
Abstract
Aim of the Study:
Necrotizing enterocolitis (NEC) is a devastating intestinal disease that mainly affects preterm infants. Despite advancements in neonatal care, mortality of NEC remains high and controversies exist regarding the most appropriate time for surgical intervention and challenging of diagnosing NEC. Using a pig model of NEC, we aimed to examine if laparoscopy is feasible for diagnosis of NEC.
Methods:
Preterm caesarean-delivered piglets (n = 42) were fed with increasing amounts of infant formula up to 5 days to induce NEC. On days 3–5, we examined the intestine by laparoscopy under general anesthesia. The bowel was examined by tilting the pigs from supine position to the left and right side. Macroscopic NEC lesions were identified and graded according to a macroscopic scoring system, then a laparotomy was performed to rule out any organ injury and missed NEC lesions.
Results:
Visible NEC lesions (scores 4–6) were found in 26% (11/42) of the piglets. A positive predictive value of 100% was found for laparoscopy as a diagnostic marker of NEC in both colon and the small intestine. One piglet had a higher NEC score in the small intestine found at laparotomy, than at laparoscopy, resulting in a sensitivity of 67%, and a specificity of 100% for the small intestine. Conversely, both the sensitivity and specificity for colon was 100%. Acceptable levels of agreement was found, with minimal proportional bias in both colon and the small intestine for laparoscopy and laparotomy. Ultrasound examination had a lower sensitivity of 67% and specificity of 63%. All piglets were respiratory and circulatory stable during the procedure.
Conclusions:
In preterm piglets, laparoscopy is a feasible tool to diagnose NEC with a high positive predictive value and a high specificity.
Introduction
Necrotizing enterocolitis (NEC) is an acute condition in neonates, which remains a leading cause of neonatal morbidity and mortality. The management in the early stages is mostly conservative using antibiotics, cessation of enteral feeding and total parenteral nutrition, accompanied by frequent repeated X-ray examinations and/or ultrasound (US) of the abdomen.1–3 In some cases, the condition deteriorates despite medical treatment, and surgical intervention becomes necessary. 4 In NEC patients, where surgery is needed, the mortality is as high as 50%.5,6 Optimizing the timing and decision of surgical intervention might result in a better outcome for surgical NEC patients.
It is a challenging decision whether to operate or not, and the most common and only absolute indication for surgery is intestinal perforation as evidenced by pneumoperitoneum 7 On the other hand, there are several relative indications based on clinical, paraclinical, and radiological parameters. 8
Traditionally, plain abdominal radiography is of the most used imaging modality for evaluating NEC, but early stages of NEC cannot be identified by X-ray. Pathognomonic findings, like free intraabdominal gas, is a relatively late finding in the disease progression, indicating perforation. 9 Abdominal US has been used as a useful adjunct to radiography for evaluating NEC. Detection of portal venous gas is a major advantage of US over plain abdominal radiography. Furthermore, US is superior to plain abdominal radiography for evaluating accumulated intraperitoneal free fluid, and the neonates are exposed to significantly less radiation.8,10
When radiological markers are missing, a clinical dilemma ensues, together with insufficient clinical signs of surgical NEC may sometimes result in the lost opportunity to perform surgery, as the neonate may become too unstable to survive the procedure or on the other hand resulting in unnecessary surgery.11,12
Some initial studies suggest that laparoscopy may be of importance in providing information regarding intestinal viability, and extent of NEC lesions, thereby assisting decision making regarding the need for laparotomy.13–15 It gives the opportunity to assist the surgeon in diagnosing cases that would further benefit from a laparotomy. A recent international survey showed that laparoscopy for diagnosis and/or treatment of NEC is performed by only 8% of pediatric surgeons. 2
Surgical NEC is an infrequent condition, limiting the possibilities of large trials, therefore an animal model is needed.
The aim of this study was to establish a model in preterm piglets with clinical symptoms of NEC. The model should be comparable to neonates with NEC, giving us the opportunity to investigate, if laparoscopy could be used to diagnose NEC compared with today's gold standard, a laparotomy.
Our piglet model with induced NEC is a well-described animal model and has previously been described and used in research studies on baby formula tolerance.16,17
Materials and Methods
Seventy-four piglets from 3 litters were born preterm by caesarean section at day 106 of gestation (i.e., 90%–92% of expected full-term gestational length). The preterm piglets were immediately transferred to the neonatal intensive care unit, and reared in temperature- and oxygen-regulated incubators. The piglets were all weighed and fitted with a vascular catheter (infant feeding tube, 4F; Portex, Kent, United Kingdom) inserted into the dorsal aorta through the transected umbilical cord using aseptic technique. Additionally, a gastric feeding tube (8F Portex) was placed and inserted through the cheek and secured by sutures. 17 Passive immunization with maternal plasma (16 mL/kg body weight during the first 24 hours) was administered through the arterial line. 16
Experimental procedures conducted during the animal experiment were approved by the Danish Animal Experiments Inspectorate (License No: 2014–15-0201-00418) in accordance with the guidelines from the Directive 2010/63/EU of the European Parliament.
All piglets received parenteral nutrition through the umbilical catheter using a modified parenteral nutrition composition to meet the nutritional requirements for piglets (Kabiven® and Vamin®; Fresenius, Bad Homburg, GE), administered at 4 mL/kg/h (first day) and 6 mL/kg/h (day 2–5) in all 3 litters.
Enteral nutrition was prepared by a commercial product for feeding infants and administrated with increasing volume, over time, so the piglets would develop NEC. 18 The commercial product was administered by the orogastric tube (Liquigen MCT® and Pepdite®; Nutricia, Utrecht, NL and DI9224; Arla Foods Ingredients, Viby, Denmark). Initially, a bolus (3 mL/kg), during the first 4 hours after birth and after that enteral nutrition, was given with increased amounts every 3 hours up to 15 mL/kg (120 mL/kg/day). Each piglet was clinically assessed at least twice daily.
The piglets were fasted 6 hours before surgery and were randomized to surgery at day 3, 4, or 5 after birth. Due to limited facilities, it was not possible to operate all piglets in 1 day. They were premedicated with an intramuscular injection of butorphanol (0.1 mg/kg, Torbugesic®; Scan Vet, Fredensborg, Denmark). On the operation day an abdominal US examination was performed using a pediatric abdominal neonatal, micro convex 8C RS transducer, on a portable Vivid™ I scanner (GE Healthcare, Gloucestershire, United Kingdom) to determine the presence or absence of gas in the portal vein or liver parenchyma. Also the presence or absence of intraperitoneal free fluid was noted. After this the piglets were anesthetized with sevoflurane (SevoFlo®; Orion, Copenhagen, Denmark), intubated with a cuffed endotracheal tube size 3.0 (Rüsch, Athlone, IE), and ventilated with the Hallowell anesthesia workstation (Anesthesia workstation w/100 mL; Hallowell EMC, Pittsfield, MA).
The piglets were placed in a supine position, and were kept warm by heated rice pads and plastic covers. Using an open technique, a bladeless 5 mm camera port (Medtronic, Copenhagen, Denmark) was placed 1 cm caudal to the sternum, and an insufflation needle (Covidien, Copenhagen, Denmark) was placed in the left side of the abdomen and CO2 was insufflated to maintain pneumoperitoneum at a pressure of 6 mmHg. The 5 mm laparoscope was inserted in the camera port (ICG-Hopkins® telescope 0°, 5 mm; Karl Storz Gmbh and Co. KG, Tüttlingen, GE) connected to a camera system (IMAGE1®; Karl Storz Gmbh and Co. KG) and a light source (D-light P®; Karl Storz Gmbh and Co. KG).
The bowel was examined laparoscopically by a nontouch technique with no additional ports or instruments. To visualize the intestines, the piglets were tilted slowly from supine position to the left and right side. Subsequently, a laparotomy was performed to validate the laparoscopic findings. NEC lesions were scored in agreement by the same 3 surgeons present during all laparoscopies and laparotomies, according to a well-described macroscopic scoring system (1–6 for increasing NEC-severity until necrosis 17 ) (Table 1). Score 1–3 were considered healthy or with none clinical relevant NEC lesions.
Macroscopic Score
Systolic and diastolic blood pressure and arterial oxygen tension were monitored during the experiment. At the end of surgery, the piglets were euthanatized by an intracardiac injection of sodium pentobarbital (Euthanimal; ScanVet Fredensborg, Denmark).
Statistics
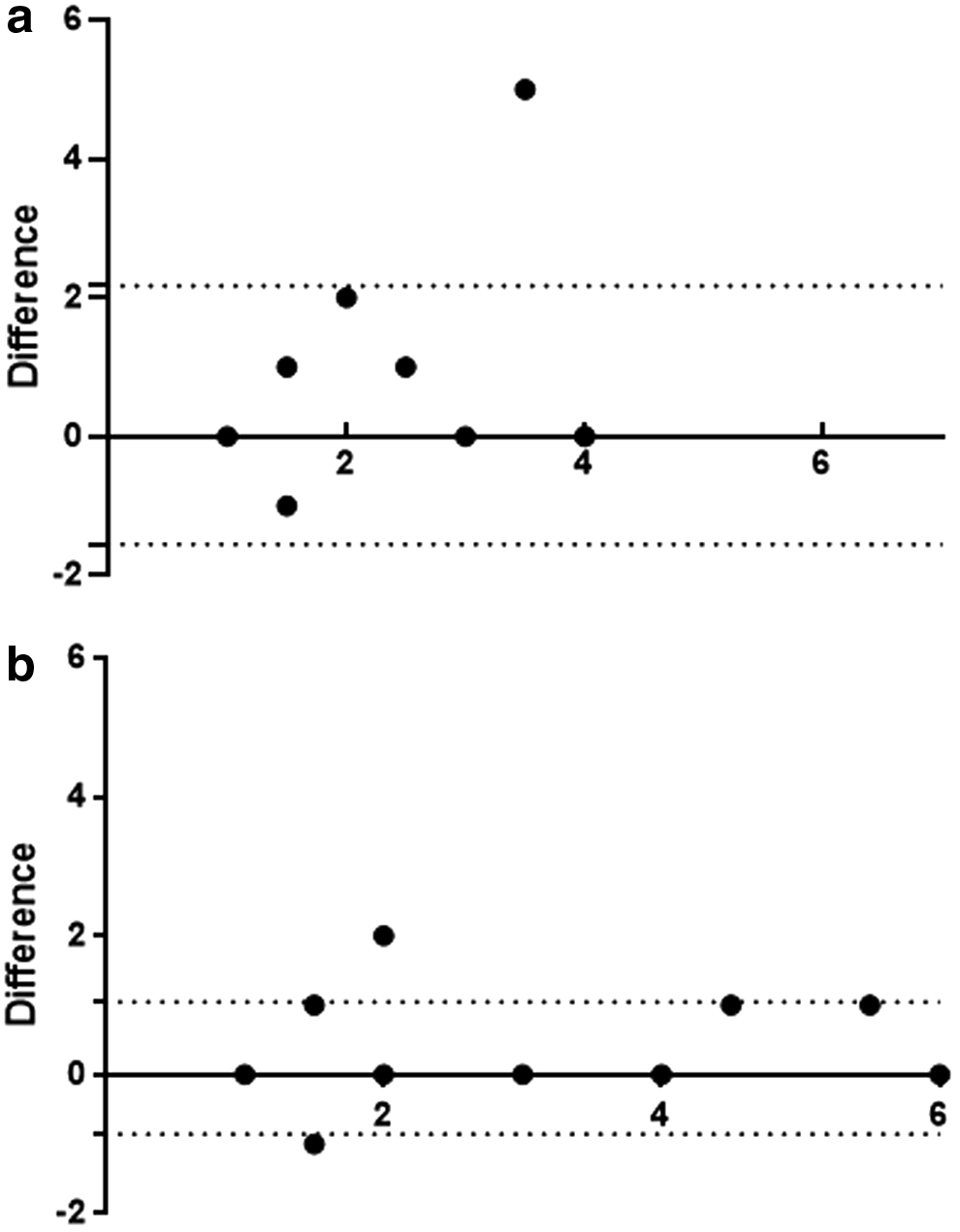
Statistical analyses were performed with GraphPad Prism™ 7.0 (GraphPad Software, Inc., San Diego, CA). Applying the Shapiro–Wilk test, data were found to be non-normal distributed. The resemblance, was assessed by a Bland–Altmann plot, with 95% limits of agreement.
Calculations of sensitivity, specificity, positive predictive value, and negative predictive value of laparoscopic examination relative to findings of current standard laparotomy were made. Likewise, the same calculations were applied to compare US findings relative to that of laparotomy. The calculations were: Sensitivity = a/(a + b), specificity = d/(c + d), positive predictive value = a/(a + c), and negative predictive value = d/(b + d), where a = number of true-positive cases, b = number of false-positive cases, c = number of false-negative cases, d = number of true-negative cases.
Macroscopically positive cases for NEC were defined as bowel lesions score 4–6 and negative cases as healthy or macroscopic invisible bowel lesions, with no need of surgery (score 1–3). A positive US was defined as gas in vena portae and/or gas in the liver parenchyma, and/or free intraperitoneal fluid.
Results
Of the total number of live-born piglets (n = 74), 32 were euthanatized due to general prematurity symptoms and/or poor respiratory function from which they did not improve within the first 48 hours. Mean weight of the remaining 42 piglets was 0.90 ± 0.03 kg (Table 2), and we found NEC lesions (score 4–6) in 11 of these (26%). All piglets were hemodynamically and respiratory stable during the experiment (Table 2).
Demographic Characteristics (n = 42)
Values are mean ± SE.
SE, standard error.
The Bland–Altmann plots for comparison are shown in Figure 1a and b. Acceptable levels of agreement was found with minimal proportional bias for both colon and the small intestine, but a greater agreement for NEC lesions in colon.
Scoring of NEC lesions at laparoscopy and laparotomy is illustrated in Tables 3 and 4. Figures 2 and 3 illustrate NEC-lesions.
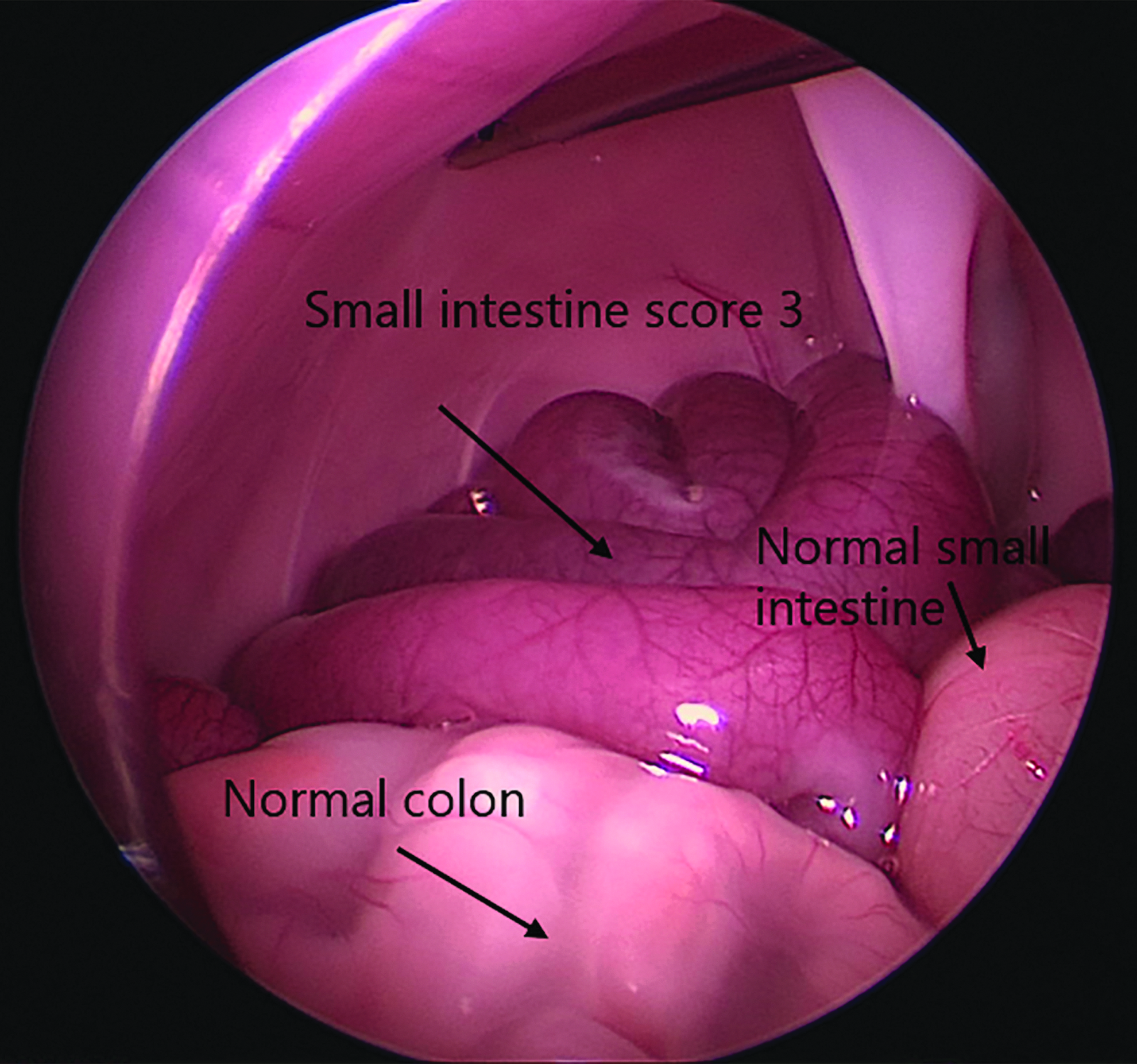
Laparoscopic illustration of a piglet with NEC. NEC, necrotizing enterocolitis.
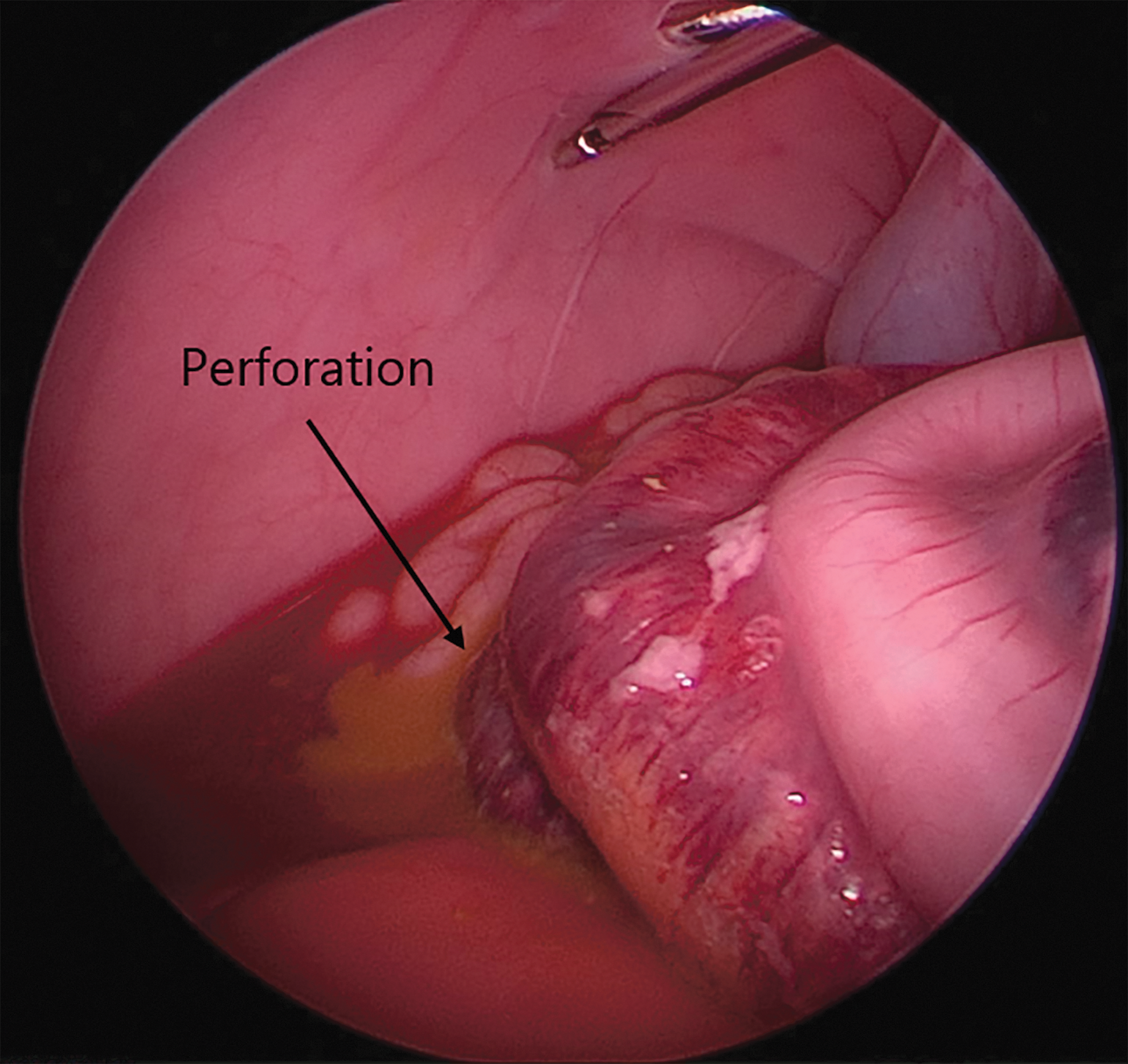
Laparoscopic illustration of a piglet with NEC score 6 and a perforation in colon. NEC, necrotizing enterocolitis.
Necrotizing Enterocolitis Score at Laparotomy and Laparoscopy in the Small Intestine
Necrotizing Enterocolitis Score at Laparotomy and Laparoscopy in Colon
Laparoscopy as a diagnostic marker of NEC (score 4–6), was found to have higher sensitivity in colon (100), than in the small intestine (67). The specificity and positive predictive value was high (100) for both the small intestine and colon. The negative predictive value for colon was higher (100) than for the small intestine (98) (Table 5).
Calculated Diagnostic Parameters of Laparoscopy
In one of the piglets, a higher NEC score was found at laparotomy. The lesion (score 6), which was not detected by laparoscopy, was located in the distal part of the small intestine.
In 3 piglets, an US was not possible to perform, as the piglets were not lying still. Table 6 is illustrating the findings by US. A low positive predictive value (35), a sensitivity at 67%, and a specificity at 63% were found, which were lower than for laparoscopy (Table 7).
Necrotizing Enterocolitis Score at Laparotomy and Ultrasound in Both Small Intestine and Colon
US, ultrasound.
Calculated Diagnostic Parameters of Ultrasound
Discussion
In a clinically relevant animal model of NEC, our study shows that laparoscopy is a feasible technique, with high specificity. In addition, there was a sufficient agreement with the findings for laparotomy, for identifying NEC lesions. However, one lesion, in the distal part of the small intestine was missed. For abdominal US a low sensitivity (67) and positive predictive value (35) were found.
NEC is a serious neonatal condition with high mortality, and during the last decades only minor improvements in survival rates have occurred. 19 Surgical management of infants with suspicion of NEC and absence of cardinal signs of perforation poses a great challenge. Here, laparoscopy may be an important novel diagnostic tool to diagnose NEC as a less-invasive procedure compared with laparotomy.
It only becomes more challenging in cases with NEC, when all attempts of maximizing medical therapy have been exhausted, and at the same time, no absolute indication for surgery is present. In such cases with suspected NEC, a diagnostic laparoscopy could be a useful procedure to identify neonates who may benefit from further surgery. Laparoscopy is less invasive than laparotomy, associated with less morbidity, and would be able to access an early diagnosis of surgical NEC, which is of particular importance for survival in critically ill neonates with NEC requiring surgery.20–22
Until now, there is limited published evidence on diagnostic laparoscopy in neonates with NEC.13,14,23 An important issue has been the possible false-negative laparoscopies, missing an intestinal lesion; such reticence is initially not contradicted by our results.
We decided not to manipulate the small intestine with instruments during the procedure, making the procedure as less invasive as possible, resulting in relatively low sensitivity for the small intestine (67), and a more marked agreement in colon than the small intestine in this study. Another reason for choosing a laparoscopy by one port only, was that the piglets were included in an additional study where intestinal microcirculation was assessed. During these measurements, manipulation of the small intestine was not allowed with instruments. Accordingly, it would be necessary to insert two intestinal graspers and handle the bowel systematically as a diagnostic laparoscopy, to visualize all parts of the small intestine. On the other hand, this approach would increase the risk of injuring the fragile wall of the small intestine.
Differences in sensitivity between the small intestine and colon may also be related to the anatomy of the gastrointestinal tract in piglets, where a spiral formed colon is placed in the left side of the abdomen, whereas the placement of the small intestine is similar to that in the neonates. This means that, in our study, the colon was therefore easier visualized by laparoscopy than the small intestine, and this might also be the case in neonates due to the shorter and more fixed colon.
The negative predictive value and the specificity of laparoscopy were high in both the small intestine and colon, indicating that a laparoscopy is a good diagnostic tool to identify cases that might not benefit from immediate surgery, and other reasons for clinical symptomatology should be considered. This is important as prolonged conservative treatment of neonates with antibiotics, and cessation of enteral feeding may be avoided in neonates who had a negative diagnostic laparoscopy.
In a study of 11 infants with suspected NEC, the use of diagnostic laparoscopy resulted in 5 infants avoiding laparotomy, and NEC was excluded in 2 infants. 14 Since this study, only few studies and case reports have advocated for the use of laparoscopy in the diagnosis of NEC.13,15,23 It is remarkable that in an international survey in 2014, only 8% of pediatric surgeons would consider laparoscopy for diagnosis and or treatment of NEC. 1
In neonates with NEC and pneumoperitoneum, laparoscopy has been suggested as a useful tool to localize the exact site of perforation and avoid extensive bowel handling, as the perforation can be treated through a 1-cm mini laparotomy. 15 In our study, we identified by laparoscopy a NEC lesion with a perforation, and for surgical treatment it might have been sufficient to only carry out a mini laparotomy after the laparoscopy.
It is often discussed whether it is safe to perform pneumoperitoneum by CO2 in neonates because of the risk of hemodynamic and respiratory changes. Earlier studies have been found to affect respiratory and cardiovascular parameters when elevating the intra-abdominal pressure up to as much as 20 mmHg.22,24–26 In our study, we found stable blood pressure and saturation during the experiment, but we only elevated the intra-abdominal pressure to a maximum of 6 mmHg, which was sufficient to overview the abdomen, and it was a short procedure of under 10 minutes.
A challenge in the current treatment of NEC is the uncertain diagnosis of NEC in the early stages. Until now, no early biomarkers are available and we found poor value of the US evaluation, even though other studies showing that US is clearly more sensitive than conventional abdominal radiography in detecting, for example, portal venous gas. 27
The neonates with suspected NEC often become critically ill before they receive surgical interventions.5,14 It may be possible to avoid extensive bowel resection if the diagnosis is made earlier, and even improve the prognosis, but evidence is missing and is difficult to obtain in this population of very sick infants.
Accordingly, an animal model like the one described in this study is needed, also to explore different treatment opportunities. The animal model is feasible and the abdominal lesions obtained with our approach is similar to those observed in premature infants with NEC.
It was also technically possible to perform a laparoscopy in a premature piglet with NEC and a body weight down to 400 g. Laparoscopy could, as mentioned, be possibly used to diagnose early stages of NEC, and the diagnostic property might be improved by adding a technique to measure bowel perfusion. In the future, laparoscopic evaluation, combined with assessment of the intestinal perfusion, may help diagnostic accuracy in the early stages of NEC.
Numanoglu et al. used fluorescein together with laparoscopy in 13 neonates with NEC, where the fluorescein could add knowledge about hypoperfused bowel in 3 out of 13 neonates where it was not macroscopically visible. 23 The technique by administrating an intravenous fluorescence agent, has already been performed in a premature piglet model. 28
We found our model sufficient in giving us the opportunity to investigate if laparoscopy could be used to diagnose NEC compared with today's gold standard, a laparotomy. The weakness of our study is related to the modest sample size of piglets, not allowing us to do valid statistics on subgroups of NEC grading, but the studies on the present piglet model are also expensive.
However, using a clinically relevant animal model of NEC, which are in many ways similar to preterm infants with NEC, we conclude that laparoscopy is a feasible technique with a good agreement to laparotomy, and high specificity (100) to identify NEC lesions. It could be an earlier diagnostic tool, especially when the NEC diagnosis is challenging due to unspecific clinical signs and limited sensitivity by conventional imaging techniques, although further research is needed. US had a low positive predictive value (35) and was not a sufficient diagnostic tool to diagnose NEC. The sensitivity to detect NEC could have been increased by using an instrument to examine the bowel systematically, but that probably entails a risk of iatrogenic lesions.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.