
Abstract
Abstract
Background:
Hemorrhage during Nuss bar removal is an uncommon but feared complication that can be life threatening if not controlled rapidly. This study aims to identify the incidence and sources of large volume hemorrhage, discuss successful management strategies, and provide patient care recommendations.
Methods:
An IRB approved (#15-11-WC-0214), single institution retrospective chart review was performed on patients who underwent Nuss bar removal over a 15-year interval. Estimated blood loss (EBL), source of hemorrhage, management, and outcomes are reported.
Results:
One thousand six hundred twenty-eight Nuss bar removal procedures were reviewed. EBL >150 mL occurred in 7 patients (0.43%), of whom 2 patients (0.12%) had EBL >2000 mL. Bleeding sources included: lateral soft tissue, lateral ectopic calcium, medial ectopic calcification, and an intercostal vessel. Most bleeding could be controlled with pressure and electrocautery. Only 2 patients (0.12%) required transfusion. One of these had bleeding from an intercostal vessel, and the other bled from a large vein in the medial calcified substernal tract. No patients sustained heart injury or died.
Conclusion:
Large volume hemorrhage after Nuss bar removal is rare, but may require blood transfusion, thoracoscopic exploration, or open exploration through thoracotomy or sternotomy. Nuss bar removal should be performed in centers capable of these interventions. After bar removal, a chest X-ray and a period of postoperative observation up to 6 hours may be beneficial to detect occult hemorrhage.
Introduction
T
Intraoperative or postoperative hemorrhage following Nuss bar removal is an uncommon but potentially life-threatening complication. There have been reports in the literature of significant hemorrhage at the time of Nuss bar removal due to cardiac laceration and injury to the ascending aorta.10,11 However, the etiology of hemorrhage is not always well understood and often not anticipated. This study aims to identify the incidence of large volume hemorrhage at our institution and categorize sources of hemorrhage, discuss possible risk factors and prevention, and provide potential management strategies.
Materials and Methods
An IRB approved (#15-11-WC-0214), single institution retrospective chart review was conducted of patients undergoing bar removal over 15 years (August 2000–August 2015). Intraoperative estimated blood loss (EBL), source of hemorrhage, techniques to control hemorrhage, patient management, and outcomes were reviewed.
Results
One thousand six hundred twenty-eight patients underwent removal of Nuss bar(s) over the study period. One hundred three (6.3%) had an EBL greater than 25 mL. More extensive blood loss occurred in a smaller percentage of patients (Table 1). In patients with an EBL >150 mL, bleeding occurred from the following locations: lateral soft tissue (i.e., muscle and scar tissue) (4 patients), lateral ectopic calcium (10 patients), medial ectopic calcium (6 patients), and an intercostal vessel (1 patient). In some patients, bleeding occurred from more than one of these locations.
EBL, estimated blood loss.
Bleeding was controlled in the vast majority of patients with pressure and electrocautery. There tended to be higher volumes of blood loss when bleeding was identified from the medial bar tract (EBL: 100, 150, 200, 400, 2000, and 3000 mL), although there was no common predisposing factor identified in these patients. Two patients with bleeding from the medial bar tract required blood transfusions due to an EBL of 2000 and 3000 mL. In one, the source was identified by thoracoscopy to be an intercostal vessel, which was controlled with bipolar cautery. The second patient required a limited right thoracotomy and assistance from a cardiothoracic surgeon, during which bleeding was identified from a large vein in the calcified medial substernal bar tract that was controlled with electrocautery.
None of the patients in this large series experienced a heart injury. There was no mortality. Of the 16 patients with EBL greater than 50 mL, only one had a titanium bar removed.
Discussion
Over 15 years we have removed Nuss bars from 1628 patients. Only 2 (0.12%) required advanced surgical intervention and transfusion. It is still important to be prepared for this rare but potentially catastrophic event. There are five potential sites of bleeding that can be described at the time of Nuss bar removal: lateral soft tissue, lateral ectopic calcification, medial ectopic calcification, intercostal vessels, and heart (Table 2).
Bleeding from the lateral soft tissue usually is minor and is due to muscular bleeding or scar tissue that can be aggravated by a previous infection, previous allergy, or bar migration into the muscle. Bar migration into the muscle can occur due to bars that are made too tight at the time of insertion or in patients that have had significant growth spurts while the bars are in place.
Bleeding from ectopic calcium in the lateral bar tract can be slightly harder to control due to its cancellous nature and on occasions may require topical hemostatic agents and bone wax.
Bleeding from ectopic calcium in the medial bar tract can be more difficult to control with the aforementioned strategies and may require additional maneuvers. If a well-developed tract exists, significant hemorrhage will come from both incisions and sometimes all that is required to achieve hemostasis is direct pressure along the tract. Another technique described by Martinez-Ferro is the Safety String Maneuver that may be used when direct pressure is not successful. This involves tying an umbilical tape to the end of the bar when it is removed and then tying a sponge to the umbilical tape that can be pulled back through the medial bar tract to tamponade hemorrhage (Fig. 1). 12 If hemostasis is achieved and the patient remains hemodynamically stable with this maneuver, further evaluation may not be necessary. However, it is prudent to perform an echocardiogram and chest X-ray (CXR) intraoperatively in this scenario to confirm that there is no fluid in the thorax or pericardium. If all of these studies are negative and direct pressure controls the hemorrhage, we observed the patient overnight and performed a repeat CXR the following day. However, in the event that a well-formed calcified tract does not exist, the hemorrhage may occur into the thorax and may not be seen in the operative field when the bar is removed. In that case, the first clinical sign may be hemodynamic changes hours after bar removal, as occurred in one of our patients.
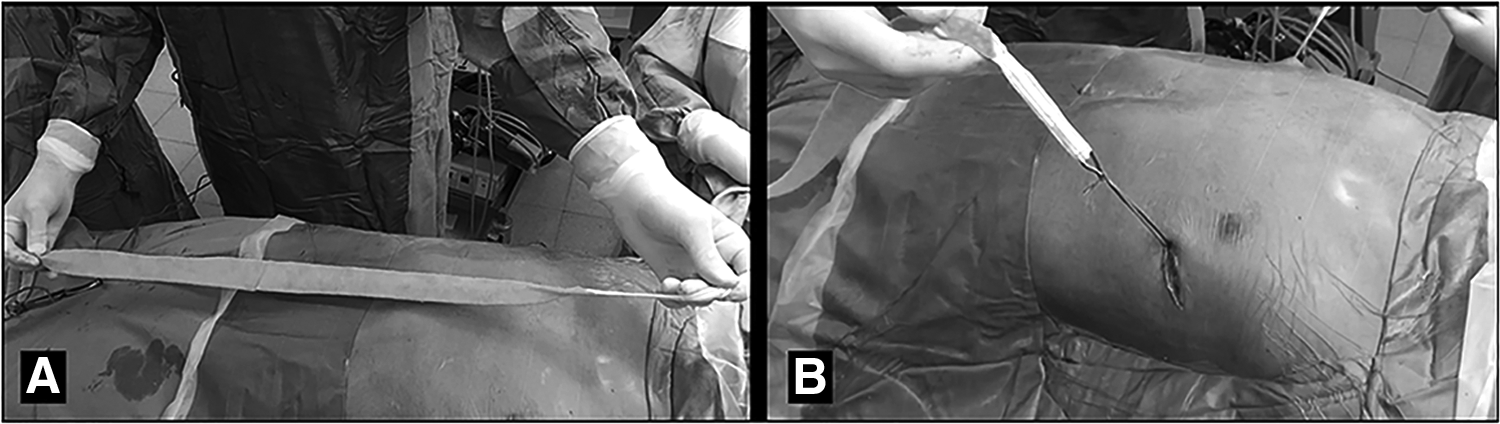
Safety string maneuver.
It is not clear why some patients form more ectopic calcium around the bars. Some authors have recommended preoperative imaging to evaluate for calcifications and position of the bar before removal but this has not been our practice. Since it does not change the plan of care. 10 Extensive calcification is occasionally seen on CXR in the medial tract of some patients after bar removal (Fig. 2).
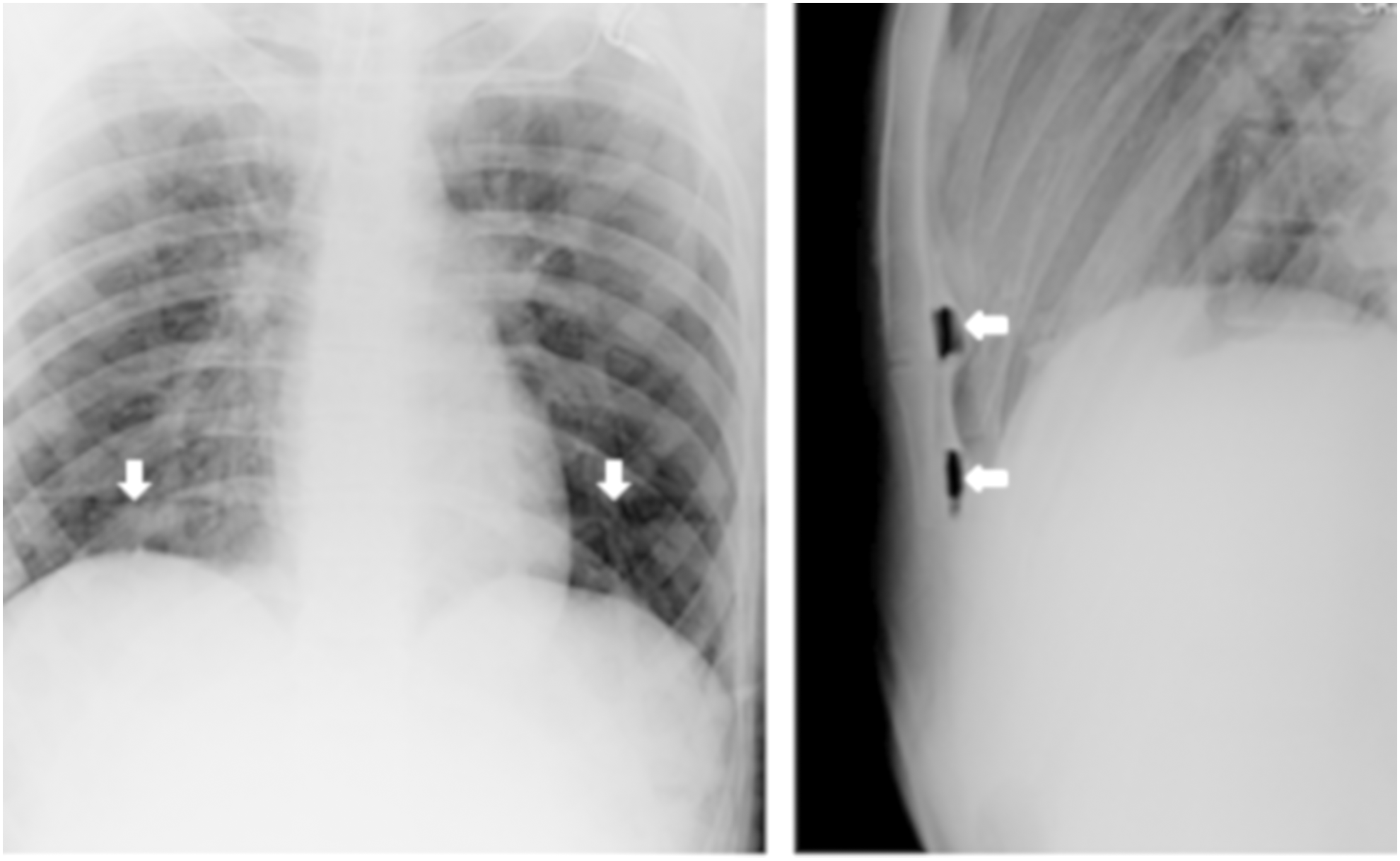
Medial calcifications after Nuss bar removal on AP and lateral images. (Arrows) Extensive calcification is seen around the site of bars, but no erosion into the sternum on the lateral view. The AP view shows radiolucent stripes across the chest outlining the extensive calcification where the bars were located. AP, anterior/posterior.
Bleeding from an intercostal vessel may be due to prior erosion of the bar into this vessel or laceration at the time of bar removal. We have not experienced a heart injury at the time of Nuss bar removal, but this has been described in the literature. 11 To decrease the risk of cardiac injury we recommend ensuring that the bar can be removed with minimal force. This often requires partially straightening the ends of the bar and/or pulling the bar in a manner that follows the curve of the bar to minimize the risk of cardiac laceration as the bar is removed. Risk factors for a cardiac injury may include prior open heart surgery when violation of the pericardium or myocardium is required.
Fortunately, in most cases minor bleeding can be controlled with a combination of manual pressure and electrocautery, but on occasions additional hemostatic agents (i.e., cellulose) and bone wax may be needed. Although rare, excessive bleeding from fractured ectopic calcium in the medial tract, lacerated intercostal vessels, or cardiac injury may require additional surgical intervention. The surgeon should have a low threshold for additional intraoperative intervention to improve exposure and obtain hemostasis. Depending on the specific clinical scenario and hemodynamic stability of the patient, an initial thoracoscopy can be performed, but open thoracotomy and sternotomy may be necessary. Intraoperative cardiothoracic surgery consult may be considered.
A summary of the potential risk factors, preventive strategies, and management strategies based on the source of intraoperative hemorrhage is provided in Table 2. We suggest several steps to be prepared for unexpected bleeding. Nuss bar removal procedures should be performed in a facility capable of blood transfusion, thoracoscopy, and thoracotomy. Therefore, we do not recommend these procedures be performed in an ambulatory surgery center. Second, since one of our patients did not become symptomatic until 3 hours postoperatively, we think it is reasonable to consider an extended period of postoperative observation with serial vital signs and repeat imaging for any concerns. Finally, when excessive bleeding occurs it is advisable to avoid ketorolac and other nonsteroidal anti-inflammatory medications as these may increase the risk of bleeding.
Conclusion
In our experience, the majority of bleeding at the time of Nuss bar removal is minor and can be controlled with simple surgical maneuvers. Large volume hemorrhage was exceedingly rare, but did require blood transfusion and more advanced surgical intervention in 2 patients. It is advisable to perform Nuss bar removal in centers capable of these interventions rather than outpatient surgical centers. After bar removal, a CXR and a period of postoperative observation up to 6 hours may be beneficial to detect occult hemorrhage. Knowledge of this potential complication and having a strategy to manage any untoward event are important lessons learned from our experience.
Footnotes
Acknowledgment
The authors acknowledge the assistance of Dr. Robert E. Kelly, Jr. in article review and preparation.
Disclosure Statement
Dr. Obermeyer is a product development consultant for Zimmer-Biomet, Inc., manufacturers of the bar used in the Nuss procedure.