
Abstract
Abstract
Purpose:
To evaluate the safety and efficacy of percutaneous transhepatic route creation for hepatic vein (HV) angioplasty in Budd–Chiari syndrome (BCS).
Patients and Methods:
Between April 2012 and August 2016, a total of 19 BCS patients underwent percutaneous transhepatic route creation for HV angioplasty after transvenous catheterization failure in this study. Color Doppler ultrasonography was required in all patients after admission and during follow-up. Data were retrospectively collected, and follow-up observations were performed.
Results:
Technical and clinical success was achieved in 18 patients. Except for 1 failure of route creation, 19 routes were successfully created in 18 patients, with a technology success rate of 95.0%. Twenty-two balloon angioplasties were performed in 18 patients, with a mean balloon diameter of 13.6 ± 0.5 mm. Blood pressure and length of occlusive HV decreased significantly, and blood flow velocity and diameter of HV increased significantly after procedure. Abdominal distension/pain and ascites decreased significantly after procedure. One procedure-related death occurred, who died of gastrointestinal bleeding 6 days later. Except for the failure case, the rest of 18 patients were successfully followed up. The remaining 18 patients survived during follow-up, with a 5-year survival rate of 94.9%. One patient had a restenosis of HV after 47 days, and had undergone successful dilation. The 5-year primary and second patency rates were 94.1% and 100%, respectively.
Conclusion:
Percutaneous transhepatic route creation is safe and effective for HV angioplasty, and can be used to treat BCS patients after transvenous catheterization failure.
Introduction
B
Materials and Methods
This retrospective study was approved by our Institutional Review Board. All procedures were performed in accordance with the ethical standards. Written informed consents for the procedure were obtained from all patients in this study.
Study design and patient selection
From April 2012 to August 2016, a total of 131 patients underwent HV recanalization in our department; of which, 112 patients were successfully treated by the transvenous approach, and the remaining 19 BCS patients with failure of HV recanalization by transvenous approach were enrolled in this study. The inclusion criteria are a definite diagnosis of BCS due to HV obstruction and a failure of HV recanalization by transvenous approach. Patients with severe liver function failure, HV obstruction caused by malignancy, terminal hepatic carcinoma, and massive ascites making difficulty in percutaneous transhepatic puncture, severe dysfunction of blood coagulation, active infection, or bleeding were excluded from this study. Patient characteristics, the main clinical symptoms and technology outcomes were collected and analyzed.
Diagnosis and definition
Diagnosis was established by reviewing the patients' history as well as the results of magnetic resonance angiography, contrast-enhanced CT angiography, or color Doppler ultrasonography. The HV and IVC angiography confirmed diagnosis during interventional procedure. Failure of transvenous catheterization was defined as an unsuccessful catheterization through the femoral vein (FV) approach, or internal jugular vein (IJV) approach, or both approaches. Technical success was defined as a complete elimination of HV obstruction confirmed by venography. Clinical success was defined as a stable or improved symptom within 1 week of technically successful HV recanalization.
Percutaneous transhepatic route creation
The patients lay in a supine position. All procedures were performed under local anesthesia with 2% lidocaine and fluoroscopic guidance. The hunter head catheter was first catheterized to the lesion HV for percutaneous transluminal balloon angioplasty. Then percutaneous transhepatic puncture performed if catheterization failed. A 0.014-inch platinum micro guide wire (Cook, Bloomington, IN) was introduced into the HV through the sheath of a Chiba needle (Cook). A 5F vascular sheath was implanted; a 5F catheter was introduced through the sheath. The guide wire successfully catheterized the involved HV and was introduced into the IVC. Then 12–14F-long sheaths were introduced through the FV (Fig. 1) or IJV (Fig. 2). Amplatz gooseneck snare (Microvena, MN) was used to capture the guide wire and to drag it out through the long sheath, to successfully establish the percutaneous transhepatic route. The occlusive segment of HV was dilated by using a balloon of 8–18 mm diameter and 40–60 mm length (Venous balloon; Cook Medical). The balloon was dilated twice, and each dilation lasted ∼30 seconds. HV/Accessory HV (AHV) pressure was measured by using a piezometric tube before and after angioplasty. After stent angioplasty, the procedure path was sealed with an embolization coil or gelatin sponge.
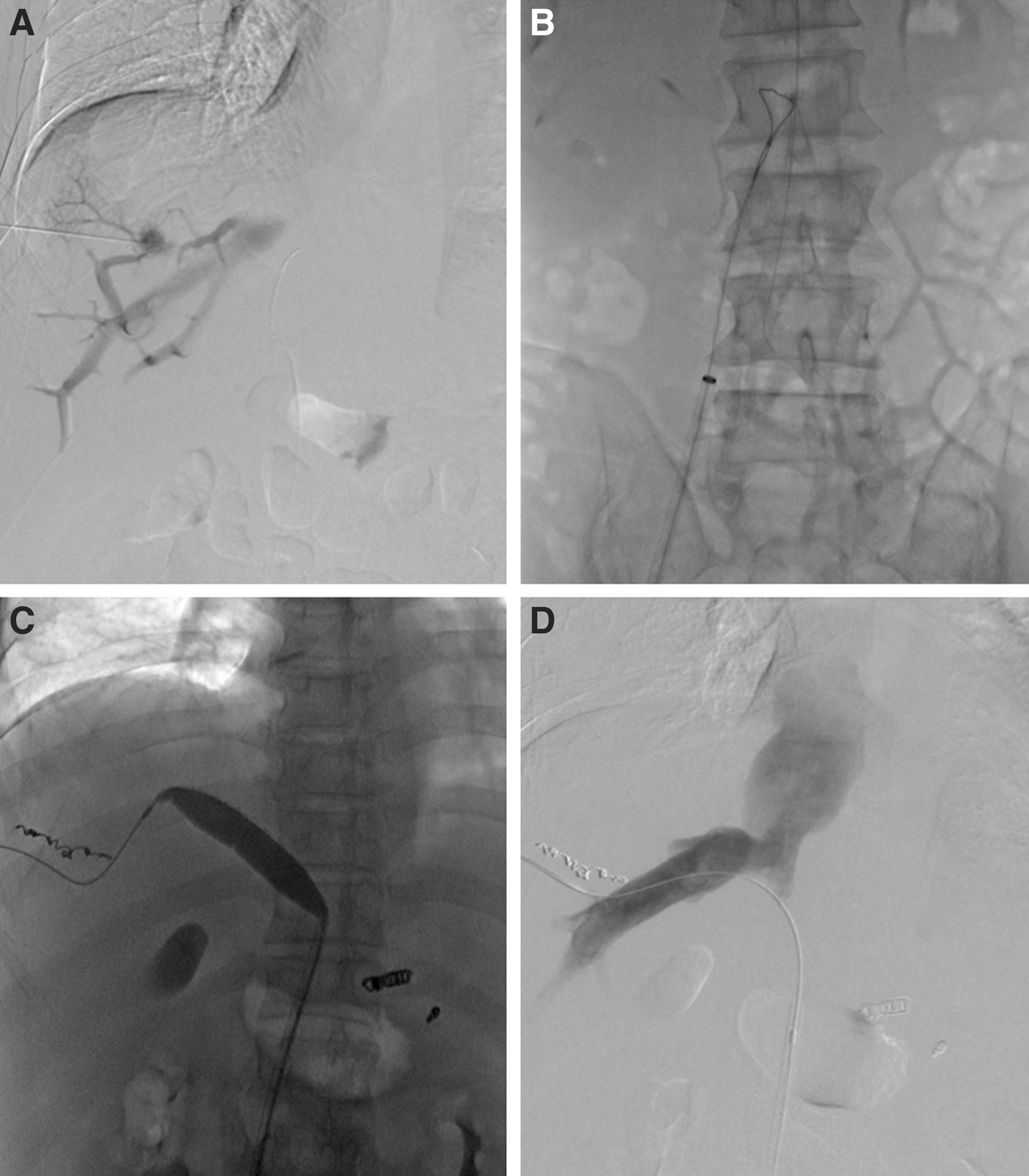
Balloon angioplasty through percutaneous HV/FV track.

Balloon angioplasty of left main HV through percutaneous HV/IJV track.
Perioperative care and medicine
Heart rate, blood pressure, oxygen saturation, and respiratory rate were monitored throughout the procedure. The low-molecular-weight heparin of 5100 U was subcutaneously injected every 12 hours for 4–5 days. Patients were monitored for 1–2 days postoperatively to observe complications, including bleeding. All patients took oral warfarin (Xinyi Pharmaceutical Co.) for anticoagulation from the second day following treatment for 2 years, with international normalized ratio of 2 to 3.
Follow-up
All patients were followed by abdominal Doppler ultrasound with or without CT angiography about 1 week after procedure, and every 3–6 months to confirm the patency of the HV (Fig. 3). Patient's conditions were ascertained by contacting the patients or their family every 3 months after treatment.

Color Doppler ultrasonography after procedure. The patency of left HV and IVC was confirmed by color Doppler ultrasonography during follow-up. HV, hepatic vein; IVC, inferior vena cava.
Statistical analysis
All data were expressed as mean ± SEM. Student t test was used for statistical analysis (Prism 5.0; GraphPad Software, Inc., San Diego, CA). Differences were considered statistically significant at P < .05.
Results
Patient characteristics
A total of 19 patients, including 11 males and 8 females (mean age 37.1 ± 3.0 years) were enrolled in this study. Ten patients (52.6%) had a combined IVC and HV involvement, and 11 (55.0%) patients had a complete occlusion of HVs or AHVs. Eight patients had a duration of symptom within 1 year, and 5 patients had a duration more than 10 years. Abdominal distension and pain were the most common symptom and sign, which were shown in 68.4% of cases (Table 1).
AHV, accessory hepatic vein; HV, hepatic vein; IVC, inferior vena cava.
Percutaneous transhepatic route creation
Transvenous catheterization failures included 11 of FV approaches, 6 of IJV approaches, and 2 of both approaches. One failure of route creation was found in 1 patient with all 3 HV occlusions, 19 routes were successfully created in the remaining 18 patients. Percutaneous HV/FV route was successfully created in half of patients. The technology success rate was 95.0% (19/20). Clinical success was achieved in 18 patients (94.7%). Twenty-two balloon angioplasties were performed in 18 patients, with a mean balloon diameter of 13.6 ± 0.5. Nineteen HVs/AHVs were successfully dilated, including 4 AHVs (Table 2).
AHV, accessory hepatic vein; FV, femoral vein; HV, hepatic vein; IJV, internal jugular vein.
Change of HV/AHV and symptoms/signs
The mean pressure of HV/AHV decreased from 40.8 ±2.8 cm H2O before treatment to 27.0 ± 1.8 cm H2O after treatment (P = .0006). Length of occlusive HV decreased significantly after procedure (P < .0001). Blood flow velocity and diameter of HV increased significantly after procedure (P < .01). Abdominal distension/pain and ascites decreased significantly after procedure (P < .01). Other symptoms, such as lower extremity edema/pain did not change significantly (Table 3).
AHV, accessory hepatic vein; HV, hepatic vein.
Perioperative complications and follow-up
One procedure-related death was found, who died of gastrointestinal bleeding 6 days after leaving hospital. One patient had mild skin anaphylaxis after the procedure, and the symptoms disappeared after the immediate administration of 10 mg of dexamethasone. This procedure did not result in further thrombosis or increase in the portal pressure and variceal bleeding. Except for failure 1, all 18 patients were successfully followed up, with a mean duration of 47.7 ± 5.1 months; the rest of 18 patients survived during follow-up, with a 5-year survival rate of 94.9%. One patient had a restenosis of HV after 47 days, and had undergone successful dilation again. The 5-year primary and second patency rates were 94.1% and 100%, respectively (Fig. 4).
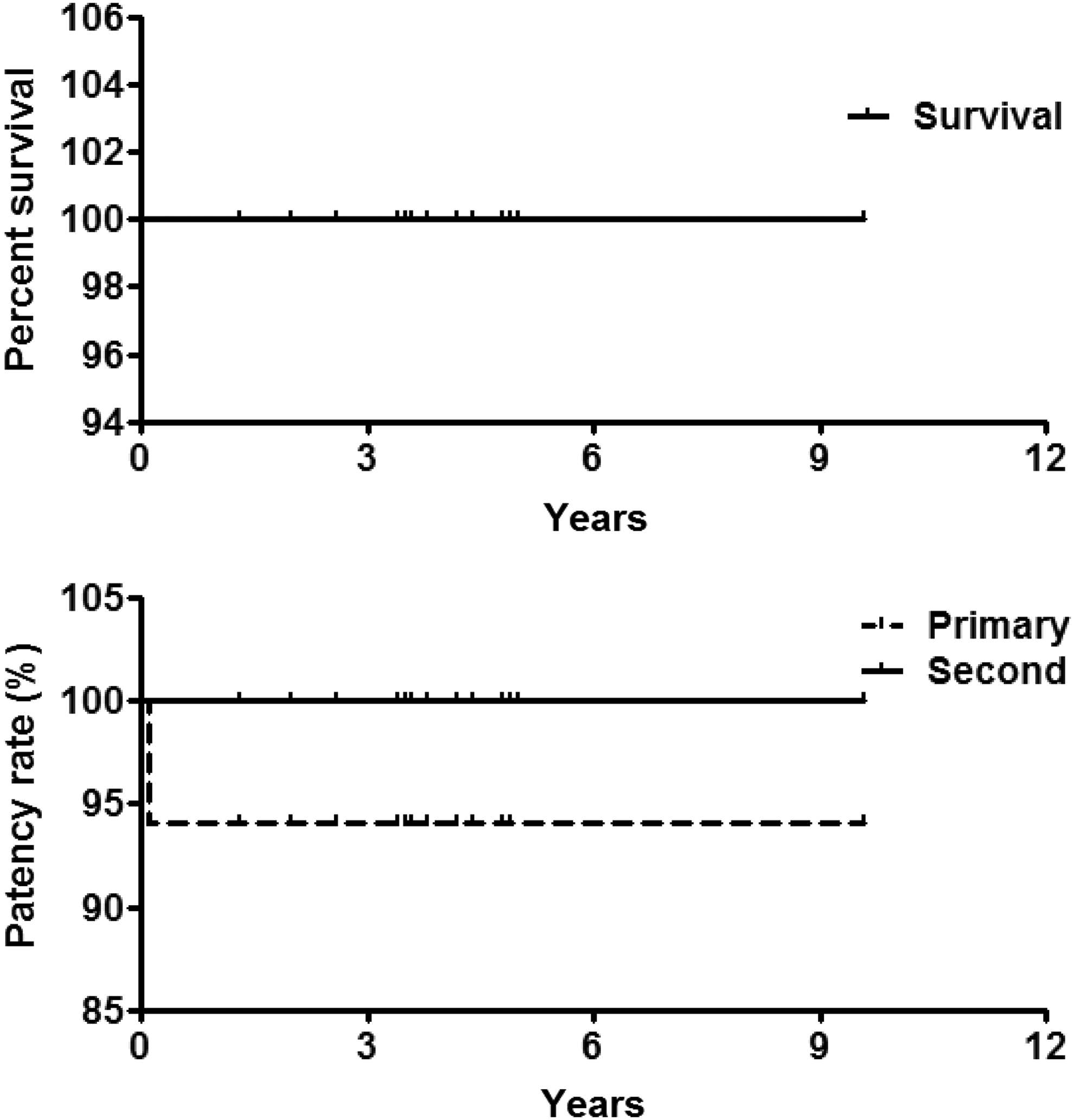
Patency rate and survival rate follow-up. The 5-year survival rate was 94.9%. The 5-year primary and second patency rates were 94.1% and 100%, respectively.
Discussions
The interventional treatments for BCS with HV lesions include balloon angioplasty, stent implantation, and TIPS. Since initial success in balloon angioplasty in 1974 12 and stent placement in 1990, 13 interventional treatments have proven efficacy for BCS. Unfortunately, HV recanalization sometimes is quite difficult due to long-segment obstruction or complete occlusion of HV outlet.4,9
This study evaluated the safety and efficacy of percutaneous transhepatic route creation for HV angioplasty in BCS patients after transvenous catheterization failure. The initial results were satisfactory, demonstrating high technical and clinical success rates. During a 5-year follow-up, the 5-year primary and second patency rates were 94.1% and 100%, respectively. These positive results may be attributable to the following factors: first, percutaneous transhepatic routes help to improve the support of the catheter thus increase the success rate of angioplasty. Second, AHV dilates to compensate and function as drainage vessels after main HV obstruction. These AHVs also received angioplasty to maximize the clinical efficacy and avoid TIPS or surgical shunt. Although TIPS has been used for BCS due to HV obstruction to decrease the portal vein pressure,8,14 hepatic encephalopathy and shunt dysfunction are troublesome problems.8,15
Currently, HV recanalization has been increasingly used for the treatment of BCS to relieve the symptoms and hepatic congestion.4,9,16,17 However, the challenges and difficulties of HV recanalization may encounter owing to the following factors: first, it is not so easy to cut through the HV obstruction, especially the long segment of obstruction through transvenous approaches.4,9 Second, stump or outlet of HV may disappear in BCS patient with severe stenosis or complete obstruction of the HV, making the catheterization difficult.
To shorten the operation time and avoid an excessive X-ray radiation, it is unnecessary to take too long to canalize the occluded HVs. According to our experience, percutaneous transhepatic route should be created due to transvenous catheterization failure. Besides, the balloon diameter selection for HV still lacks unified standards. Early clinical experience shows that a high recurrence rate was found after the use of 12 mm balloon catheter. Nowadays, a larger diameter balloon expansion is performed. No stents were used to avoid long-term complications in our study, which was different from the report in the literature. 11
There are some limitations to this study: First, the present report was a retrospective case analysis, and the sample size was small. Second, it is not a comparative study. However, the purpose of this study was to provide an additional treatment option for patients with BCS due to long-segment obstruction of HV.
In conclusion, percutaneous transhepatic route creation is safe and effective for HV angioplasty, and can be used to treat BCS patients after transvenous catheterization failure.
Footnotes
Acknowledgments
This work is supported by the National Natural Science Foundation of China (Grant No. 81501569). The authors extend their appreciation to Dr. Linxia GU, Department of Mechanical and Materials Engineering, University of Nebraska–Lincoln, Lincoln, NE 68588–0656, USA, for her valuable comments and English editing.
Disclosure Statement
No competing financial interests exist.