
Abstract
Abstract
Background:
Recent reports have suggested that the use of the robot might reduce the rate of pancreatic complications following minimally invasive radical gastrectomy.
Methods:
By meta-analyzing the available literature, we aimed to elucidate possible differences between conventional laparoscopic and robotic radical gastrectomy on pancreatic morbidity.
Results:
More than 2000 patients from eight studies were eventually included in the analysis. The overall incidence of postoperative pancreatic complications was 2.2%, being 1.7% and 2.5% following robotic and laparoscopic gastrectomy (LG), respectively. In particular, pancreatic fistula occurred in 2.7% of patients receiving robotic gastrectomy (RG) and 3.8% of patients receiving laparoscopy.
Conclusions:
The use of the robot showed a trend toward better outcomes compared with laparoscopy, despite the presence of more advanced disease and higher body mass index. The meta-analysis resulted in an odd ratio of 0.8 favoring RG over LG on pancreatic morbidity, although without statistical significance.
Introduction
A
MIG has been now almost universally accepted as a valid option for the treatment of gastric cancer, with special emphasis for stage I malignancies.13–15 Improved overall morbidity, shorter hospitalization, and earlier return to daily activities are some of the main factors favoring MIG over conventional open gastrectomy (OG).13–15 Despite this, during the last few years there have been a number of reports showing a higher rate of injury to the pancreas in laparoscopic gastrectomy (LG) compared with OG.6,11,16–19 On the contrary, others have suggested that the use of the robot may be utile in reducing such morbidity.6,7,20–22
We recently investigated the available scientific evidences on the incidence of pancreas-related complications after radical gastrectomy. 3 The overall incidence of AP and POPF was 0.6% and 1.4%, respectively. Interestingly, MIG was associated with a higher rate of pancreatic morbidity compared with OG. Nevertheless, from the pooled data in the meta-analysis, it was not possible to divide the results of MIG between standard laparoscopy and robotic laparoscopy.
The purpose of this study was to assess the available literature on whether robotic gastrectomy (RG) may present some advantages over conventional LG in terms of pancreatic morbidity.
Methods
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) 23 and MOOSE (Meta-analysis of Observational Studies in Epidemiology) 24 guidelines were used to identify the existing studies comparing RG with LG. Accordingly, an itemized protocol to perform the meta-analysis was produced before data collection.
Two authors (F.G., G.G.) performed the literature search up to September 2017 independently. The PubMed/MEDLINE and EMBASE electronic databases were queried as follows: “robot” or “robotic” and “gastrectomy.” Our search was restricted to English language. The 2 authors screened titles and abstracts of the retrieved records. Differences in opinion were resolved by discussion. Full-text versions of studies considered for inclusion were appraised and relative bibliographies were hand searched to find further eligible works.
Any potentially eligible study was assessed and included in the meta-analysis if the following criteria were met:
Studies on patients undergoing radical gastrectomy for gastric cancer with curative intent Randomized controlled trials (RCTs) or observational studies comparing RG versus LG Report of pancreatic event (AP or POPF) rate of RG and LG independently.
To evaluate any bias of matching between the two groups of patients, studies were included in the pooled analysis only in the presence of adequate reporting of the following data about RG and LG: age, body mass index (BMI), tumor staging, and type of surgical procedure. According to the Cochrane Handbook for Systematic Reviews of interventions guidelines for rare events, were excluded from the analysis those studies reporting no pancreatic events. The same guidelines were used to assess methodological quality. 25
In the case of multiple studies by the same authors or multicentric studies with overlap among patients groups, the most recent or the most informative data were considered. From each eligible study the following data were extrapolated: study design, type of surgical procedures, and number and clinical characteristics of patients in each group. Overall, pancreas-related morbidity and the relative incidence of AP and POPF were the primary endpoints. Secondary endpoints were operative time, length of hospital stay, and number of lymph nodes yielded.
Statistical analysis
Data are presented in descriptive statistics. Statistical analysis was performed using the Statistical Package for the Social Sciences v 20.0 (SPSS Inc, Chicago, IL). Where needed, medians with ranges were converted into means with standard deviations according to the method popularized by Hozo et al. 26 Meta-analysis was performed with Review Manager 5.3 (Cochrane Collaboration, Oxford, England) under the random-effects model. Estimated effect measures were calculated for event-related outcomes as odds ratios (ORs). For continuous variables, mean differences (MDs) were calculated with the inverse variance method. Statistical heterogeneity was assessed by inspecting the forest plots and I 2 statistics. ORs and MDs were identified and reported with 95% confidence interval. The Z test for overall effect and its two-sided P value were also assessed. Statistical significance was set at the .05 probability level.
Results
Study selection and quality assessment
Our initial database query resulted in 815 records. By assessing titles and abstracts, a total of 41 potentially pertinent records were identified. Twelve additional records were identified by hand searching of bibliographies, resulting in a total amount of 53 records.27–77
After the evaluation of the full-texts, eight studies21,22,30,34,38,41,53,64 met all the inclusion criteria and were considered eligible for data extraction and meta-analysis. The remaining records were excluded for the following reasons: absence of a comparator group (2 records39,72), absence or impossibility to extrapolate detailed data on patient characteristics or pancreatic morbidity (27 records17,35–37,40,43–49,51,54–59,60,62,63,66–70), review articles (11 records7,27–29,30–33,50,52,61,71), and presence of duplicate data (5 records8,20,42,65,73). Figure 1 describes the selection process. Table 1 shows the general characteristics of the included studies.
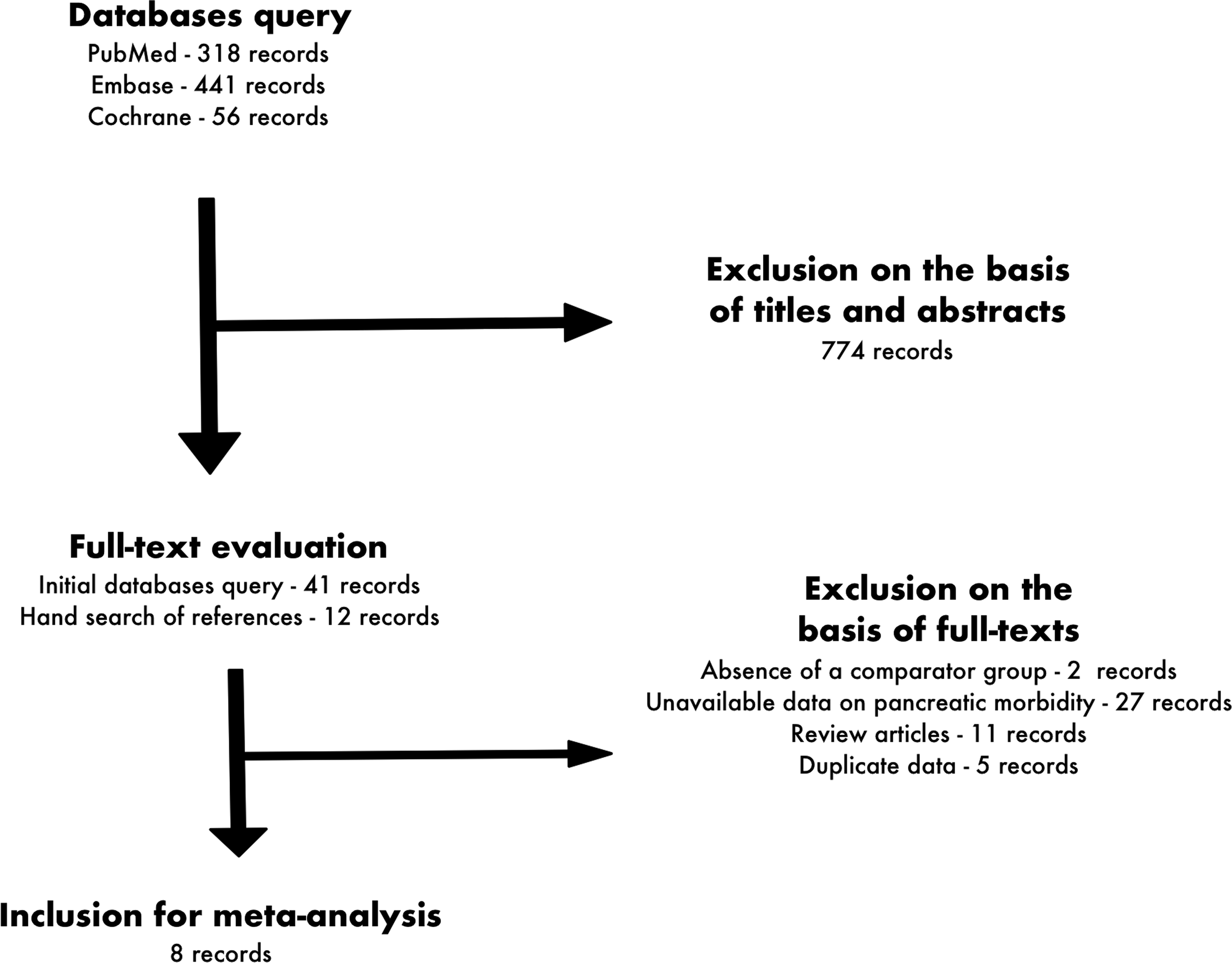
The flow diagram illustrating the selection process.
BMI, body mass index; L, laparoscopic; R, robotic; DG, distal gastrectomy.
There were no randomized trials comparing LG with RG and all included studies21,30,34,38,41,53,64 were retrospective in nature, with the exception of the study by Noshiro et al., 22 which is a prospective, nonrandomized trial. Although all studies had consecutive cases collected from contemporary groups of patients, clinical heterogeneity was considerable mostly due to the lack of detailed endpoints. In general, specific detection and selection biases were present in all of the included studies. This was essentially because of the absence of detailed diagnostic criteria to define AP and POPF and the lack of systematic and reproducible postoperative assessment of pancreatic morbidity. In all measurements of the outcomes of interest, the I 2 index revealed a low risk of heterogeneity (I 2 = 0%–44%).
Baseline characteristics and outcome evaluation
A total of 2026 patients were finally considered eligible for the meta-analysis, 1456 undergoing LG and 570 undergoing RG. Five studies21,22,30,34,41 included solely patients receiving distal gastrectomy, while the remaining three studies38,53,64 included data concerning all types of gastrectomy. All studies reported on patients undergoing gastrectomy with D1+/D2 lymphadenectomy, the only exception was the article by Parisi et al., 53 containing data concerning D2 lymphadenectomy solely.
Mean ages ranged between 55 and 74 years for LG and between 51 and 73 years for RG. Overall, patients undergoing RG were younger than those receiving LG (MD −3.2, [−5.36, −1.04], Z = 2.91, P = .004). RG patients had significantly higher BMI compared with LG patients, with an MD of 0.38 [0.09, 0.67], Z = 2.58, P = .01. With regard to tumor stage, two studies22,64 included patients with gastric malignancies of all stages; the majority of studies21,30,34,38,41,53 included patients with stages I–III disease. By assessing each included article in particular, there was no statistical difference between the LG and RG group in terms of tumor stage, with the exception of the studies by Eom 34 et al. and Suda et al., 64 in which patients receiving RG had more advanced disease compared with those undergoing LG. Clinicopathologic characteristics are given in Table 2.
Statistical significance.
L, laparoscopic; NS, not significant; R, robotic.
Overall, the rate of postoperative morbidity related to the pancreas was 2.2%, with 46 cases of AP/POPF among a total of 2026 patients. Globally the rate of pancreatic morbidity ranged between 0.8% 38 and 16.2%. 53 At the meta-analysis, pancreatic morbidity (Fig. 2) tended to occur less frequently following RG (10 out of 570 patients, 1.7%) than after LG (36 out of 1456 patients, 2.5%), with an OR of 0.8 [0.31, 2.04], although without statistical significance (Z = 0.47, P = .64). The general incidence of postoperative AP was 0.5%, being 0.6% and 0.5% for RG and LG, respectively (data on 1463 patients from five studies,30,34,38,41,64 OR = 1.24, Z = 0.32, P = .75). In total, POPF occurred in 38 patients (3.5%). Of note, the rate of POPF was 2.7% after RG and 3.8% after LG, with an OR of 0.72 [0.15, 3.56] (data on 1089 patients from four studies,21,22,53,64 Z = 0.40, P = .69). Specific data concerning POPF severity were reported in detail only by Seo et al. 21 according to the classification popularized by the International Study Group on Pancreatic Fistula (ISGPF). 78 In this study, there was a significant difference between LG and RG in terms of POPF (22.5% versus 10%). Particularly, LG patients had higher incidence of grade A (15% versus 7.5%), grade B (5% versus 2.5%), and grade C POPF (2.5% versus 0%) than RG patients.
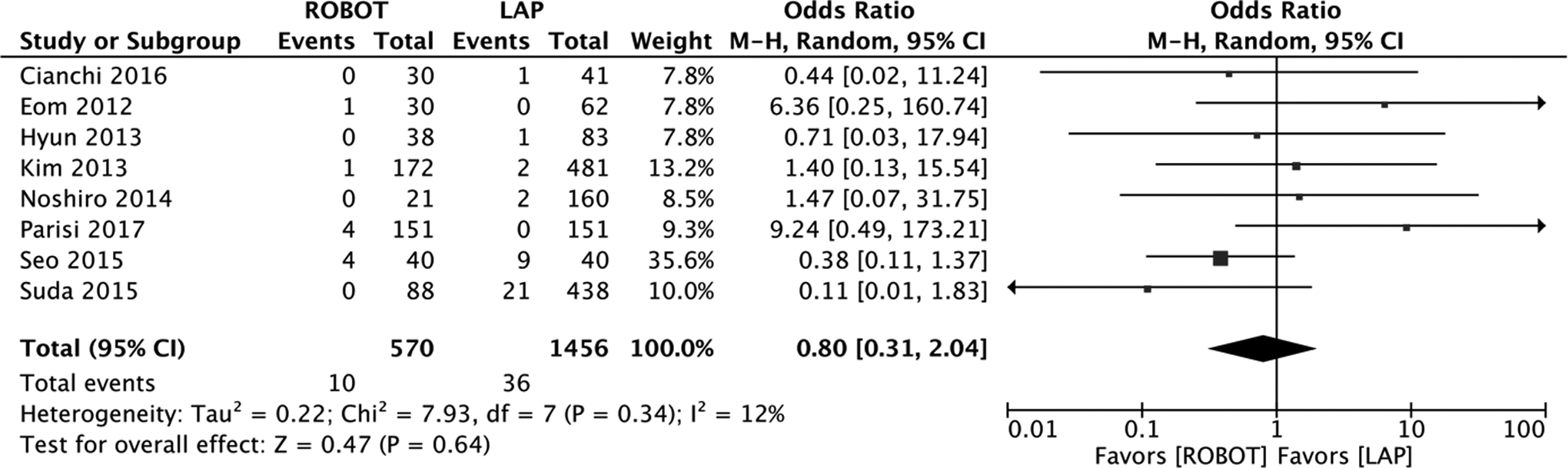
Postoperative pancreatic morbidity.
Regarding surgical procedure, RG required significantly longer surgeries than LG. Mean procedural time ranged between 206 and 439 minutes and between 167 and 361 minutes for RG and LG, respectively (MD of 59.44 [37.92, 80.96], Z = 5.41, P < .00001). Overall, mean length of hospital stay was between 6 and 15 days. The meta-analysis slightly favored RG over LG, although without statistical significance (MD −0.19 [−1.26, 0.87], Z = 0.36, P = .72). The mean amount of harvested lymph nodes ranged between 25 and 44, globally. There was a statistical difference favoring RG over LG, with an MD of 2.92 [0.32, 5.53], Z = 2.2, P = .03. Table 3 shows the main outcomes of interest from the included studies.
L, laparoscopic; POPF, postoperative pancreatic fistula; R, robotic.
Discussion
Pancreatic complications are quite uncommon but potentially devastating occurrences in the postoperative period of radical gastrectomy,1–4,18 although the true incidence of pancreas-related morbidity is likely difficult to quantify.3,6,74,75 In fact, the reported percentage of POPF and AP following gastrectomy varies significantly in the inherent literature, although such variability probably depends more on diagnostic accuracy rather than on surgical procedures or patient characteristics per se.3,5,6,19,74,75
We recently published the result of a systematic review with meta-analysis investigating the relative incidences of AP and POPF following radical gastrectomy. 3 Our analysis also focused on possible differences between conventional open and minimally invasive surgery. Overall, 20 articles comparing OG with MIG were included, covering a total of 7336 patients. The included articles consisted of 6 RCTs and 14 nonrandomized trials. The general rate of pancreatic morbidity was nearly 1%, ranging between 0.16% and 6.47% among studies. MIG had higher incidence than OG (0.91% versus 1.24%) with an OR of 1.6 and 1.39 at the analysis of solely RCTs and RCTs combined with nonrandomized analysis, respectively. AP occurred more frequently following MIG than OG (OR = 2.69) with statistical significance. Similarly, MIG had higher POPF rate than OG (OR = 1.13), although this difference was not statistically significant. Interestingly, among the 7336 patients we included in the meta-analysis, there were a total of 3753 MIGs. Of these, only less than 50 cases of robotic procedures were included from two reports.3,76,77
Surgical robots have been introduced in clinical practice to improve the handling of demanding procedures requiring fine dissections in narrow surgical spaces. As a consequence, robotic radical gastrectomy has been increasingly performed worldwide and its efficacy has been universally recognized in terms of both oncological and surgical outcomes.27–29,32,50,52,79,80 Actually, the use of the robot in radical gastrectomy is thought to be technically advantageous and it has been suggested that its application can be of some benefits in improving nodal dissection.3,21,43,64 In particular, increased dexterity in suprapancreatic dissection may avoid or limit unnecessary compression of the pancreas. 43 Actually, some evidence exists suggesting that the use of the robot may improve the outcomes of radical gastrectomy in terms of pancreas-related complications, especially in the setting of advanced disease.7,21,64 The importance of such data should be taken into account also considering two main factors: first, the occurrence of POPF has been associated with poorer long-term results following MIG 20 ; and second, dissection of the suprapancreatic area is of the utmost importance to improve long-term survivals in advanced gastric cancer.43,81,82
However, definitive conclusions on the possible merits of the robot cannot be drawn on the basis of the available literature, as few data come from single experiences.3,21,64 Accordingly, the aim of our analysis was to identify, summarize, and combine the published evidences comparing robotic and conventional laparoscopy on this specific focus. First, this meta-analysis revealed that some pancreatic complications can relevantly aggravate the postoperative course of MIG in more than 2% of patients. Notably, the overall incidence of POPF was 3.5%. Moreover, our review suggests that LG has a trend toward increased postoperative morbidity related to the pancreas, although without statistical significance (OR = 0.8, P = .6). It is interesting to note that RG patients, compared with those receiving LG, had higher BMI and more advanced disease. Moreover, the extent of the amount of harvested lymph nodes was significantly higher for RG than for LG. All these features have been indicated as specific risk factors for POPF following radical gastrectomy.3,5,18,75 Taken together, these factors strengthen the data elicited by the meta-analysis favoring the robot over laparoscopy on POPF.
Several mechanisms are thought to contribute to the onset of AP and POPF following radical gastrectomy and it is plausible that in most cases a wide spectrum of factors operate simultaneously.1–3 First, a number of different vascular injuries, including those due to postoperative inflammatory responses, may occur and result in compromised local blood supply.3,83 Second, it should be taken into account that some degree of direct manipulative trauma is produced by some specific maneuvers required during both the demolitive and the reconstructive phases of the intervention.3,84,85 Finally, the thermal damage produced by electric dissection near the pancreas may also play a crucial role. Actually, compared with conventional surgery, laparoscopic surgery generally requires a wider use of advanced energies such as ultrasonic-activated scalpels, which have been associated with a higher extent of thermal damage during peripancreatic lymphadenectomy.3,16 On the contrary, robotic technology is thought to allow radical gastrectomy to be performed with electrocautery devices alone.3,16,20,22
With regard to this, Noshiro et al. 22 published the results of a prospective, well-matched comparison between conventional laparoscopic and robotic distal gastrectomy for gastric cancer. The authors compared the two approaches on 181 consecutive surgeries, including 160 laparoscopic and 21 robotic procedures. Robotic procedures were carried out using only basic electrocautery instrumentation (i.e., monopolar and bipolar energies), while laparoscopic surgeries were performed with ultrasonic-activated devices. Robotic procedures were performed competently and showed greater amounts of harvested lymph nodes compared with laparoscopic procedures (44 ± 19 versus 40 ± 15), although without statistical significance (P = .29). Interestingly, the rate of POPF and the estimated blood losses of robotic surgery were smaller than those of laparoscopic surgery, although without statistical significance (P = .9 and P = .5, respectively).
Son et al. 62 investigated the results of more than a hundred minimally invasive spleen-preserving total gastrectomies with D2 lymphadenectomy and compared the mean number of retrieved and metastatic lymph nodes between robotic (51 patients) and laparoscopic (58 patients) procedures. These results come from a large-volume, referral center with large expertise in both gastric surgery and mini-invasive gastrectomy. The two groups did not differ in terms of preoperative data, including BMI, tumor stage, and previous surgery. Similarly, the complications experienced by the patients were comparable for laparoscopy and robotics. Overall, the mean number of lymph nodes retrieved with the robot was 47.2, compared with 42.8 of laparoscopy (P = .2). Notably, perigastric lymphadenectomy resulted in 30.8 and 26.6 lymph nodes for robotics and laparoscopy, respectively (P = .12). Interestingly, the volume of extraperigastric lymphadenectomy was significantly higher for the robot than for laparoscopy (15.9 versus 12.2, P = .02). In particular, the amount of retrieved lymph nodes favored with significance the robot in the case of stations 10 (splenic hilum) and 11 (splenic pedicle) and the suprapancreatic stations (7–12). Overall, the authors noticed no difference in the mean number of metastatic nodes between the two groups, with the exception of peripancreatic lymphadenectomy, in which the robot showed increased rate of metastatic disease than laparoscopy (0.4 versus 0; P = .04). Although neither overall survival nor disease free survival differed significantly between the two methods, the authors concluded that robotic total gastrectomy might be associated with more appropriate staging information and potential survival advantages.
Kim et al. 43 recently presented similar data comparing conventional laparoscopic with robotic distal gastrectomy in suprapancreatic nodal dissection for gastric cancer. The authors included a total of 272 patients who received radical gastrectomy with D2 dissection. Compared with standard laparoscopy, robotic surgery showed a significantly higher number of harvested lymph nodes in total (37.1 ± 12.9 versus 34.1 ± 12.1, P = .04) and specifically at extraperigastric area (16.3 ± 7.7 versus 3.2 ± 5.3, P = .001) and number 11 station (2.9 ± 2.9 versus 2.2 ± 2.0, P = .04).
This review has several limitations. First, a considerable amount of data, especially concerning RG, come from the initial experience of some centers. Thus, the effect of the procedure-specific learning curve may have influenced our findings. Second, the methods used to diagnose and define pancreatic complications were not clearly specified in the majority of studies. This implies a certain risk of bias due to diagnostic accuracy. In particular, the absence of a univocal method of classification based on clinical severity and management of AP/POPF precludes the possibility of a reliable analysis of the clinical importance of pancreatic morbidity. Finally, the limited methodological level of the included studies is to be acknowledged, as it may have influenced our findings. This is essentially due to the retrospective nature of most studies, the lack of randomized evidences, and the likelihood of a number of reporting biases within the primary reports.
Conclusions
Due to the lack of high-level evidence, definitive conclusions cannot be drawn on possible advantages of robotic over conventional LG with regard to pancreatic morbidity. However, in this review, RG shows a propensity for lower rates of postoperative pancreas-related events despite more unfavorable baseline characteristics compared with LG.
Footnotes
Disclosure Statement
The authors declare no conflict of interests pertaining to the present article. No grants or other sources of funding have been received for the drawing up of the present article. The article has not been submitted or under consideration elsewhere.