
Abstract
Abstract
Background:
Cardiac sympathetic denervation (CSD) is a surgical option for patients with life-threatening ventricular arrhythmias. Previously described cohorts included populations in which CSD was performed for primary and secondary prevention. We report the efficacy of CSD as adjunct therapy in children with medically refractory life-threatening arrhythmias.
Materials and Methods:
Retrospective review of patients undergoing thoracoscopic CSD at one institution between January 2008 and July 2017. Patient demographics, indications, procedural details, complications, length of stay, and effectiveness were evaluated.
Results:
Ten thoracoscopic CSD procedures were performed in 8 patients. Mean age was 8.2 years (8 days–19 years); mean weight was 32.6 kg (2.7–57 kg); and 50% were female. Four had long QT syndrome, 3 catecholaminergic polymorphic ventricular tachycardia, and 1 short QT syndrome. All patients had at least two (2 to >40) episodes of resuscitated ventricular arrhythmia and were maximized on medical therapy. Six patients had implantable cardioverter-defibrillators (ICD) with a mean of 11.9 appropriate discharges (1–40) before CSD. All patients underwent left CSD; 2 subsequently required right CSD. Four of the 6 ICD patients experienced dramatic improvement (total 48 ICD discharges pre-CSD; 3 post-CSD). Two patients noncompliant with medical therapy had no significant improvement (24 ICD discharges pre-CSD; 23 post-CSD) and also underwent right CSD, again with no improvement (23 discharges pre-right CSD; 28 post-right CSD).
Conclusions:
Thoracoscopic CSD can be safely performed in the neonate and pediatric populations. When utilized with medication therapy, CSD is an effective adjunct in reducing ICD discharges and arrhythmias.
Introduction
P
Left cardiac sympathetic denervation (CSD) for the treatment of LQTS was first described by Moss and McDonald in 1971, and the first report of a successful thoracoscopic approach was described nearly 30 years later.7,8 The advent of minimally invasive techniques in thoracic surgery has allowed this approach to become a relatively low-risk option for infants and children. The procedure often results in less postoperative discomfort and an earlier return to function compared to ICD placement. The risks of the CSD procedure are related to the partial resection of the stellate ganglion and are discussed with patients and families preoperatively. As realistic expectations can be set and the potential benefits often outweigh the risks, most families are interested in pursuing this surgical therapy.
Over the past 18 years, there have been several small case series—with less than 20 pediatric patients per series—describing the favorable outcomes of thoracoscopic left CSD.9–14 Most commonly, thoracoscopic left CSD has been performed for LQTS but also described for CPVT, idiopathic ventricular tachycardia/fibrillation, Jervell and Lange-Nielsen syndrome, left ventricular noncompaction, and a number of cardiomyopathies.9–14 Herein, we describe our single institution experience with left, as well as right, thoracoscopic CSD in 8 pediatric patients with life-threatening ventricular arrhythmias, including the youngest case reported in the literature who underwent the intervention at 8 days of life.
Materials and Methods
All patients who underwent thoracoscopic CSD were identified (using CPT code 32664) at a single pediatric tertiary care institution between January 2008 and July 2017. Retrospective review of the medical records detailed demographic data (age, gender), arrhythmia information (type, duration, previous treatment), surgical information (procedure time, technique), postoperative information (length of stay, complications), and procedural efficacy (improvement of arrhythmia, need for ongoing pharmacologic treatment, appropriate ICD discharges). Follow-up data were collected through October 15, 2017. Descriptive analysis was performed. Institutional Review Board approval was obtained.
Operative technique
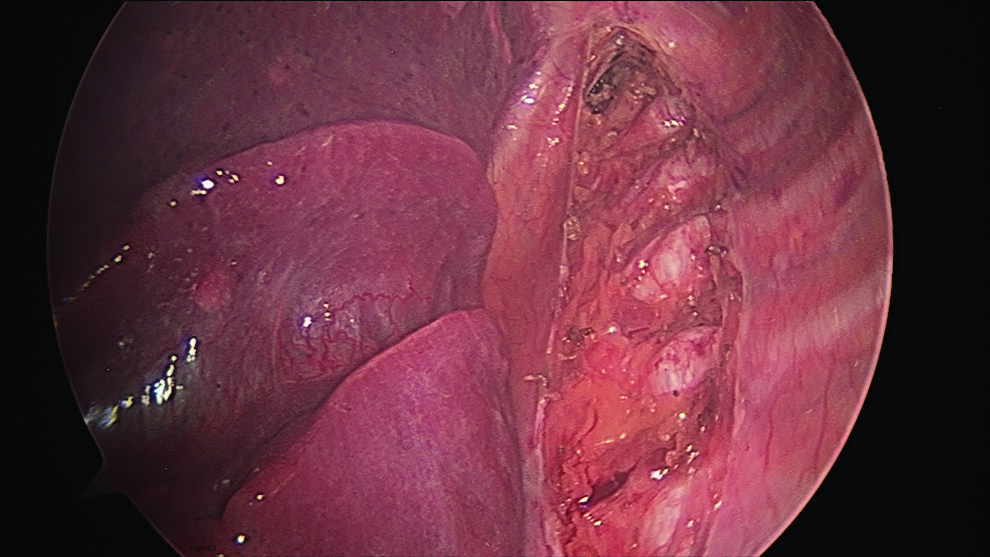
Patients were referred to pediatric surgery by their primary pediatric electrophysiologist and were seen on either a semiurgent outpatient basis or as an inpatient consult. Determination of appropriateness for intervention was made and an informed consent discussion was held with the families, including the known postoperative risk of unilateral partial ptosis or more severe symptoms of Horner's syndrome, including miosis and hemifacial anhidrosis. Pediatric cardiac anesthesiologists were involved in all cases with appropriate intraoperative monitoring and medications available to treat arrhythmias. ICDs were turned off during the procedures, and in some cases, defibrillator pads were placed. External defibrillator pad positioning was done with port placement in mind, and pads were excluded from the surgical field with plastic adhesive drapes. Patients were placed in a lateral decubitus position and access to the chest was obtained using a 5 mm port in the midaxillary line. Gentle insufflation of 5 mm Hg pressure limit and low flow rates were used for adequate visualization of the posterior chest (Fig. 1). Two additional ports were placed, one anteriorly and one posteriorly. The sympathetic chain was identified and the pleura was divided at the fifth rib space with electrocautery (Fig. 2). The nerve was identified, elevated, divided, and then caudal traction was applied to the nerve as the pleura was divided cranially to further expose the nerve. Branches at the inferior rib margins were divided using electrocautery (Fig. 3). Progress was made until the ganglion was encountered and more substantial branches at this level were divided (Fig. 4).
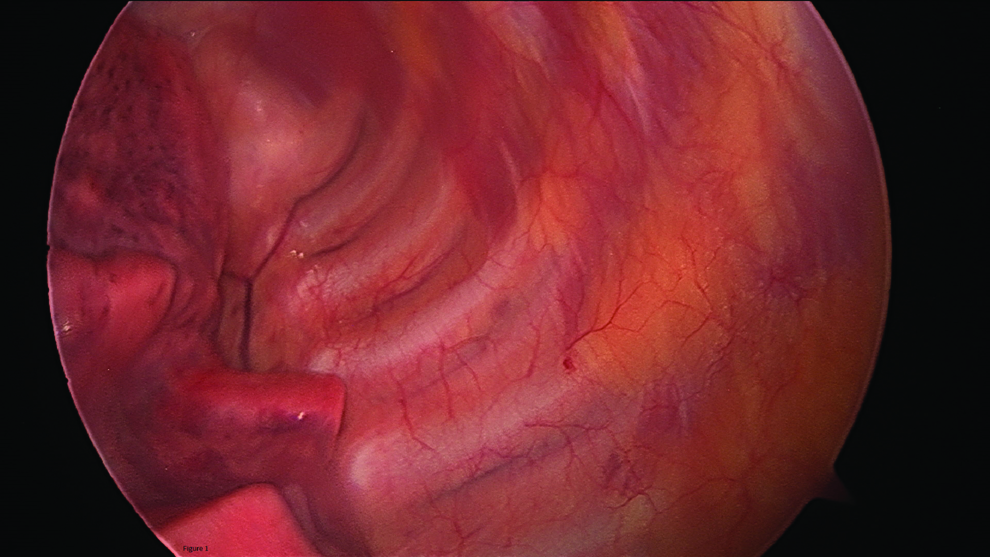
Insufflation of 5 mm Hg allows for adequate visualization of the posterior chest.
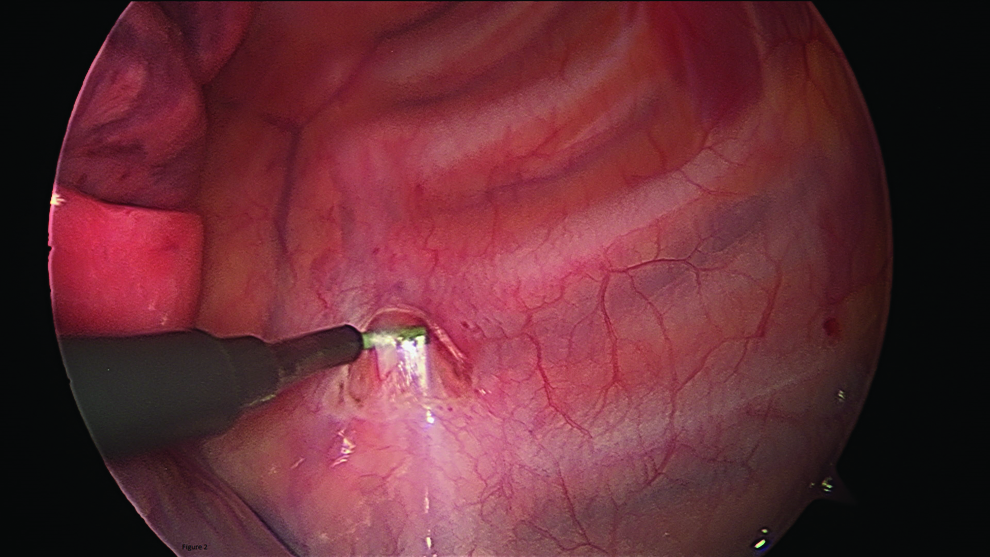
The sympathetic chain is identified, and the pleura is divided at the fifth rib space with electrocautery.
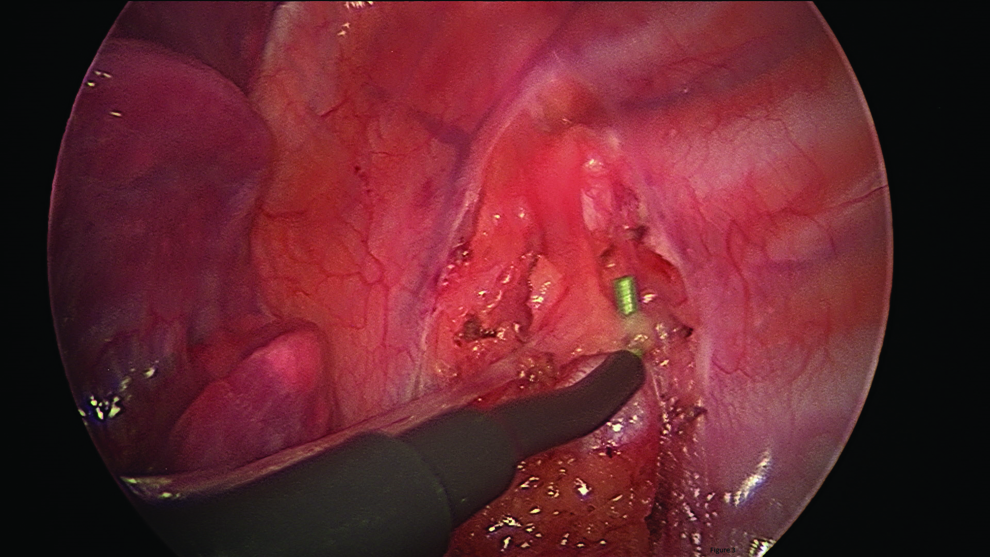
Nerve branches at the inferior rib margins are divided with electrocautery.

Dissection is continued until the stellate ganglion is exposed.
The stellate ganglion is the fusion of the inferior cervical ganglion with the first, and sometimes second, thoracic ganglion, and therefore, it can be variable in size and length. After the ganglion was fully visualized, it was transected with electrocautery, leaving 25% of the superior portion in place (Fig. 5). Vascular structures are avoided if dissection is limited to the area just around the nerve chain and ganglion. Hemostasis was confirmed and an 8.5 French pigtail catheter was inserted. Rib blocks were performed with 0.25% Marcaine. Ports were removed and incision sites were closed with absorbable suture. The thoracostomy tube was placed to suction for 12 hours and then placed to water seal and removed, if there was no evidence of air leak or pneumothorax. Patients were given a regular diet and maintained on analgesic medications for 1–2 days.
The stellate ganglion is transected with electrocautery leaving 25% of the superior portion of the ganglion in place.
Results
A total of 10 thoracoscopic CSD procedures were performed in 8 patients (8 left-sided and 2 right-sided). Patient demographics and ICD shock rates are shown in Table 1. Mean age at time of surgery was 8.2 years (8 days–19 years), mean weight was 32.6 kg (2.7–57 kg), and 50% were female. All patients were on maximized medical therapy before CSD (mean number of antiarrhythmic medications 1.5) and had at least 2 (2 to >40) previously documented episodes of resuscitated ventricular arrhythmia. Six patients had undergone ICD placement with a mean of 11.9 appropriate discharges (1–40) before CSD.
CSD, cardiac sympathetic denervation; LCSD, left cardiac sympathetic denervation; RCSD, right cardiac sympathetic denervation; ICD, implantable cardioverter-defibrillator; LQTS, long QT syndrome; CPVT, catecholaminergic polymorphic ventricular tachycardia.
Six surgeons performed the procedures, and 1 surgeon (K.V.L.) was present for 9 of the 10 procedures. Pediatric cardiac anesthesiologists were involved in all 10 cases. Procedures were able to be scheduled on an elective basis 50% of the time. The remaining cases were done while the patients were already inpatient (admitted due to symptoms or complications from arrhythmia). Mean procedure duration was 52 minutes (40–66 minutes). Three 5 mm ports were utilized for each procedure, with the exception of the neonate for whom 3 mm ports were used. In all cases, 75% of the lower portion of the stellate ganglion was resected. There were no intraoperative complications, no conversions to open, and no intraoperative arrhythmias. Blood loss was minimal in all cases.
All patients initially underwent left-sided CSD, with 2 patients subsequently undergoing right-sided CSD. Four of the 6 patients with ICDs experienced dramatic improvement following CSD (total 48 ICD discharges pre-CSD; 3 post-CSD). Two patients had no significant long-term improvement following left CSD (24 ICD discharges pre-CSD; 23 post-CSD) and subsequently underwent right CSD, again with no long-term improvement (23 discharges pre-right CSD; 28 post-right CSD). These 2 patients were noncompliant with medications.
Both patients without an ICD underwent elective pacemaker placement at the time of CSD to facilitate maximum beta-blocker therapy. An 8-day-old female with LQTS and intractable torsades de pointes experienced no further arrhythmias following CSD; she was managed with dual-chamber pacing and propranolol alone until undergoing elective upgrade to an ICD at 4 years of age. An 8-year-old male remains atrially paced without an ICD 4 years post-CSD.
Median length of postoperative stay was 1 day (1–19 days). The neonatal patient remained in the neonatal intensive care unit for 19 days postoperatively and when excluded from the cohort, median length of stay was 1 day (1–4 days). One patient experienced transient mild ptosis. One patient, performed early in the cohort when pigtail catheters were not routinely placed intraoperatively, had a small postoperative pneumothorax that did not require chest tube placement. The neonatal patient continues to have anisocoria, mild ptosis, and intermittent Harlequin syndrome 5 years postprocedure. Mean follow-up for the cohort was 47 months (2.5–98 months).
Discussion
Initially used as a therapy for intractable angina as early as 1916, left CSD was not widely utilized for its antiarrhythmic effects until 1971.7,15 Experimental and clinical evidence demonstrated that left CSD resulted in both a direct shortening of the QTc and an increase in the ventricular fibrillation threshold leading to its adoption as a potential treatment modality for patients with LQTS.16,17 The utility of left CSD has subsequently been shown in patients with CPVT and has been suggested as a treatment option for patients with ischemic or dilated cardiomyopathies, arrhythmogenic right ventricular cardiomyopathy, left ventricular noncompaction, or indeed any patient with recurrent ventricular fibrillation regardless of the etiology.13,18
The approach to sympathectomy has anatomic significance influencing the portion and amount of stellate ganglion resected resulting in a spectrum of side effects. The open cervical approach with complete destruction of the stellate ganglion will not only have the desired effect of CSD but also the full spectrum of Horner's syndrome, if the superior portion of the stellate ganglion is taken. Using a minimally invasive technique that approaches the ganglion from the inferior direction within the thorax enables sparing of the superior most portion of the ganglion thereby minimizing the postoperative side effects. The size of the ganglion at the time of resection will play an obvious role in the likelihood of developing Horner's syndrome. In our series, the only patient to experience ongoing anisocoria, intermittent ptosis, and Harlequin syndrome weighed 2.7 kg at the time of the procedure.
Our technique differed slightly from that described in other publications.11,14,17 We do not use right main stem intubation as we do not find it necessary for visualization of the posterior thorax and the sympathetic chain. We do not apply lidocaine solution to the ganglion, and we have not experienced episodes of intraoperative ectopy. We use electrocautery to divide the ganglion while other authors report using a harmonic scalpel or sharp dissection with scissors. The amount of ganglion left behind also differs among institutions and in series where the ganglion is intentionally spared, the effect on prevention of arrhythmias was decreased. 14 Placement of a chest tube for evacuation of residual pneumothorax, postoperative detection of lung injury, or unexpected bleeding is a practice that is not used in some series. Evacuation of the pleural carbon dioxide at the conclusion of the procedure, in the absence of any significant bleeding, may be adequate and preclude the need for chest tube placement. This may decrease postoperative pain, lessen the need for additional imaging required to remove the chest tube, and decrease the already short length of stay.
The role of thoracoscopic left CSD for the treatment of ventricular arrhythmias in the pediatric population has been limited to case reports and relatively small, single-institution case series.9–14 Almost universally, these reports have demonstrated a benefit of left CSD by reducing the incidences of either syncope or ICD discharges in patients previously demonstrated to be at risk. A similar degree of success in reducing the incidence of life-threatening events was demonstrated in our small case series. Just as importantly, however, are the potential limitations of this intervention implied by the 2 nonresponders in our series.
While the majority of patients undergoing thoracoscopic CSD at our institution experienced a dramatic reduction in the incidence of life-threatening events following left CSD, 2 of 8 individuals actually experienced a higher number of ICD discharges following left CSD. Although nonresponse to left CSD is not without precedent, several potential explanations exist for this observation in our data. Traditionally, left CSD has not been used as a primary arrhythmia management tool at our institution, and only patients who have failed maximum medical therapy are referred for left CSD. This approach implies a selection bias in the treatment group, as only patients with particularly aggressive disease undergo left CSD. Both of the nonresponsive patients in our cohort (1 with LQTS, 1 with CPVT) enjoyed a period of relative improvement immediately after the left CSD before again developing an increased arrhythmia burden months later. Both were then referred for right CSD, and again, both enjoyed an arrhythmia-free period following the right CSD procedure before a second relapse. Later it was revealed that neither patient was compliant with medication therapy before the left CSD. Both were medically compliant immediately after left CSD only to again lapse into noncompliance—prompting a right CSD. This pattern of brief medication compliance followed by a lapse and subsequent increase in ICD discharges repeated itself following right CSD in both patients. It was only well after both of the procedures that this cycle of noncompliance was revealed, and both are now relatively arrhythmia-free on maximum medication therapy. This observation would suggest that left CSD by itself may not provide adequate protection in particularly at risk individuals, and the continued use of an aggressive antiarrhythmic regimen may still be required in apparent nonresponders.
Also of potential significance is the fact that neither of these patients experienced a significant improvement following right CSD. Both clinical and experimental data have, respectively, demonstrated an improvement in the arrhythmia burden and an increase in the ventricular fibrillation threshold following left CSD. Data regarding the usefulness of right CSD are mixed, however. Work performed by Schwartz et al. demonstrated that acute complete inhibition of the right stellate ganglion input in a canine model resulted in a lowering of the ventricular fibrillation threshold. 19 Clinical improvement in arrhythmia burden following right CSD has been limited to scattered case reports, with subjects either undergoing bilateral sympathectomy as first line therapy or right CSD only after an apparent suboptimal response to left CSD.20,21 In our small series, completion of a right CSD after apparent nonresponse to left CSD did not appear to offer additional benefit, but this was in the context of noncompliance with medication therapy.
To our knowledge, the current series includes the youngest and smallest patient (8 days, 2.7 kg) to undergo a thoracoscopic CSD. The patient, who later was found to have a de novo KCNH2 mutation, had a QTc of 588 ms with resultant 2:1 atrioventricular conduction, and experienced numerous episodes of ventricular tachycardia degenerating into ventricular fibrillation during the first week of life (Fig. 6). Owing to the challenges of ICD placement in a <3 kg infant, a strategy of left CSD, dual chamber pacing, and aggressive beta blockade (4–5 mg/kg/day of propranolol) was instituted. Following this intervention, the patient experienced no further ventricular arrhythmias. She was electively upgraded to an ICD at 4 years of age (when her pacemaker reached elective replacement indices), and remains arrhythmia-free to this day.

Electrogram of an 8-day-old, 2.7 kg infant with prolonged QT interval (588 ms) and resultant 2:1 atrioventricular conduction deteriorating into ventricular fibrillation.
Also included in this series is the first report of left CSD utilization for the treatment of a patient with short QT syndrome. This patient had perhaps the most dramatic improvement in the cohort, experiencing 40 appropriate ICD discharges in the 12 months before left CSD and only 1 in the 8 months since the procedure. This significant decrease in arrhythmia burden supports the proposed notion that left CSD may be an effective therapeutic modality across a broad spectrum of disease. 13
Limitations
Limitations to our study include the retrospective nature as well as the small number of patients. As noted, patient selection was also a potential limitation as only those in whom maximum medical therapy had failed were referred for the procedure, and thus the effect of left CSD on less severe cases and its efficacy as a tool for primary prevention cannot be assessed. A total of 6 surgeons were involved in these 10 cases, potentially introducing slight variation in technique. However, a single surgeon being involved in 9 of the 10 cases likely mitigated this effect.
Conclusion
Thoracoscopic CSD is an effective tool in the management of pediatric patients who have survived an acute life-threatening arrhythmia. The procedure can be performed safely in neonates and children and can be helpful for patients in whom ICD placement may not be feasible. In particularly high-risk individuals, however, it is unlikely to supplant the need for ongoing aggressive antiarrhythmic therapy.
Footnotes
Disclosure Statement
No competing financial interests exist.