
Abstract
Abstract
Aims of the Study:
To assess the short-term clinical outcome of the novel Shehata technique of laparoscopic traction—lengthening for abdominal testes in a single center over a 12-month period (January–December 2014). An ethics approval of the study and appropriate consents were obtained for all patients before inclusion in our study.
Materials and Methods:
A total of 47 consecutive boys presented with impalpable testes in the ipsilateral hemiscrota, 3 of them were bilateral summing up to a total of 50 U of impalpable testes to a single center over 12 months (January–December 2014). Those boys underwent a preoperative ultrasound (US) Doppler scan for the ipsilateral and contralateral testes. They then proceeded to a first-stage laparoscopic exploration for the testes in which the cranial testicular artery and the caudal vas deferens were traced to their meeting point to locate the abdominal testes that were either found (peeping at the internal inguinal ring [IIR] or more cranially) or otherwise vanishing (intraabdominally blind-ending vas and vessels or extra-abdominally passing through the IIR). All 50 testes failed to stay at the contralateral IIR when brought there mandating a preliminary lengthening of the testicular vessels by lateral dissection, traction, and fixation to a point 1–2 cm superolateral to the contralateral anterior superior iliac spine (ASIS), essentially a mobile traction point. After 12 weeks, all underwent a second-stage laparoscopic-assisted ipsilateral subdartos orchidopexy for the testes under traction. Occasional slippage of the testis under traction mandated an otherwise second-stage retraction and a third-stage orchidopexy. All underwent US Doppler scan 3 and 6 months after orchidopexy.
Results:
The 47 cryptorchid boys presented at a mean age of 3 years 2 months (range: 6 months–8 years). Out of the 50 impalpable testes, 9 were nonvisualized on preoperative US Doppler scan and 16 were vanishing on laparoscopic exploration: 5 abdominally (in utero vascular accident) and 11 scrotally (perinatal torsion). The remaining 34 testes were fixed loosely near the contralateral ASIS in the first-stage laparoscopic exploration. Out of which, 3 had slipped traction at the second stage. The 12-week traction interval went uneventfully and a predefinitive US Doppler scan confirmed viability of all testes under traction. All 34 elongated testes were mobilized and fixed in the ipsilateral hemiscrota inside a created subdartos pouch (of de Netto). All 34 fixed testes were confirmed viable on US Doppler scan 1, 3, and 6 months after orchidopexy.
Conclusion:
The novel Shehata technique of staged laparoscopic traction-lengthening for abdominal testes is safe, easy, and convenient as evidenced by our limited early experience. Neither internal herniation complicated the traction period nor testicular atrophy (by undue tension) complicated the traction or follow-up periods. We believe it is a good alternative to the Fowler–Stephens staged orchidopexy that entails risky division of the testicular vessels.
Introduction
Cryptorchidism is one of the most common genitourinary disorders in boys. The original birth prevalence of 3% in full-term (versus 30% in premature) male neonates, decreases later on in life to 1% in boys 6 months to 1 year old. Familial clustering is a well-known demographic feature of this disease. 1 Testicular descent occurs in 2 phases: transabdominal and inguinoscrotal. Transabdominal descent by differential growth of the vertebrae and pelvis is more significant in the first half of gestation, whereas inguinoscrotal descent requires an intact gubernaculum and processus vaginalis later in gestation. This is mediated by a sound hypothalamic–pituitary–gonadal axis and by sufficient active dihydrotestosterone. Etiology is usually a multifactorial mixture of global hormonal (Mullerian inhibiting substance, prenatal estrogen exposure, and descendin) and local mechanical factors (gubernacular insufficiency, genitofemoral nerve, and calcitonin gene-related peptide). 2
Clinical examination is paramount in the assessment of cryptorchidism. Testes are either palpable (70%–80%) or nonpalpable (20%–30%). Palpable testes could be retractile, ectopic, or truly undescended at the scrotal neck. Nonpalpable testes could be vanishing, canalicular, or truly intraabdominal. Associated anomalies include patent processus vaginalis, epididymo-vasal anomalies, hypospadias, Wilms' tumor, and abdominal wall defects. 3
Besides laboratory work-up that is needed for associated anomalies, imaging studies for testicular localization are of limited value. Among which, Doppler ultrasound (US) scanning is currently the most popular, despite its low accuracy and its operator-dependent nature, probably due to its availability, low cost, and noninvasiveness. 4 On the other hand, computed tomography scanning involves high-dose radiation exposure and magnetic resonance angiography is expensive and requires sedation or anesthesia although claimed to be almost 100% accurate. Abdominal laparoscopy, therefore, remains to be the diagnostic (and therapeutic) tool of choice whenever available, owing to its high accuracy and being minimally invasive. 2
Current recommendation still remains to start treatment around 3 to 6 months of age with the concept of giving enough chance for testes to descend spontaneously and the probability of damaging testicular vessels working together pushing that age up against theoretically improving the chances for future fertility bringing that age down. 5
Current treatment options for abdominal testes include laparoscopic Fowler–Stephens orchidopexy and testicular microvascular autotransplantation, both achieved disappointing and suboptimal outcomes: 67% for standard and 77% for staged Fowler–Stephens orchidopexy 6 versus 84% for microvascular orchidopexy. 7 In his landmark article, Shehata 8 has proposed a new staged laparoscopic-assisted gradual traction on abdominal testes to lengthen the testicular vessels facilitating scrotal orchidopexy with promising initial results and minimal complications. We, therefore, felt encouraged to attempt laparoscopic testicular traction to stimulate the testicular vessels to grow allowing scrotal orchidopexy in a staged fashion.
Materials and Methods
A total of 47 consecutive boys presented with impalpable testes in the ipsilateral hemiscrota, 3 of whom were bilateral summing up to a total of 50 U of impalpable testes over 12 months (January–December 2014) to School Children's Hospital, Health Insurance Authority (HIA), Alexandria, Egypt.
All cryptorchid boys underwent a preoperative laboratory work-up, including Complete Blood Picture, Bleeding and Partial Thromboplastin times, as well as US Doppler scan for the ipsilateral and contralateral testes. Regardless of the US report, all still proceeded to a first-stage laparoscopic exploration.
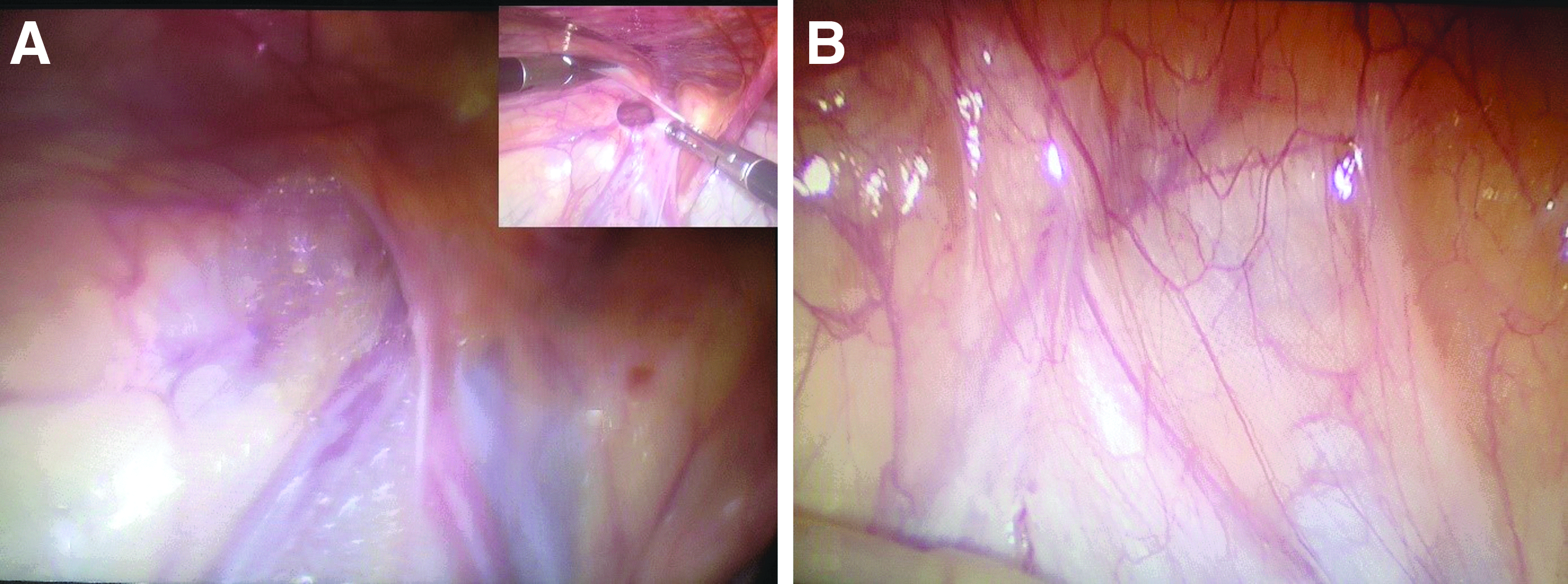
A. First-stage laparoscopic exploration was planned in an elective fashion. A preoperative preparation with Bisacodyl suppositories (5 mg) was done the night before. Under general inhalational anesthesia, a urinary catheter was placed to evacuate the urinary bladder. An insufflating 5-mm safety trocar was inserted transumbilically using the open Hasson method for CO2 insufflation at pressures ranging from 8 to 12 mmHg suitable for the patient's age. After achieving sufficient pneumoperitoneum, a 5-mm telescope 0° or 30° was inserted from the same umbilical trocar. The patient is routinely positioned in Trendelenburg position with elevation of the ipsilateral side of the operating table up to move the bowel loops away from the ipsilateral internal inguinal ring (IIR) facilitating exploration of the ipsilateral testis. Another two 5-mm ports were routinely inserted 1–2 inches lateral to the umbilical port for ergonomically suitable angulation toward the ipsilateral IIR. The cranial retroperitoneal testicular artery and the caudal retrobladder vas deferens were traced to their meeting point to locate the abdominal testis. This exploration usually resulted in two alternative findings:
1. Both vas and vessels passing through the IIR (Fig. 1A). Then laparoscopic exploration is terminated, and a conventional open inguinal canal exploration was performed for a presumably atrophic testicular nubbin that was excised if found.
2. Both vas and vessels meeting intraabdominally:
i. A “blind-ending vessels” (Fig. 1B) was considered the endpoint of exploration where a diagnosis of a vanishing testis is made.
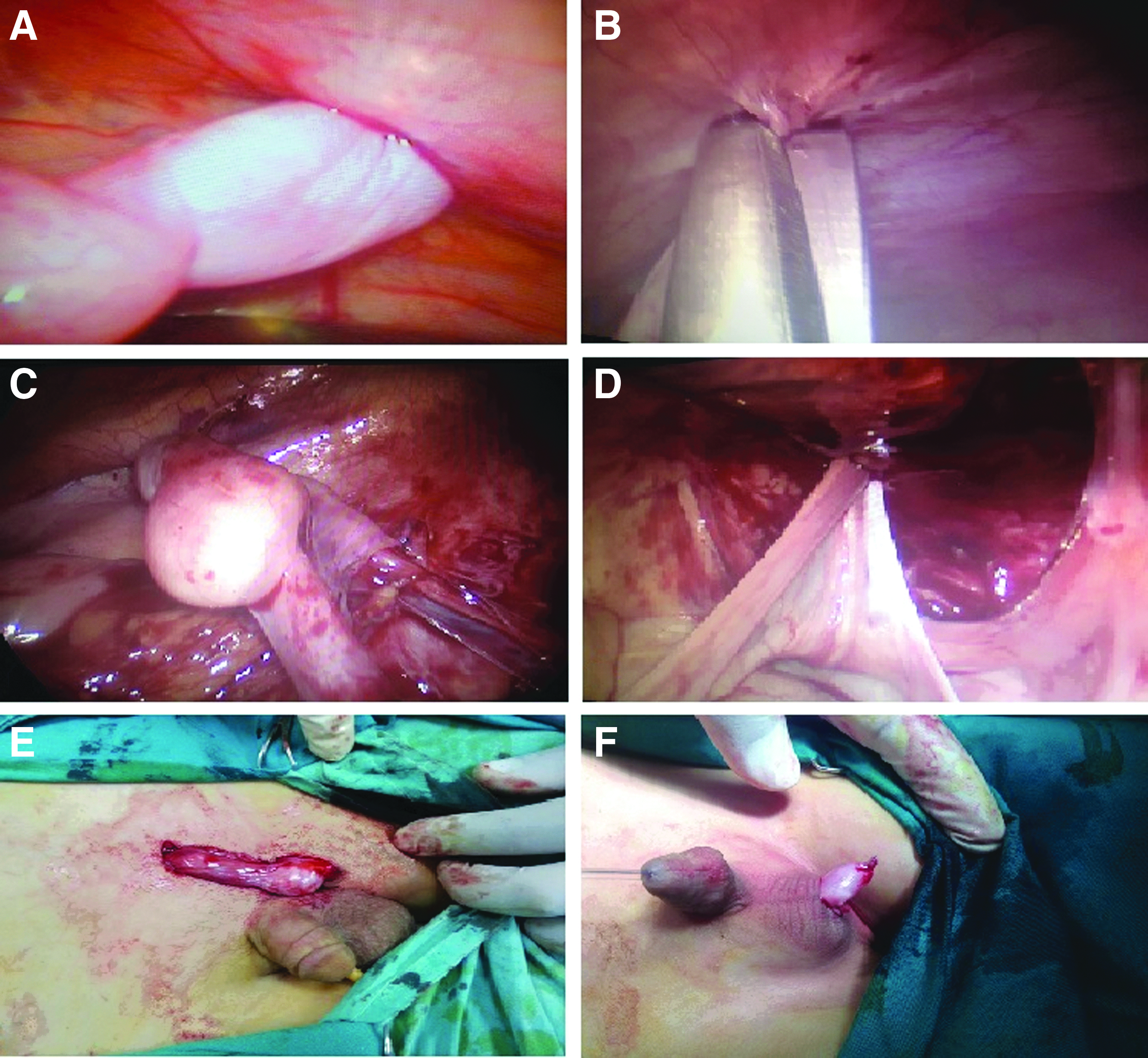
ii. If otherwise both the vas and vessels terminate in a visible testis (Fig. 2A) at variable distance from IIR (peeping or more proximally). Then, a contralateral fenestrated grasper (Yohan) was used to move the testis away from the IIR to pull any possible long-looping vas out of IIR (Fig. 2B) allowing an ipsilateral low-power monopolar hook diathermy to dissect the testis off its abnormal gubernaculum (Fig. 2C). The testis is placed at the contralateral IIR and left there:
If it stayed there, then its vas and vessels had sufficient length amenable for one-stage laparoscopic-assisted orchidopexy.
If it recoils back, then its vas and vessels are short enough mandating preliminary traction to lengthen the testicular vessels. We started freeing the testis by dissection of the lateral peritoneum using low-power monopolar hook diathermy. Then the testis is fixed to a point within 1 cm from the contralateral anterior superior iliac spine (ASIS), essentially a mobile traction point, as follows: at first a small 1–2 cm incision is made anteromedial parallel to the contralateral ASIS. Then, a 2/0 Ethibond on a round needle is passed through the abdominal muscle, received inside the abdomen under laparoscopic vision by a 5-mm needle holder to pierce the tunica albuginea of the testis (Fig. 2D) and then grasped by a port-closing instrument to be (Fig. 2E) returned through the abdominal wall at the same incision to be tied loosely outside so the testis was subjected to minimal tension inside the abdominal cavity and not even touching the abdominal wall (Fig. 2F) thus avoiding undue tension. This traction stitch is later buried under the skin when the wound is closed.
The procedure is then terminated, abdomen deflated, ports removed, and wounds closed surgically. The boys were discharged on the same or next days after regaining normal bowel motions and tolerating oral feeding.
1. If the stitch slipped, the testis lost traction and was found floating near the ipsilateral IIR. Then a retraction stitch is placed like the first stage and left for another 12 weeks of traction period.
2. If the testis sustained traction, the testis is found sagging inside the abdominal cavity (Fig. 3A). Then the stitch is cut by a 5-cm scissors (Fig. 3B) releasing the testis off the abdominal wall (Fig. 3C) and then passed either through the ipsilateral IIR or better through the abdominal wall medial to medial umbilical ligament (Fig. 3D) opposite the external inguinal ring above the pubic tubercle to appear in the superficial inguinal pouch (Fig. 3E), where it is fixed in a created subdartos pouch as described by de Netto (Fig. 3F).
D.
First-stage laparoscopic exploration for intraabdominal testis.

First-stage laparoscopic traction of intraabdominal testis.
Second-stage laparoscopic-assisted orchidopexy.
Results
A total of 47 cryptorchid boys presented to Alexandria School Children's Hospital (Sporting), HIA, Alexandria, Egypt with impalpable testes, 3 of which were bilateral making a total of 50 U of impalpable testes, 36 right (72%) and 14 left (28%) (Table 1 and Fig. 4). Boys were 6 months–8 years of age with a mean of 3 years 2 months. All were confirmed impalpable by clinical examination and accordingly underwent a routine preoperative US Doppler examination that revealed 9 nonvisualized testes (18%) and the remaining 41 testes (82%) were visualized within the inguinal canal or at varying distances from the ipsilateral IIR. Regardless of the clinical and US scan results, all underwent a laparoscopic exploration for the testis in question.
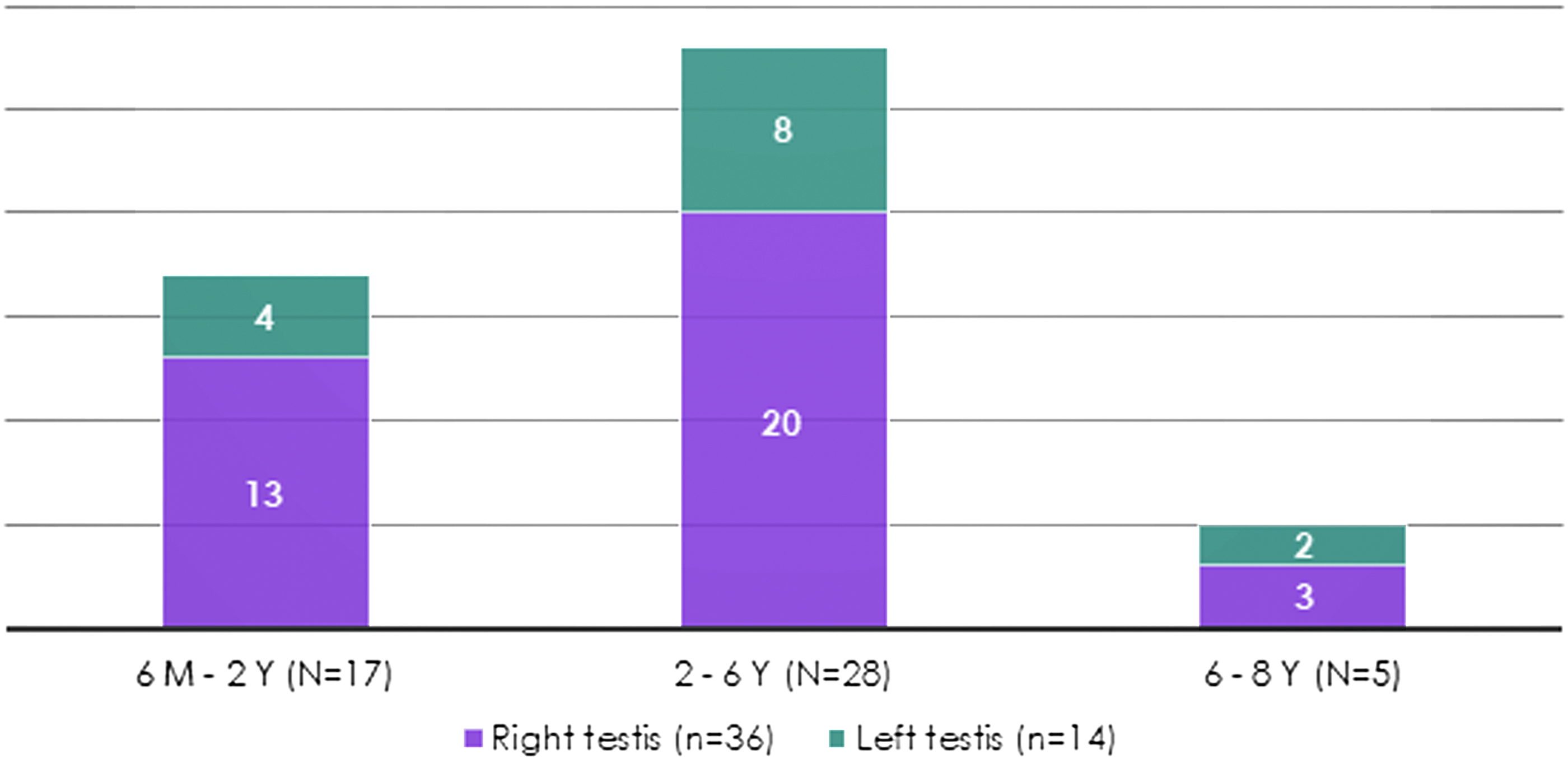
Age distribution by side (n = 50).
Age Distribution by Side
On laparoscopic exploration, the vas deferens and testicular vessels were found blind ending in 5 testis units (10%) probably due to an in utero vascular accident, while they were found passing through the ipsilateral IIR in another 11 U (22%) that were found to end in an atrophic nubbin on concurrent inguinoscrotal exploration confirming the diagnosis of vanishing testes (probably due to perinatal torsion).
Out of the remaining 34 testes (68%), only 3 (9%) were found peeping from the ipsilateral IIR and the remaining 31 (91%) were found at various distances ranging from 1 to 4 cm from the ipsilateral IIR and classified accordingly into two groups: low lying (1–2 cm from IIR) and high lying (3–4 cm from IIR) (Table 2 and Fig. 5).
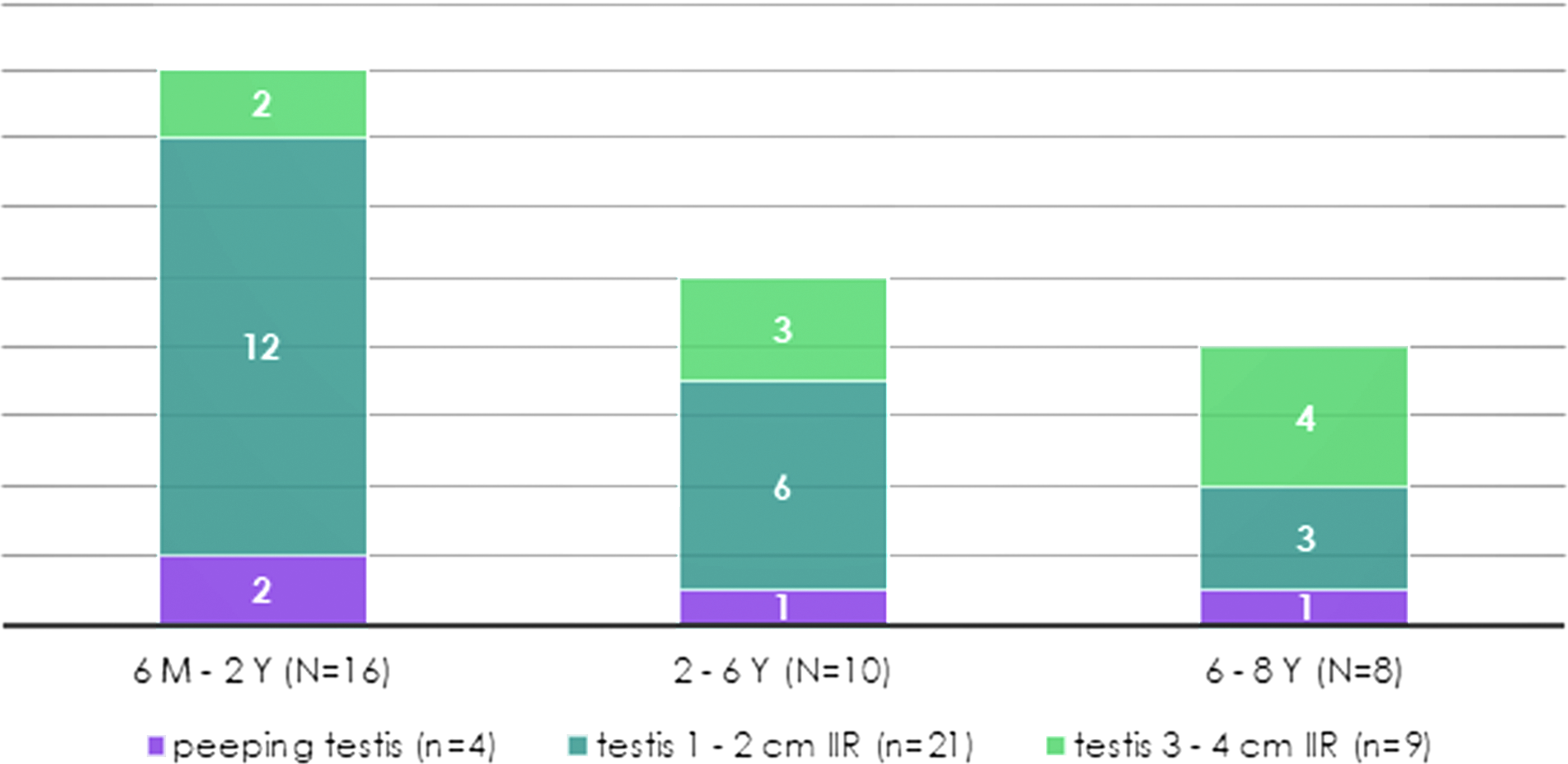
Age distribution by distance from IIR (n = 34). IIR, internal inguinal ring.
Age Distribution by Distance from Internal Inguinal Ring
Regardless of the position of the testicular units, all were dissected off their lateral peritoneum as well as the distal gubernaculum and all failed to stay at the contralateral IIR (measuring test), mandating a preliminary traction to the abdominal wall 1-inch anterosuperior to the contralateral ASIS for a 12-week interval. The 12-week traction interval passed uneventfully without any complications, like internal herniation of the small bowel or adhesive intestinal obstruction. At the end of the traction interval, the predefinitive follow-up US Doppler scan confirmed the viability of all 34 testes under traction (100%) with slippage of the traction stitch in 3 (9%) of the older boys.
Regardless of the US findings, all boys proceeded to the (definitive) second-stage laparoscopic exploration that confirmed the viability in all 34 testes (100%) and slippage of the traction stitch in 5 testes (15%) of the older boys who subsequently underwent retraction. All otherwise 29 elongated testes (85%) were mobilized and passed through the respective IIR to be fixed in the ipsilateral hemiscrotum inside a created subdartos pouch (of de Netto). All 34 (100%) fixed testes were confirmed viable on US Doppler scan 1, 3, and 6 months after orchidopexy, with evidence of punctate calcification only in 2 testes (6%) of the older boys (Fig. 6).
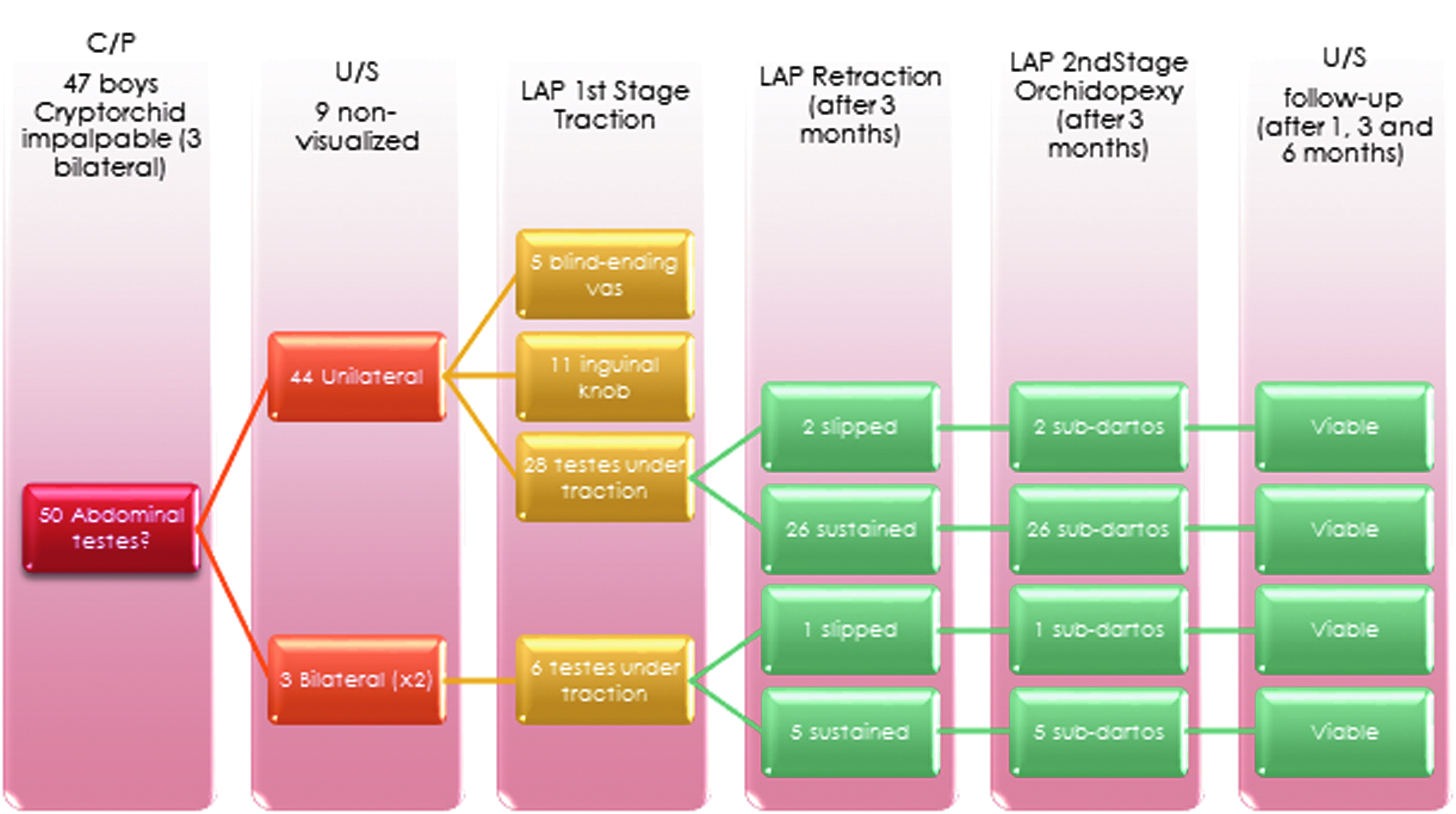
Flowchart of patients.
Discussion
Although been recognized over a century ago, the abdominal testis remains to be a major challenge to pediatric surgeons as a surgical paradigm. Although many surgical procedures have been described to address this problem, yet none has achieved supremacy in the clinical paradigm. The absence of a worldwide consensus on a management protocol not only emerges from lack of an ideal surgical technique nor imaging tools, but also from incomplete understanding of the interplay of genetic, physiological, and hormonal mechanisms involved in testicular descent.1–3,9
Intraabdominal testes have been traditionally divided into low lying (within 2 cm from IIR) and high lying (over 3 cm from IIR). For the low-lying testes, a conventional one-stage open orchidopexy has been practiced for ages with marginal results until laparoscopy has been established as an efficient diagnostic and surgical tool in the management of abdominal testes, especially using the Prentiss maneuver achieving excellent results. 5
On the other hand, the high-lying testis is more controversial as regards the ideal management protocol. Fowler–Stephens staged orchidopexy has dominated the surgical techniques for decades but with only suboptimal results. Alternatively, testicular microvascular autotransplantation is tedious, time consuming, and requires special experience and equipment making it less feasible and far from becoming a worldwide standard. 5
Traction to achieve organ growth or stretch has been an interesting surgical concept employed originally by orthopedic surgeons to lengthen short bones by distraction and later by general surgeons to lengthen esophagus after resections. Keetley and Torek have separately proposed techniques to lengthen the short spermatic vessels for abdominal testes based on traction by fixation to the thigh. However, those techniques and many others were quickly abandoned after achieving disappointing results losing many testes probably because of the sudden and uncontrolled tension on the testicular vessels. 10
Recently, Shehata has reintroduced the concept of traction in the management of high intraabdominal testes. In his landmark article, he proposed a new staged laparoscopic-assisted technique for bringing down the abdominal testis with minimal complications and maintaining their viability. 8
We report on 47 cryptorchid boys with 50 impalpable testes who underwent a preoperative US Doppler scan that failed to locate 5 truly intraabdominal testes and falsely located 12 other vanishing testes. In our series, US was 85% sensitive and 25% specific locating the intraabdominal testis with a positive predictive value of 71% and a negative predictive value of 44% (Table 3). Overall, US accuracy was 66%, being highly operator dependent and technology variable, was far less accurate than reported by Onkar et al. 88%, 11 yet similar to that reported by Budianto et al. 4
Ultrasound Accuracy Locating Intraabdominal Testes
US, ultrasound.
In our series, regardless of US findings, all 34 testes confirmed intraabdominal at laparoscopic exploration underwent laparoscopic-assisted traction to the contralateral ASIS for a minimum of 12 weeks to lengthen the testicular vessels to facilitate the second-stage laparoscopic-assisted subdartos orchidopexy of the viable testes. Neither internal herniation complicated the traction period nor testicular atrophy (by undue tension) complicated the traction or follow-up periods. However, two older complications were encountered. Occasional slippage of 3 out of 34 testes under traction (9%) in the older boys who then underwent laparoscopic retraction at the second stage and fusion of both testes concurrently put in traction in 1 patient with bilateral intraabdominal testes. This highlights the special difficulty managing those two specific subgroups of patients: older children and bilateral cases. Even Shehata et al. 12 reported a higher success rate (>90%) for traction in younger boys (<2 years-old) that drops to only 64% for older boys (>6 years-old) even recommending Fowler–Stephens vessel transection in favor of traction for high-lying testes (>4 cm from IIR). This may be due to the fact that older boys had higher intraabdominal testes rather than age itself as an independent factor. We believe that cases of bilateral intraabdominal testes, older boys (>2 years-old), and high-lying abdominal testes (>2 cm from IIR), pose a special challenge to the pediatric surgeon and need to be addressed differently. We, therefore, should study traction on such subsets of patients separately.
Conclusion
The technique of staged laparoscopic traction lengthening for abdominal testes is safe, easy, and convenient as evidenced by our limited early experience. Neither internal herniation nor testicular atrophy complicated the traction or follow-up periods. We believe it is a good alternative to Fowler-Stephens transection of testicular vessels.
Footnotes
Acknowledgment
The authors are grateful to Prof. Sameh Shehata, MD, Professor of Pediatric Surgery, Alexandria University, Egypt, the originator of this technique, for his support and guidance and constructive criticism throughout this study.
Disclosure Statement
No competing financial interests exist.