
Abstract
Abstract
Background:
Laparoscopic liver resection (LLR) is a high-risk and difficult minimally invasive surgery that requires a comprehensive preoperative evaluation and strict technical training. The Ban Difficulty Scoring System (DSS-B) and the Difficulty Scoring System Based on the Extent of Resection (DSS-ER) are difficulty scoring systems used in LLR. The aim of this study was to explore the clinical practicality of the DSS-B and DSS-ER in LLR.
Methods:
Differences in perioperative data were compared among different difficulty groups. The DSS-B and DSS-ER were used to evaluate the difficulty of LLR in 199 patients with tumors. Furthermore, the DSS-ER was used to evaluate the difficulty of LLR in 50 patients with intrahepatic bile duct stones (IBDSs). Finally, the correlation between the DSS-B and DSS-ER were explored.
Result:
In 199 patients who underwent LLR for tumors, the results of an intergroup comparison using the DSS-B groupings showed that operation time, intraoperative blood loss, the intraoperative blood transfusion rate, hepatic portal blockage, conversion to open surgery rate, and the postoperative hospital stay were significantly different among the groups (P < .05). Differences in perioperative data among the difficult groups were similar between the DSS-ER and DSS-B groups. A total of 50 patients who underwent LLR for IBDS were grouped based on the DSS-ER, and intergroup comparisons showed that operation time, intraoperative blood loss, the intraoperative blood transfusion rate, and the hepatic portal block rate were significantly different among the groups (P < .05). Moreover, there was a significant difference in DSS-B scores among the DSS-ER groups (P < .001).
Conclusion:
The DSS-B and DSS-ER accurately classify the degree of difficulty in LLR and therefore provide significant guidance to clinical doctors working and training in LLR.
Introduction
L
In 2014, Ban et al. proposed the Ban Difficulty Scoring System (DSS-B), which included a low-difficulty group (score = 0–3), a medium-difficulty group (score = 4–6), and a high-difficulty group (score >7) according to the difficulty of surgery based on the location and size of the tumor, the relationship between the tumor and local vessels, and the preoperative Child–Pugh rating of liver function.6,7 In 2017, Kawaguchi et al. proposed the Difficulty Scoring System Based on the Extent of Resection (DSS-ER), which was a new difficulty assessment system that was independent of the DSS-B. The DSS-ER divided patients into three grades of difficulty, including a low-difficulty group (score = 0) that included wedge-shaped lobectomies and left outer lobectomies, a medium-difficulty group (score = 2) that included anterolateral liver segment resection and left hepatectomy, and a high-difficulty group (score = 3) that included the removal of the upper hepatic segment, right posterior resection, right hepatectomy, medium hepatectomy, and the enlargement of a hepatectomy.8,9 Both scoring systems are used to classify the difficulty of LLR, with a low-difficulty surgery being suitable for a novice surgeon who has operated on less than 10 patients, a moderately difficult surgery suitable for a surgeon who has operated on 10–50 patients, and a highly difficult surgery suitable for surgeons who have operated on more than 50 patients. 10
Currently, the clinical utility of the DSS-B and DSS-ER is not universally or widely accepted. However, both the development of large endoscopy centers and improvements in the training system require a difficulty scoring system that can guide clinical practice and promote competence in LLR.
Patients and Methods
Research design
From August 2015 to November 2017, 249 patients underwent LLR at the Department of Hepatobiliary and Pancreatic Surgery at The Affiliated Hospital of Qingdao University in Qingdao, China. The following inclusion criteria were applied for the first LLR: detailed preoperative CT or MR imaging information. The following exclusion criteria were applied for LLR: tumors observed in other organs during the operation, LLR with radiofrequency ablation and laparoscopic liver caudate lobe resection. The following inclusion criteria were applied for intrahepatic bile duct stone (IBDS): LLR with IBDSs, cholecystectomy, choledocholithotomy, and detailed preoperative CT or MR imaging information. The following exclusion criteria were applied for IBDS: LLR during which complications related to other organs were encountered and complicated intraoperative choledocholithotomy. All studies were approved by the Ethics Committee of Qingdao University.
Research methods
The following perioperative indicators were used to reflect the difficulty of the operation: the operation time, intraoperative blood loss, the intraoperative blood transfusion rate, the hepatic portal block rate, conversion to open surgery rate, the postoperative hospital stay (POS), the total complication rate and the severe complication rate (Clavien–Dindo grade ≥3).11–13 We used the DSS-B and DSS-ER to classify 199 LLR cases based on difficulty. Moreover, dissection and nonanatomical classification were carried out based on the DSS-B. Based on the above eight indicators, we compared the degree of difficulty of LLR among different difficulty groups in the anatomical resection group and the nonanatomical resection group and between anatomical and nonanatomical resection groups with the same difficulty rating. Moreover, we scored 50 patients with IBDS according to the DSS-ER and compared the results for each of the above perioperative indexes between the groups. Finally, we used the DSS-ER to identify low-, medium-, and high-difficulty groups and compared the results against those obtained using the DSS-B.
Statistical analysis
All data were analyzed using the SPSS 24.0 (SPSS Statistics, Inc., Chicago, IL) statistical software package. Continuous variable data are presented as the mean ± SD. The Kruskal–Wallis rank sum test was used for multigroup comparisons, and the Mann–Whitney U test was used for comparisons between two independent groups. Classified variable data are presented as frequencies (percentages), and the χ2 test was used for comparisons between multiple groups or two groups, while Fisher's exact test was used for analyses of categorical data, as appropriate. P < .05 was considered statistically significant.
Results
Patient characteristics
Of the 249 included patients, 129 were male (51.8%) and 120 were female (48.2%), and the patients had an average age of 55.90 ± 11.38 years (range 16–82 years). The study group included 119 (47.8%) patients with hepatocellular carcinoma, 37 (14.9%) with hepatic hemangiomas, 8 (3.2%) with cholangiocarcinoma, 6 (2.4%) with hepatic metastases, 2 (0.8%) with mixed hepatocellular carcinoma, 2 (0.8%) with focal liver nodule hyperplasia and 25 (10.0%) with other lesions (inflammatory pseudotumors, liver metastases, and so on). In total, 199 patients underwent LLR for a tumor, while 50 (20.1%) underwent LLR for IBDS.
Clinical practicality of the DSS-B
In this study, we compared LLR parameters among different difficulty groups scored using the DSS-B. The 199 patients who underwent LLR were divided into three groups: 55 patients were in the low-difficulty group, 81 patients were in the medium-difficulty group, and 63 patients were in the high-difficulty group. In three sets of comparisons, our results showed that operation time, intraoperative blood loss, the intraoperative blood transfusion rate, the hepatic portal block rate, the conversion to open surgery rate, and the POS were significantly different among the groups (P < .05), while the total complication rate and severe complication rate were not significantly different among the groups (P > .05). These results are shown in Table 1.
P < .05.
POS, postoperative hospital stay; SD, standard deviation.
We next compared the same parameters among anatomical LLR patients with different levels of difficulty as determined by the DSS-B. The 105 patients who underwent anatomical LLR were divided into three groups: 2 were in the low-difficulty group, 45 were in the medium-difficulty group, and 58 were in the high-difficulty group. To reduce errors, we did not perform comparisons using the low-difficulty group because of its small sample size. We therefore compared the medium-difficulty group with the high-difficulty group. The results showed that operation time, intraoperative blood loss, the intraoperative blood transfusion rate, the total complication rate, and the POS were significantly different between the groups (P < .05), while the hepatic portal block rate, the conversion to open surgery rate, and the severe complication rate were not significantly different between the groups (P > .05). These results are shown in Table 2.
P < .05.
POS, postoperative hospital stay; SD, standard deviation.
We next compared the parameters among nonanatomical LLR patients scored with different levels of difficulty using the DSS-B. The 93 patients who underwent anatomical LLR were divided into three groups: 52 were in the low-difficulty group, 36 were in the medium-difficulty group, and 5 were in the high-difficulty group. Because of its small sample size, we did not include the high-difficulty group in the subsequent analyses. Comparisons between the low-difficulty group and the medium-difficulty group showed that the POS was significantly different between the groups (P < .05), while operation time, intraoperative blood loss, the intraoperative blood transfusion rate, the hepatic portal block rate, the conversion to open surgery rate, the total complication rate, and the severe complication rate were not significantly different between the groups (P > .05). These results are shown in Table 3.
P < .05.
POS, postoperative hospital stay; SD, standard deviation.
We next compared the patients in the anatomical and nonanatomical LLR groups who were scored with the same difficulty using the DSS-B. Of the 199 patients who underwent LLR, the low-difficulty group included 3 patients treated with anatomical LLR and 52 patients treated with nonanatomical LLR, the medium-difficulty group included 45 patients treated with anatomical LLR and 36 patients treated with nonanatomical LLR, and the high-difficulty group included 58 patients treated with anatomical LLR and 5 patients treated with nonanatomical LLR. Because of its small sample size, we did not include the low-and high-difficult groups in the subsequent analyses. We therefore compared the anatomical and nonanatomical LLR groups that were scored as having medium-difficulty group according to the DSS-B. The results showed that operation time, intraoperative blood loss, the intraoperative blood transfusion rate, the hepatic portal block rate, the conversion to open surgery rate, the POS, the total complication rate, and the severe complication rate were not significantly different between the two groups (P > .05). These results are shown in Table 4.
POS, postoperative hospital stay; SD, standard deviation.
Clinical practicality of the DSS-ER
We compared LLR patients with different difficulty scores according to the DSS-ER. We divided the 199 patients who underwent LLR into three groups: 61 were in the low-difficulty group, 108 were in the medium-difficulty group, and 30 were in the high-difficulty group according to the DSS-ER. Comparisons among the three groups showed that operation time, intraoperative blood loss, the intraoperative blood transfusion rate, the hepatic portal block rate, the conversion to open surgery rate, the POS, and the severe complication rate were significantly different among the groups (P < .05), while the total complication rate was not significantly different among the groups (P > .05). These results are shown in Table 5.
P < .05.
POS, postoperative hospital stay; SD, standard deviation.
We next compared LLR patients with IBDS scored as different levels of difficulty according to the DSS-ER. The 50 patients who underwent LLR for IBDS were divided as follows: 25 patients were in the low-difficulty group, 20 were in the medium-difficulty group, and 5 were in the high-difficulty group. Comparisons among the three groups showed that operation time, the intraoperative blood loss, intraoperative blood transfusion rate, and the hepatic portal block rate were significantly different among the groups (P < .05), while the conversion to open surgery rate, the POS, the total complication rate, and the severe complication rate were not significantly different among the groups (P > .05). These results are shown in Table 6.
P < .05.
POS, postoperative hospital stay; SD, standard deviation.
Correlation between the DSS-B and DSS-ER
The DSS-ER divided the 199 patients who underwent LLR as follows: 61 were in the low-difficulty group, 108 were in the medium-difficulty group, and 30 were in the high-difficulty group. The median scores these groups received when using the DSS-B were 3, 6, and 10, respectively (Fig. 1). The differences between the groups were statistically significant (P < .001).
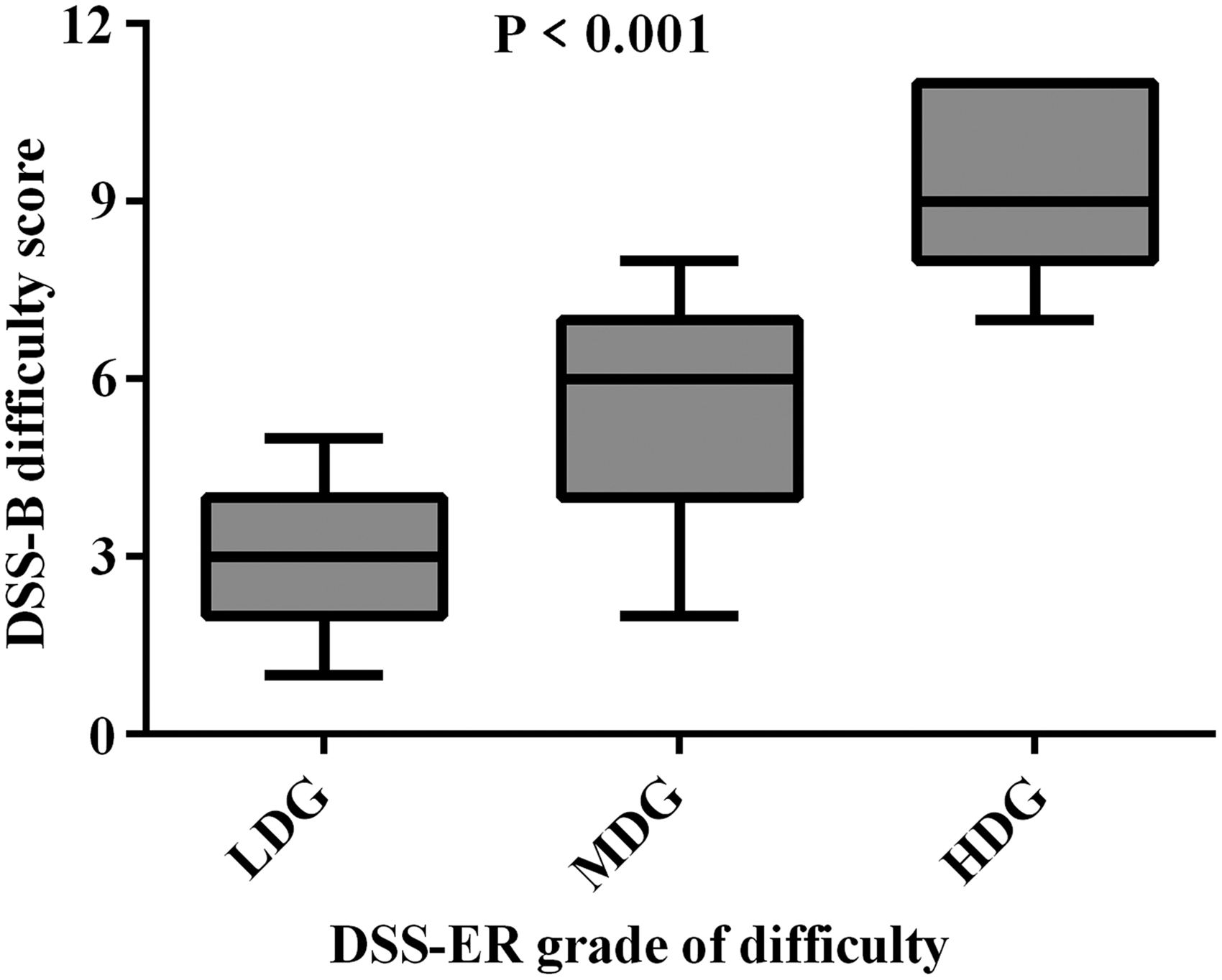
Correlation between the DSS-B and DSS-ER in LLR. LDG versus MDG versus HDG (P < .001). DSS-B, Ban Difficulty Scoring System
Discussion
LLR is one of the most complicated surgeries of the liver and is associated with a high level of risk, a high-difficulty level, and a high degree of technical requirements. Hence, a sound thorough preoperative evaluation and strict technical training are required.14,15 Traditional preoperative assessment systems and general surgical training methods have failed to keep pace with the development of LLR technologies.16,17 Obtaining an accurate preoperative assessment of surgical difficulty can help the surgeon choose an LLR operation with the appropriate level of difficulty and ensure that procedures are in line with a surgeon's growth requirement and the fundamental interests of the patients.18,19 According to the International Conference on LLR, which was held in Morioka, Japan in 2014, small-scale LLR can be considered as a routine procedure, but a full evaluation is still needed in such cases. Extensive LLR remains under study, and it is possible for a surgeon to continue to learn while cautiously performing such surgeries under the supervision of another surgeon with adequate laparoscopic experience.20,21 Nomi et al. used the cumulative sum method to evaluate the learning curve for 173 cases of LLR. Their research confirms that the learning curve comprised three phases: an initial phase of 45 patients, an intermediate phase of 30 patients, and a final phase of 98 patients.22–25 These stages correspond to the three difficulty levels defined by difficulty scoring systems. Therefore, a difficulty scoring system can be used to develop a reasonable training program that may shorten a surgeon's growth cycle so that they can advance from simple to complex LLR procedures.26–28
When 199 LLR surgeries were scored using the DSS-B, the results showed that there were significant differences in perioperative data between groups rated with different levels of difficulty. There were more nonanatomical LLR cases in the low- and middle-difficulty groups, and the majority of cases in the high-difficulty group underwent anatomical LLR. There were no significant differences between the anatomical and nonanatomical resection patients in the middle-difficulty group. This finding demonstrates that the DSS-B objectively reflects the difficulty level of the LLR procedure. The DSS-B basically produces the same results as those described in the study by Ban et al. 6 Therefore, it can be used to evaluate preoperative LLR difficulty. When 199 LLR cases were scored using the DSS-ER, there were significant differences in perioperative indexes between groups based on the extent of resection and the complexity of the anatomical structures involved, demonstrating that the DSS-ER objectively reflects the difficulty level of the LLR procedure, which is in line with Kawaguchi's findings. 9 However, when 50 patients who underwent LLR for IBDS were scored using the DSS-ER, the results only partly reflected the level of surgical difficulty. This result may be related to the complexity of IBDS itself and its association with additional biliary surgery. The inclusion criteria for the DSS-ER did not include LLR for IBDS, and we have therefore included a preliminary discussion here with the aim of adding IBDS-related factors to the scoring system in the future.29,30 The accuracy of the DSS-ER may be improved by including IBDS-related parameters for LLR. 31 At last, we explored the correlation between the two scoring systems. Also, the results showed that the DSS-B and DSS-ER systems are highly correlated. Therefore, both scoring systems can evaluate the difficulty of LLR in patients with tumors.
Because there are differences in their scoring standards, each of the DSS-B and DSS-ER systems has its own characteristics. The DSS-ER system is based on the extent of resection, which includes characteristics with simplicity and a wide range of applications. However, it ignores the basic condition of the patient and the difficulty of the operation, and its accuracy will be affected. The DSS-B system is a comprehensive scoring system based on the results of a preoperative examination. It is more accurate and targets specific features but cannot be applied in IBDS patients and does not meet the needs of the broad disease spectrum encountered by physicians in China. We therefore suggest that the two scoring systems should be combined in clinical practice to increase the accuracy of the assessment.
The DSS-B and DSS-ER are based on retrospective studies performed in multiple centers are continuously improved as techniques to treat LLR develop. Several clinical centers in Japan are involved in an ongoing prospective study of LLR difficulty scoring systems, and their findings will allow difficulty scoring systems to better assess the difficulty of surgeries and to predict the course of recovery after surgery, thereby greatly improving the clinical value of these systems.32–34
In summary, the DSS-B and DSS-ER complement each other as independent and reliable systems for evaluating the difficulty of LLR in a clinical setting. The clinical application of LLR difficulty scoring systems promotes the development of safe, standardized, effective evaluation and training systems for surgeons performing LLRs. In addition, minimally invasive technologies are continually being developed, allowing more patients to benefit from these treatments.
Footnotes
Acknowledgment
This work was supported by the Shandong Science and Technology Development Plan Foundation.
Disclosure Statement
No competing financial interests exist.