
Abstract
Abstract
Objectives:
Spleen-preserving distal pancreatectomy with splenic vessel preservation (SVP) and only the save of short gastric and left gastroepiploic vessels called the Warshaw technique (WT) are the optimal procedures to resect benign or borderline malignant tumors of the left pancreas. The aim of this meta-analysis was to assess the intra- and postoperative outcomes between SVP and the WT.
Methods:
We searched studies that compared the intra- and postoperative outcomes between SVP and the WT from PubMed, Embase, and the Cochrane Library (2004–2017). Dichotomous and continuous variables were calculated by the odds ratios and weighted mean differences with 95% confidence intervals.
Results:
Eighteen retrospective studies, including 1039 patients, were eligible for our analysis. Six hundred seventy-nine patients (65.4%) underwent SVP, and 360 patients (34.6%) underwent the WT. Although the estimated blood loss in patients undergoing the WT was less than that in those undergoing SVP (P < .00001), SVP had a lower incidence of clinically relevant postoperative pancreatic fistula (P = .03), splenic infarcts (P < .00001), intra- and postoperative splenectomies (P = .0009), and gastric varices (P < .00001) than the WT. In addition, the tumor size of patients who underwent SVP was smaller (P = .006).
Conclusions:
Both SVP and the WT are feasible and effective surgical techniques. SVP should be given priority to reduce postoperative complications, and the WT should be regarded as a salvage operation to preserve the spleen based on the preoperative evaluation or in the case of uncontrolled bleeding during SVP.
Introduction
G
In 1943, Mallet-Guy and Vachon10,11 first described the spleen-preserving distal pancreatectomy (SPDP), during which the splenic vessels were preserved by careful separation and ligation of the small pancreatic tributaries. Thereafter, surgeons attempted to improve this procedure while demonstrating its time-consuming and complex nature. In 1988, Warshaw 4 reported a new technique in which the spleen was supplied by branches of splenic vessels (short gastric and left gastroepiploic vessels). Compared with the previous methods, the Warshaw technique (WT) 4 was easier, safer, and more effective, but blood flow to the spleen was reduced. In 1996, Kimura et al. 12 first described the detailed procedure and steps of the SPDP with splenic vessel preservation (SVP) for benign lesions of the distal pancreas. With the advances in surgical techniques, it became feasible to separate the splenic artery and vein from the pancreas.
The classic SVP procedure and the WT have been widely utilized to preserve the spleen during distal pancreatectomy. The WT has been shown to be a safe and expeditious procedure that provides a greater likelihood of preserving the spleen. 13 Of note, the decreased blood perfusion may also cause a series of complications, including splenic infarctions and gastric/peri-gastric collateral formation. In contrast, SVP retains the normal anatomy and supplies more blood to the spleen. Splenic vessels, especially splenic veins, are surrounded by the pancreas and are easily injured during separation. 14 Consequently, uncontrollable bleeding may occur during SVP, which requires conversion to the WT or splenectomy during or after the operation. 15 It has been reported that SVP is always the initial plan during SPDP in some centers, and the procedures are switched to WT when the splenic vessels cannot be separated from the pancreas or the separation causes uncontrolled bleeding.16–18 The following factors were considered to influence conversion from SVP to the WT: tumor size, length of resected pancreas, tumor location, and tumor component.19,20
In this study, we primarily analyzed the intraoperative outcomes and short-term postoperative complications of SVP and WT. Further, we investigated the related parameters to decide whether or not SVP or WT should be performed.
Methods
This study was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and is registered at the International Prospective Register of Systematic Reviews (PROSPERO, number CRD 42017064109; see Supplementary Data S1.)
Search strategy
We searched relevant studies published by using the following subject headings and keywords before May 2017 in the Pubmed, Embase, and Cochrane Library databases: distal/left/body/tail; pancreatectomy/pancreas resection/pancreas excision; splenic vessels; and WT/Kimura technique (see Supplementary Data S2). The references of all the retrieved studies were searched as an additional source. The language limit in this search was English.
All of the retrieved studies were imported to Mendeley Desktop, which was used to remove duplicates. Two independent investigators (JS and SM) screened study titles and abstracts, after which we performed further screening by reviewing the full text of the selected studies. Disagreements were resolved by the third investigator (ZH).
Inclusion and exclusion criteria
Studies that met the following criteria were regarded as eligible: (1) compared distal pancreatectomy with and without SVP independent of the procedure (open surgery, laparoscopy, or robot-assisted) performed; (2) performed on benign or borderline malignant tumors of the distal pancreas; (3) provided at least one of the outcomes mentioned next; and (4) when multiple studies were reported by the same authors and institution, the subsequent article was included in the analysis.
Studies were excluded for the following reasons: (1) no comparative outcomes in the study; (2) data could not be extracted or converted to the mean and standard deviation (SD); and (3) case reports, reviews, editorials, commentaries, and letters.
Data extraction and quality assessment
Two independent investigators (JS and CM) extracted the following data from each eligible study: basic characteristics (first author, year, periods of the study, and region); population characteristics (age, gender ratio [M/F], American Society of Anesthesiologists [ASA], and body mass index [BMI]); intraoperative outcomes (tumor size [mm], operative time [minutes], estimated blood loss [mL], and postoperative hospital stay [day]); and postoperative outcomes (clinically relevant postoperative pancreatic fistula [CR-POPF] [ISGPF grades B and C], splenic infarction, intra- and postoperative splenectomy, and gastric/peri-gastric varices).
We used the Newcastle-Ottawa Scale (NOS) to assess the quality of each study. 21 Studies that scored >6 were regarded as high-quality research.
Statistical analysis
This meta-analysis was performed by using Review Manager (RevMan [version 5.3]). The odds ratios (ORs) and weighted mean differences (WMDs) were used to analyze dichotomous and continuous variables with 95% confidence intervals (CIs). A P < .05 was considered statistically significant. For continuous variables of the outcomes reported as medians and ranges, we used statistical methods to estimate the mean and the SD.22,23 Heterogeneity was quantified by using the I2, and sources of heterogeneity were analyzed by subgroup or sensitivity analysis. The potential publication bias of the selected studies was tested by using a funnel plot.
Results
Characteristics of eligible studies
As of April 2017, a total of 531 studies were retrieved from the electronic database, as follows: 276 studies from Embase, 255 studies from Pubmed, and zero studies from the Cochrane Library. After screening and according to the inclusion criteria, 16 full-text articles and 2 conference abstracts were eventually included in this meta-analysis. The NOS scores of 12 studies10,15–20,24–28 were >6. The details of the process are listed in Figure 1.
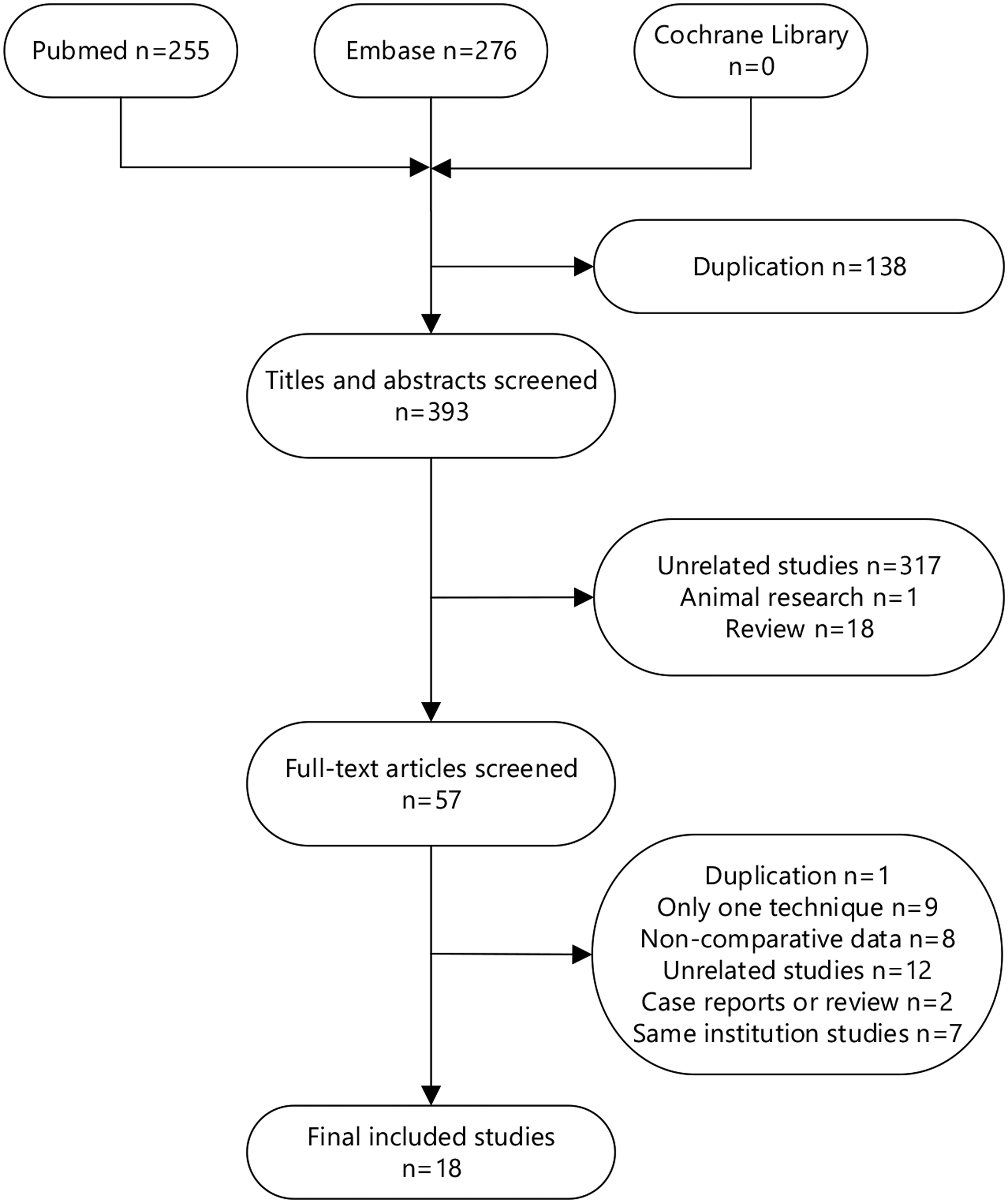
Flow diagram for selection of studies.
Eighteen eligible studies were published between 2004 and 2017, and they included 1039 patients, 679 of whom underwent distal pancreatectomies with SVP and the other 360 patients who underwent the WT. In this meta-analysis, most of the current studies involved minimally invasive surgery with the exception of two full-text articles and one conference abstract involving open surgery and a laparoscopic approach. All the other patients underwent minimally invasive surgery whether or not the splenic vessels were conserved or ligated, with the exception of 29 patients who were switched to open surgery. The basic characteristics of the included studies are summarized in Table 1.
Conference abstract.
All the patients in both groups.
ASA, American Society of Anesthesiologists; BMI, body mass index; LAP, laparoscope; NA, not available; NOS, Newcastle-Ottawa Scale; OP, open surgery; RA, robot-assisted; SVP, splenic vessels preservation; WT, Warshaw technique.
Intraoperative outcomes
Twelve studies reported data regarding operative time between SVP and the WT. The analysis showed no significant difference (WMD = 12.15; 95% CI, −9.62 to 33.92; P = .27; Fig. 2A) with high heterogeneity (I2 = 79%; x2 = 53.33; P < .00001). Sensitivity analysis was used to determine the source of the heterogeneity, but there was no change after removing any included studies. The estimated blood loss extracted from 10 studies had a statistically significant difference between SVP and the WT (WMD = 46.55; 95% CI, 27.25–65.85; P < .00001; Fig. 2B) with moderate heterogeneity (I2 = 42%; x2 = 15.50; P = .08). When the Lv study 26 was removed by sensitivity analysis, the heterogeneity changed to zero (I2 = 0%; x2 = 6.95; P = .54).
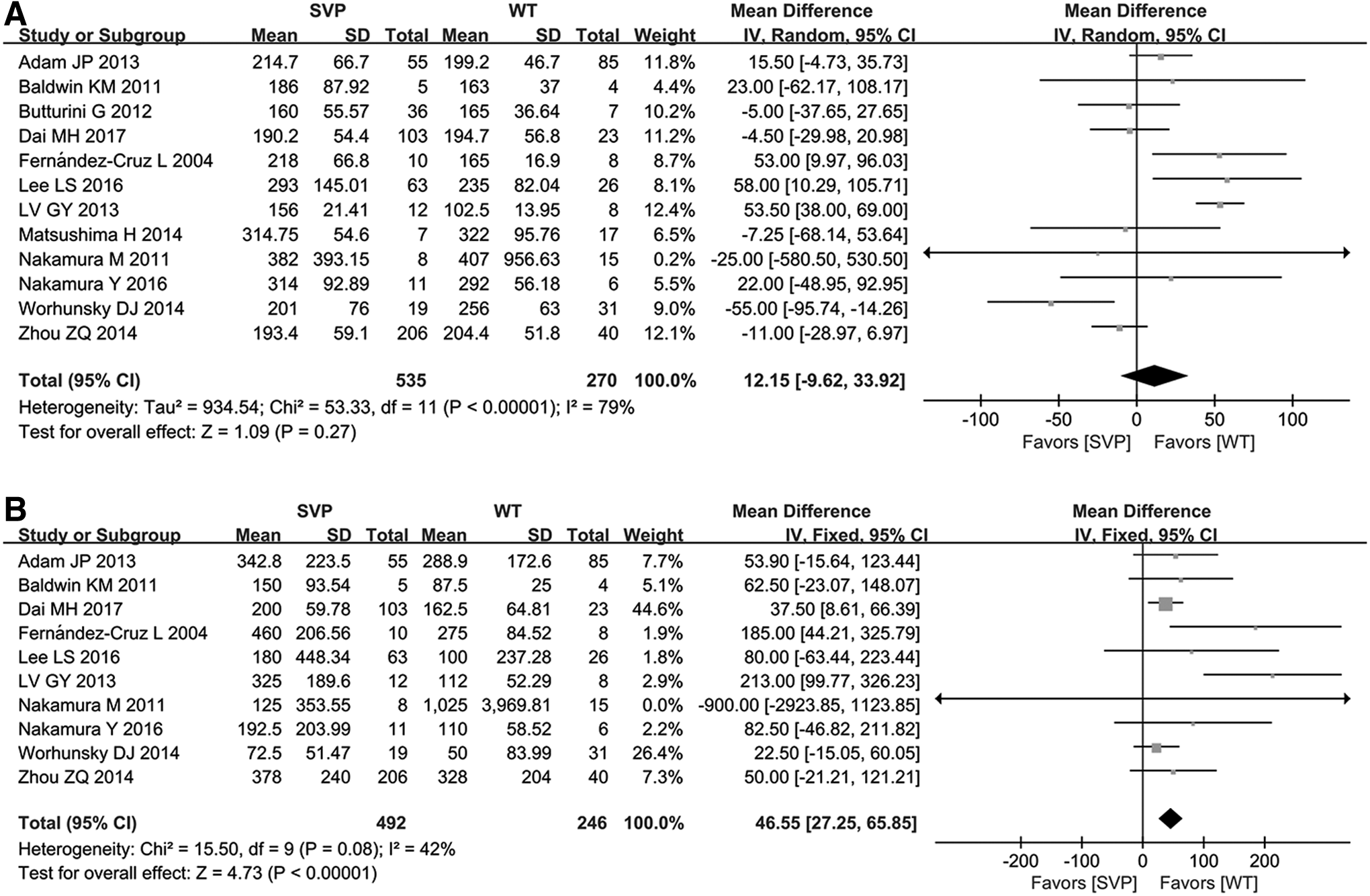
Forest plot of intraoperative outcomes: operation time
Postoperative outcomes
There was no significant difference in the postoperative hospital stays between the two techniques (WMD = −0.67; 95% CI, −1.60 to 0.26; P = .16; Fig. 3A); CR-POPF was a common complication after SPDP with SVP or the WT. Most of the complications were grade A, which did not require treatment or only required conservative treatment. In this meta-analysis, we compared CR-POPF (grade B or C) from eight studies, which were significantly different (OR = 0.48; 95% CI, 0.25–0.94; P = .03; Fig. 3B). No heterogeneity (I2 = 0%; x2 = 5.34; P = .62) was observed. There was a significant difference in the incidence of splenic infarcts between SVP and the WT (OR = 0.14; 95% CI, 0.08–0.22; P < .00001; Fig. 3C) with no significant heterogeneity (I2 = 0%; x2 = 8.70; P = .89). Further, we compared the number of patients who needed to undergo splenic resection during or after SPDP. The WT group has more severe splenic infarcts than the SVP group (OR = 0.32; 95% CI, 0.17–0.63; P = .0009; Fig. 3D) with a low-level heterogeneity (I2 = 21%; x2 = 8.77; P = .26). A significant difference existed in the incidence of gastric varices between SVP and the WT (OR = 0.19; 95% CI, 0.10–0.35; P < .00001; Fig. 3E). The heterogeneity was low grade (I2 = 21%; x2 = 12.65; P = .24).

Forest plot of postoperative outcomes: postoperative hospital stays
Intra- and postoperative switching factors
We recorded and analyzed the tumor size, length of resected pancreas, and tumor location from the patients who underwent SVP or the WT. Three studies reported that SVP was always performed first; the WT was regarded as a salvage operation when SVP was not feasible because of uncontrollable bleeding or difficult dissection. In addition, the tumor size in one study 19 was a comparison between the SVP group and the group in which SVP was converted to the WT. The other five studies selected SVP or the WT according to imaging examinations before surgery. The tumor size in the SVP group was significantly smaller than the WT group (WMD = −9.75; 95% CI, −16.73 to −2.77; P = .006; Fig. 4A) with high heterogeneity (I2 = 78%; x2 = 35.70; P < .0001). The sub-group analysis showed a significant difference (WMD = −11.83; 95% CI, −17.05 to −6.60; P < .00001) with low-grade heterogeneity (I2 = 35%; x2 = 4.65; P = .20) in the SVP sub-group first. Moreover, there was no significant difference in the intent-to-treat sub-group (WMD = −9.30; 95% CI, −23.11 to 4.51; P = .19). No significant difference existed regarding the length of the resected pancreas (WMD = −9.23; 95% CI, −25.67 to 7.17; P = .27; Fig. 4B) and tumor location (OR = 0.66; 95% CI, 0.27–1.62; P = .36; Fig. 4C).
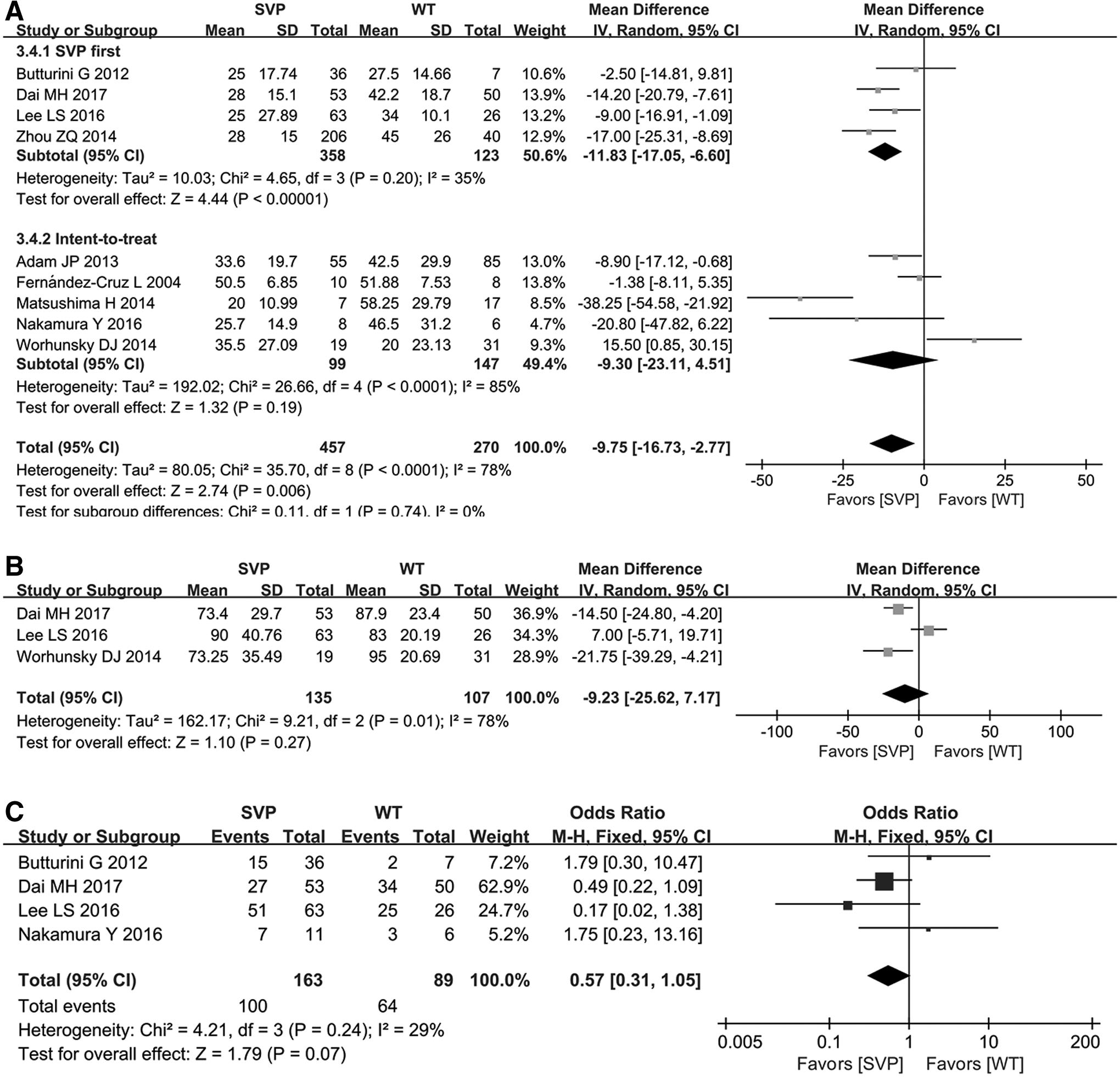
Forest plot of intra- and postoperative switching factors: tumor size
Sensitivity analysis and publication bias
The results of the analysis did not change when studies with low NOS scores29–34 were excluded. We used funnel plots to evaluate the potential publication bias. Figure 5 shows a funnel plot of the included studies, and it indicated no obvious publication bias.
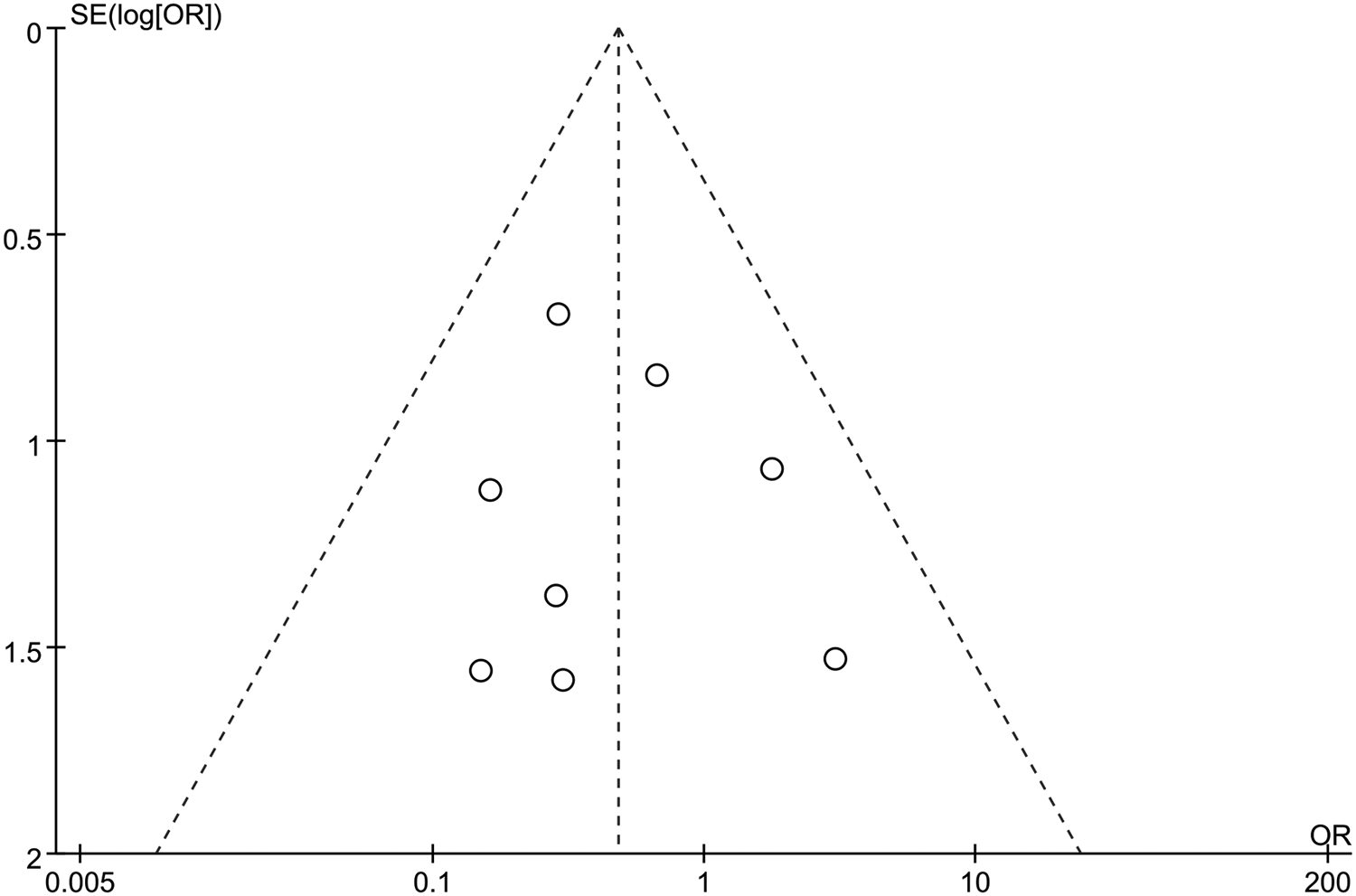
Funnel plot of clinical pancreatic fistulas. (OR; SE (log [OR]): standard error of the natural logarithm of the OR). OR, odds ratio.
Discussion
In this meta-analysis, 18 retrospective studies including 1039 patients who underwent SPDP with SVP or the WT showed that SVP has several advantages in short-term postoperative outcomes. Compared with the WT, SVP had a greater estimated intraoperative blood loss, while a lower incidence of some important postoperative complications, including CR-POPF, splenic infarctions, and gastric/peri-gastric varices in patients undergoing SVP. There were no significant differences in operative times and postoperative hospital stays. We also concluded that tumor size should be an important parameter to influence the switch from SVP to the WT.
The pooled data showed that minimally invasive surgery has become the most widely accepted approach for SPDP. Nine hundred sixty patients (92.40%) in the included studies underwent conventional laparoscopy (Lap) or robot-assisted laparoscopy (Ra-lap). Only 3.02% of the patients required conversion to laparotomy. Although hemostasis is a shortcoming of Lap, visualization of smaller vessels is enhanced, 25 and there is less postoperative pain and inflammation, and faster recovery after surgery. 35 In recent years, the Ra-lap approach has been used in distal pancreatectomies and shown to be effective, compensating for the limitations of traditional Lap with helping surgeons dissect with more precision and suture more accurately and easier, and provided a stable camera platform held by a robotic arm.36,37 All the advances just described improved the success rate of spleen preservation, and reduced damage to splenic vessels.
Anatomic location of the splenic vessels is complex, time-consuming, and delicate; numerous small vessels require separation and ligation in SVP. Indeed, previous studies reported that the WT is easier than SVP,15,26,29 but the operative time was not significantly different between SVP and the WT. In terms of our current knowledge, SVP may benefit more from the progress of surgical technology. There was significantly less estimated blood loss in the WT than SVP. Hwang et al. 38 concluded that SVP faces a higher risk of intraoperative bleeding, and even splenectomy, when dividing the splenic vessels from the pancreas, resulting from the challenging procedure and complex anatomy.
CR-POPF is regarded as one of the most common and harmful complications, and a previous study also 39 reported that the WT has an increased risk for clinical POPFs; however, the former systematic reviews and meta-analyses only compare asymptomatic and clinical POPFs, and demonstrated no significant difference between SVP and the WT. According to the 2016 update of the ISGPS definition, 40 the former grade A POPF was renamed a biochemical leak, which should no longer be quantified. We only included the former ISGPF grades B and C POPFs, and the analysis showed that the incidence of CR-POPF in patients undergoing SVP was significantly lower than the WT.
In the WT group, splenic infarctions and gastric or peri-gastric varices are well-known shortcomings caused by inadequate blood flow. Splenic infarctions may result from arterial and venous occlusion, 41 and our results also showed fewer splenic infarctions in the SVP group than the WT group. Most splenic infarctions are asymptomatic, which are revealed only by CT scan and resolved by conservative treatment. In the study, 9.13% of the splenic infarctions require splenectomy during or after surgery. Of note, Baldwin et al. 28 reported that all 4 elderly patients >70 years of age who ultimately underwent the WT developed clinical splenic infarctions in spite of precautions taken. Among of them, 3 patients still required splenectomies. Thus, the WT may not suitable for the elderly, and a splenectomy is needed when it is not possible to continue the SVP. In addition to the damage of splenic function, portal hypertension can increase the risk of gastric bleeding. As a result of sacrificing the splenic vessels, portal hypertension occurred and resulted in the development of gastric varices. In fact, no cases among the included studies reported gastrorrhagia.
The pancreatic tumor size in the SVP group was significantly smaller than in the WT group. Dai et al. 19 concluded that tumor size is positively correlated with the failure rate in SVP, and the ROC curve also showed that SVP was preferred when the cut-off level of the tumor size was ≤3 cm. In our study, the sub-group analysis showed that tumor size was an important risk factor of switching from SVP to the WT during SPDP. Zhou et al. 18 argued that it is worth attempting SVP in every patient with benign or borderline malignant tumors in the distal pancreas. This approach provides a greater probability to preserve splenic vessels during SPDP, and it may affect the operative process and prognosis of patients who need to undergo the WT initially. Notably, Hanbaro et al. 42 reported that in a group with the planned Lap-WT or early conversion to a Lap-WT, the mean operative time and estimated blood loss were significantly less than the group that underwent the WT after the SVP failure. In our analysis, six studies16–18,28,30,34 confirmed that SVP was always the initial plan and the WT was a salvage procedure when splenic vessels are impossible to conserve.
This study had the following limitations. First, all included retrospective studies have selection bias and inevitably reduced the conclusion reliability in this study. In fact, it is difficult to conduct randomized controlled trials in consideration of the safety and prognosis of the patients. Two series that were published as conference abstracts were included in this study, and they increased the potential bias. Second, in the absence of standards and with technological gaps, the observed outcomes had considerable disparities in different centers. Third, either switching to the WT during SPDP or performing the WT at the beginning of the surgery, the WT always involved a shorter distance between splenic vessels and the tumor, larger tumors, uncontrolled bleeding, and influenced the comparison between the two techniques. Finally, this study did not focus on the overall postoperative complications, the need for percutaneous drainage of organ space infection, and re-admissions or postoperative mortality, which need to be explored in future studies.
In conclusion, both SVP and the WT are safe and effective techniques but less estimated blood loss when using the WT. With respect to postoperative outcomes, the patients undergoing SVP were associated with less clinical POPFs, splenic infarctions, and secondary splenectomies. Therefore, SVP should be still given priority to reduce postoperative complications. The WT is regarded as a salvage operation to conserve the spleen according to the preoperative evaluation or while SVP could not continue due to uncontrolled bleeding. In addition, tumor size is regarded as a significant factor worth considering before surgery.
Footnotes
Acknowledgments
This project was supported by the National Natural Science Foundation of China (Grant No. 81470897). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of this article.
Authors' Contributions
J.S., Z.H., and J.L. conceived and designed this study. J.S., S.M., and T.Y. searched related studies in the databases. J.S. and S.M. screened for studies by inclusion and exclusion criteria. J.S., C.M., and J.L. extracted data and assessed included studies. J.S., T.Y., and Z.H. analyzed the data. J.S. wrote this article, and Z.H. participated in the revision. All authors approved this publication of study.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.