pressure by the assistant suction tip, or increased pneumoperitoneum pressure (20 mm Hg). The specimen is then placed in a previously inserted specimen bag above the liver or spleen for later retrieval. We change the fenestrated bipolar forceps and scissors are replaced with two large needle drivers. The inner layer closure is performed using a running 3–0 Vicryl SH on needle (sliding clip renorrhaphy technique). We use the Lapra-ty and 5-mm Weck clips (Ethicon Endosurgery, Cincinnati, OH) to secure the running suture. For the outer layer closure, we use a running 2–0 Vicryl SH on needle. Before closure of the Gerota's fascia, hemostatic agents Floseal (Hemostatic Matrix, Baxter), Surgicel, or Greenplast (Fibrin Glue) are applied over the renorrhaphy site. A 5-mm tubal drain is routinely inserted in the paracolic gutter, and the specimen is removed through the 12-mm umbilical port with extension of the incision if necessary.
Statistical analysis
We used an independent t-test or Mann-Whitney U-Test for comparing continuous variables between groups, specified as mean and standard deviation or median and interquartile range, while Chi-square test or Fisher's exact test was used for comparing categorical variables, specified as frequency (%). Kaplan-Meier analysis was used to compare the long-term CKD upstaging-free survival, cancer-specific survival (CSS), metastasis-free survival (MFS), and overall survival (OS) rates between RAPN and OPN. Statistical analyses were performed using IBM SPSS 23 statistical package (SPSS, Inc., Chicago, IL).
Results
A total of 89 cases (52 RAPN, 37 OPN) with totally endophytic tumors were performed. Table 1 summarizes the baseline clinical and demographic characteristics of both groups. The median follow-up was 59 and 53 months for RAPN and OPN, respectively. There was no statistically significant difference between both groups regarding age, BMI, sex, ASA score, tumor size, clinical stage, and R.E.N.A.L. score (P > .05). However, patients in the RAPN cohort had higher incidence of complex tumors compared to those in the OPN cohort (38.5% versus 16.2%; P = .037), and lower median eGFR (86 versus 96 mL/minute/1.73 m 2 ; P = .032).
Baseline Clinical and Demographic Characteristics
P-values shown in bold < 0.05 are considered significant.
ASA, American Society of Anesthesiologists; BMI, body mass index; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; IQR, interquartile range; OPN, open partial nephrectomy; RAPN, robot-assisted partial nephrectomy; RCC, renal cell carcinoma; SD, standard deviation.
Regarding the pathology findings, 44 (84.6%) patients in the RAPN group and 34 (91.9%) patients in the OPN group presented malignant pathologies (P = .350). There was no statistically significant difference regarding the prevalence of histopathological RCC subtypes in both groups (P = .507). Similarly, high Fuhrman grade 3 + 4 was 26.9% versus 24.3% in RAPN and OPN cohorts, respectively (P = .351). Eight patients (8.9%) showed PSM in our cohort with no significant difference between both surgical approaches (P = .806). Among those patients, seven had moderate-to-high complex RENAL score. Regarding pathological features, six patients had clear cell RCC, two had papillary RCC, two had chromophobe RCC, and one had multilocular cystic RCC. One patient with PSM developed local recurrence at the tumor bed.
Table 2 summarizes the perioperative data, functional and oncological outcomes. Patients in the RAPN group had shorter WIT (24 minutes versus 27 minutes; P = .067) than those in the OPN group. In the RAPN group, tumors were resected by zero ischemia in four patients (7.7%), while in OPN, eight patients (21.6%) had cold ischemia (P = .001).
Perioperative and Postoperative Outcomes:
P-values shown in bold < 0.05 are considered significant.
Clinical disease progression is defined as any local recurrence and/or distant metastasis event.
eGFR(mL/minute/1.73 m 2 ), eGFR% preservation, eGFR% change, CKD, and CKD upgrading at latest follow-up, “a median time of 59 and 53 months.”
Survival analysis was estimated for patients with proven malignant pathology only.
CKDFS, chronic kidney disease upstaging-free survival; CSS, cancer-specific free survival; EBL, estimated blood loss; IQR, interquartile range; MFS, metastasis-free survival; OPN, open partial nephrectomy; OS, overall survival; OT, total operative time; PFS, progression-free survival; PSM, positive surgical margin; RAPN, robot-assisted partial nephrectomy; RN, radical nephrectomy; SD, standard deviation; WIT, warm ischemia time.
Of note, EBL volume (P = .435), length of OT (P = .744), and LOHS (P = .154) were similar between groups. In terms of intraoperative complications, three patients (5.9%) in the robotic arm were converted to robotic-assisted radical nephrectomy (RN) due to positive frozen biopsy, renal vein injury, and persistent severe bleeding after unclamping. On the other hand, one patient (2.3%) was converted to open RN due to uncontrolled bleeding in the OPN group. The rate of intraoperative blood transfusion did not differ between groups (P = .372). Postoperative complications were observed in 12 and 10 patients in the RAPN and OPN groups, respectively (23.1% and 27%, P = .390). The majority of complications (87.5%) were grades 1 and 2.
At the latest follow-up, patients in the RAPN cohort had lower median eGFR (78 versus 89 mL/minute/1.73 m 2 , P = .032) and higher CKD stage 2 (67.3% versus 35.1%, P = .011) than the OPN cohort; nevertheless, there was no significant difference in the overall CKD upgrading rate (P = .891), median eGFR%-change at 1 year (P = .821), median eGFR% change at last follow-up (P = .420), median%-eGFR preservation rate (P = .119), as well as, CKD upstaging ≥stage 3 (P = .728). The 5-year CKD upstaging-free survival rates were 96.2% versus 94.6% (log rank, P = .746) when stratified by RAPN and OPN, respectively.
From an oncological point of view (Fig. 4), in the RAPN cohort, one patient (2.3%) showed local recurrence at resection bed, and one patient (2.3%) showed distant metastasis in the lung. There were no cases of cancer death and the CSS rate was 100%. The rates of local recurrence (P = .577), distant metastasis (P = .854), and cancer death (P = .187) did not differ between groups.

Discussion
PN is considered the treatment of choice for small renal masses. 1 It aims to achieve oncological safety, minimize ischemia, avoid complications, and preserve renal function as much as possible. Endophytic renal tumors are defined as tumors with no exophytic component and are scored with an endophytic/exophytic “E” domain nephrometry score of 3. 10 The treatment of such tumors with PN is considered surgically challenging. Inaccuracy in identification of the tumor extension, increased risk of vascular entry, and the need for reconstruction of a large parenchymal and pelvicalyceal defect could have a negative influence on the perioperative findings, oncologic control, and renal function preservation.
The use of intraoperative US is mandatory to identify the location, margin and depth of the endophytic renal tumor before surgery. RCC can be hypoechoic, isoechoic, or hyperechoic relative to the remainder of the renal parenchyma. Isoechoic renal masses can be difficult to identify. However, the high spatial resolution of intraoperative US provides high-quality and real-time imaging. In addition, the direct contact of the transducer on the kidney capsular surface helps in reducing artifacts and visualization difficulties, detecting additional small renal masses, and characterizing the anatomic relationship of the renal mass to adjacent structures such as pelvicalyceal system, renal sinus, and major blood vessels to determine the best surgical resection site.14,15 Preoperative CT scan and/or MRI are essential in determining the primary site of isoechoic endophytic tumors, which are further confirmed using intraoperarive US to identify either a clear-cut margin between the renal sinus and the tumor or a distortion of the hyperechoic central sinus fat by the tumor.
Recently, Patel et al. showed that PN utilization in renal surgery is on the rise, which is associated with the rise of robotic application. 16 Indeed, RAPN has allowed for the meticulous dissection of endophytic tumors with intraoperative US guidance, renorrhaphy completion within a short period of time, and improved perioperative outcomes. Recent studies examining perioperative and short-term outcomes concluded that RAPN is a safe and feasible option for endophtyic tumors.6–9 However, none of them assessed the long-term outcomes.
Our aim in this study was to describe the long-term outcomes of our RAPN techniques for endophytic tumors, as well as, to compare it to an OPN cohort in a retrospective study. Although the ideal approach for comparing competing treatment modalities is a randomized controlled trial, it is very difficult to carry out this type of study due to ethical considerations. A feasible alternative is performing a propensity score-matched analysis to minimize the selection bias by adjusting for the preoperative confounding variables. However, we could not do matching due to the small number of patients in our study. Although we included patients with the same lesions, that is, totally endophytic tumors, patients in the RAPN group had more prevalence of high complex renal tumors and lower preoperative eGFR than those patients in the OPN group. This represents a source of selection bias in this study. Actually, high complex tumors and those with lower eGFR might be ideally treated by open approach with the advantages of using cold ischemia. However, in high-volume robotic centers and expert robotic surgeons, the first preference is to treat complex renal tumors and patients with borderline renal function by using the robotic technology as an alternative to open surgery. Similarly, complex and endophytic tumors could be treated within safe WIT by using the robotic technology, which overcomes the difficulties of laparoscopic PN. As shown in Table 3, the mean WIT ranged from 17 to 24 minutes following RAPN.7–9 More recently, several studies compare RAPN and OPN in the treatment of high complex tumors 5 and patients with CKD. 17 Wang et al., compared the surgical, functional, and oncological outcomes of patients undergoing RAPN (n = 190) or OPN (n = 190) for moderate or high complex renal tumors (R.E.N.A.L. score ≥7). They found that RAPN provides acceptable and comparable results in terms of functional and oncological outcomes compared to OPN. Moreover, RAPN is a less invasive approach with the benefit of shorter LOHS, less EBL, and lower rate of postoperative complications. 5 Similarly, Takagi et al., compared the surgical outcomes between RAPN (n = 40) and OPN (n = 40) in patients with CKD. They concluded that both surgical approaches provide similar outcomes in terms of functional preservation and perioperative complications among patients with CKD. However, a lower EBL and shorter LOHS were obtained with RAPN. 17
literature Data of Endophytic Renal Tumors Outcomes Following Partial Nephrectomy Surgery
CKD, chronic kidney disease; CSS, cancer-specific free survival; EBL, estimated blood loss; eGFR, estimated glomerular filtration rate; MFS, metastasis-free survival; NAV, not available; OPN, open partial nephrectomy; OS, overall survival; OT, total operative time; PSM, positive surgical margin; RAPN, robot-assisted partial nephrectomy; WIT, warm ischemia time.
From the pathological standpoint, our PSM rates were 9.6% and 8.1% in the RAPN and OPN groups, respectively. Of note, the PSM rates in our study are slightly higher than previous RAPN (6.5%) 18 and OPN (5.5%) reports. 19 We could attribute higher PSM rates in this study to the nature of lesions included, that is, endophytic and the majority with a high RENAL score. Of note, the rate of PSM in endophytic tumors is much lower than in patients with nonendophytic tumors. Our previous study showed that PSM rate was 2.1% and 4% in exophytic and mesophytic tumors, respectively. 8 Interestingly, several studies showed that, in most cases, the presence of PSM on the final pathology does not mean that cancer remains in the renal remnant, 20 and thus may not be associated with disease recurrence.19,21 Recently, Mouracade and colleagues studied the patterns and predictors of recurrence in 830 patients with clinically localized RCC managed by PN. The overall PSM rate was 7.1%. They found that higher pathological stage and grade were predictors of metastasis, while higher RENAL score was the only predictor of local recurrence. 22 There are several technical points that will help to minimize the risk of PSM for totally endophytic tumors: (1) using intraoperative US; (2) using cold-scissor cutting to excise the tumor without tissue charring and provide an unaltered specimen for pathological assessment; and (3) using adequate hilar clamping to achieve a bloodless operative field and decrease kidney turgor for excellent tumor visualization and precise resection.
Although intraoperative frozen section analysis is not definitive and its value in guiding intraoperative management remains to be defined, 23 we routinely take a frozen specimen from the tumor bed. In our study, one patient showed positive frozen biopsy and thus was converted to RN. Some endophytic tumors may abut or invade into the renal sinus, in which case, the frozen biopsy is taken as superficially as possible.
Regarding the perioperative outcomes, the median WIT in the RAPN group was 24 minutes and the postoperative complications rate was 23.1%. There was no significant difference compared to the OPN group. Our results are in agreement with a recent report by Kara et al. who compared RAPN (n = 87) and OPN (n = 56) for treatment of totally endophytic renal tumors. 9 The median WIT was 24 minutes and the postoperative complications rate was 20.7% in the RAPN arm, with no significant difference compared to the OPN arm. 9 The median OT length in our study was 170 minutes and median LOHS was 4 days; these results are in line with a study by Autorino et al. 6 They evaluated the outcomes of 65 endophytic tumors following RAPN with a mean OT and LOHS of 175.8 minutes and 3.4 days, respectively. 6 Interestingly, the mean EBL in our study was 300 mL (100–550), which was higher than 100 mL (100–150) EBL found by Curtiss et al. 7 We may attribute this to the relatively larger tumor size in our cohort (mean 2.8 cm), while median tumor size was 2.3 cm and pT1a stage was present in 75% of cases in the Curtiss et al.'s study. 7 Moreover, 4 patients (7.7%) of our cohort underwent off-clamp and 11 patients (21.2%) underwent selective-clamp RAPN. Notably, off-clamp RAPN is a surgically demanding approach associated with more blood loss and requires a very experienced robotic team. Thus, endophytic tumors treated with off-clamp surgery in our cohort were chosen very carefully, that is, small (<3 cm), cortical lesions, and were of low-to-moderate tumor complexity. Actually, the maximum functional benefit appears in the setting of single kidney, 24 while in patients with two functioning renal units, its use marginally increased blood loss without providing a renal function benefit. 25 Our recent research (unpublished data) comparing matched groups after off-clamp and on-clamp RAPN showed no significant difference at the long-term functional outcomes. Also, we do not recommend its application for high complex tumors (Preoperative Aspects and Dimensions Used for an Anatomical [PADUA] ≥9) and tumors larger than 3.2 cm because of increased risk of bleeding and transfusion. 26 The conversion rate was 5.9% and 2.7% in RAPN and OPN, respectively. Despite increased tendency of RN in our RAPN cohort, it seems that conversion rate is comparable between both surgical approaches as reported in a recent systematic review and meta-analysis by Wu et al. 2 In addition, the rate of conversion in our study is in agreement with more recent studies. In a prospective multi-institutional study, including 501 patients undergoing RAPN from 2014 to 2017, 5% converted to RN. 27 In a larger cohort, 1,857 patients underwent successful PN between 1990 and 2016; the rate of conversion to RN was 5% (n = 90) patients. Of note, laparoscopic PN (OR = 7.34; P < .001) was the surgical approach that associated with conversion to RN compared to OPN and RAPN. 28
For the assessment of renal function, we included patients with a minimum follow-up of 12 months, which is sufficient for proper functional recovery following PN.16,29 At the latest follow-up, the median eGFR was lower and the prevalence of CKD stage 2 was higher in patients undergoing RAPN compared to OPN. However, this result was expected and can be attributed to the lower baseline eGFR in the RAPN arm. Despite the lower preoperative eGFR and the higher prevalence of complex tumors in RAPN patients, the % eGFR preservation rate, the overall CKD upgrading rate, CKD upstaging ≥stage 3, and the 5-year CKD upstaging-free survival rate did not differ between the RAPN and OPN groups. These results emphasize the promising role of robotic surgery in the future treatment of endophytic renal tumors. In the study comparing the functional outcomes of RAPN and OPN at median follow-up of 15.2 months, the median% eGFR preservation was 85.2% (76.4–93.3%) with no significant difference to OPN (P = .22). 9 Similarly, our study showed that the median% eGFR preservation in the RAPN group was 88% (80%–100%) at median follow-up of 59 months.
In terms of RAPN oncologic control, 1/52 patients (2.3%) had local recurrence in the anastomosis site, in agreement with the local recurrence rate of 1/65 patients (1.7%) by Autorino et al. 6 Previous studies reported no distant metastasis in their results at median follow-up of 15.2 months 9 and 12.6 months. 6 On the other hand, 1 patient (2.3%) in our RAPN cohort had distant metastasis to the lung. This difference might be attributed to the longer follow-up period in our study. Moreover, the CSS rate in our study was 100% in the RAPN cohort and 93.8% in the OPN cohort, and there was no significant difference in the 5-year CSS, MFS, and OS survival between RAPN and OPN. Interestingly, Mullerad et al. reported a CSS rate of 93% for the outcomes of centrally located tumors following OPN at median follow-up of 38.8 months. 29
Our study is not devoid of limitations. Its retrospective design may carry unintentional selection bias, as was found in the difference of eGFR and tumor complexity between groups. However, we believe that this difference emphasizes the advantages of RAPN compared to OPN,5,18 since both approaches portrayed similar oncologic control and functional outcomes. The relatively small number of patients in our study may underpower certain differences between procedures. However, our results matched most RAPN studies of totally endophytic renal tumors.6–9 Our study represents the outcomes of high-volume surgeons at tertiary-care institutions; thus, our results should be generalized with care for low-volume centers.
Our study has several strength points. It is the first study to report the long-term oncologic and functional outcomes of totally endophytic tumors treated with RAPN. Previous studies mainly focused on the perioperative outcomes,6–9 and they did not evaluate the survival rates. In addition, we compared RAPN to the gold standard OPN and demonstrated the feasibility, long-term oncologic safety, and renal function preservation of robotic surgery as an effective alternative to open surgery in treatment of such difficult lesions. Supplementary Video 1 illustrates the detailed RAPN surgical technique for endophytic tumors.
In summary, our study shows that RAPN for treatment of totally endophytic renal tumors confers excellent long-term oncologic control and functional outcomes similar to OPN.
Ethical Standards Statement
Our study was approved by the Ethics Committee Review Board of the Yonsei University College of Medicine. Ethical approval number is 2014-0091-001. All patients were fully informed with regard to the off-clamp RAPN surgical approach and its possible complications.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.