
Abstract
Abstract
Background:
Traditionally, Billroth I procedure or bypass gastrojejunostomy were the recommended approaches for management of postcorrosive complete gastric outlet obstruction (GOO), whereas Heineke Mickulicz pyloroplasty was recommended for moderate mucosal injury with partial cicatrization. In this study, laparoscopic diamond antroduodenostomy was carried out as an alternative minimally invasive approach for cases with pyloric cicatricial obstruction.
Patients and Methods:
Between January and December 2017, children who were referred to Pediatric Surgery Department, Cairo University Hospital, with GOO as a consequence of caustic liquid ingestions were included in this study. Laparoscopic diamond antroduodenostomy was performed for the presented cases.
Results:
Through the year 2017, 5 cases were approached with laparoscopic diamond antroduodenostomy. Isolated pyloric cicatrization was evident in 4 cases, whereas synchronous insult to thoracic esophagus and pylorus was manifest in the fifth case. Laparoscopic feeding jejunostomy completed the procedure for the case with esophageal stricture. Contrast study—24 hour postoperatively—assured no radiological leaks in the presented cases, where enteral feeding was gradually commenced, and patients discharged home a day later. After a mean follow-up of 13.5 months, neither recurrence of obstructive symptoms nor dumping was displayed. Cosmetic outlook inherent to the minimally invasive approach was appreciated by the parents.
Conclusion:
Laparoscopic diamond antroduodenostomy is a feasible approach for management of postcorrosive pyloric obstruction. It allowed early enteral feeding, with no dumping symptoms, in addition to the fundamental advantages of minimally invasive surgery. A bigger series and longer follow-up is recommended to verify the reported results.
Introduction
Accidental ingestion of corrosive chemicals is not uncommon in developing countries. 1 The resulting mucosal damage is largely linked to the nature, volume, and concentration of the ingested corrosive; stomach is the vicinity of corrosive acids' burn, whereas esophagus is burned by alkalis.2,3 Nevertheless, synchronous insults to both esophagus and stomach have been reported with either substances ingestion.4,5
Gastric outlet obstruction (GOO) is an anticipated consequence to strong acids; ascribable to pooling of the ingested acid just ahead of a corrosive-induced pylorospasm. 6 Furthermore, cicatrization can inflict the antrum, body, pyloroduodenal area, or the entire stomach.7–9
Once the diagnosis of GOO is confirmed, early intervention should be carried out. Recommended approaches were endoscopic balloon dilations of pylorus, Heineke Mickulicz pyloroplasty, Billroth I gastric resection or bypass gastrojejunostomy. 10 In this study, laparoscopic diamond antroduodenostomy was carried out as a less invasive alternative approach, following the footprints of laparoscopic repair of neonatal duodenal atresia. 11
Patients and Methods
Through the year 2017, all children referred to Cairo University Specialized Pediatric Hospital with postcorrosive confined pyloric cicatricial obstruction were prospectively included in this study. Excluded from the study were cases with extensive esophageal and/or gastric insult (contracted stomach) or pyloroduodenal strictures.
Preoperative patients' preparation included upper gastrointestinal (GI) endoscopic evaluation of esophageal and gastric mucosa. A nasogastric tube (Ryle) was kept for preoperative gastric decompression and lavage.
Children were placed lithotomy at the end of the table, where the surgeon stood between child's legs, with the cameraman on his left hand side. Figure 1 depicts patient positioning and port-site placement. We followed the surgical principles of laparoscopic diamond duodenoduodenostomy in neonates.
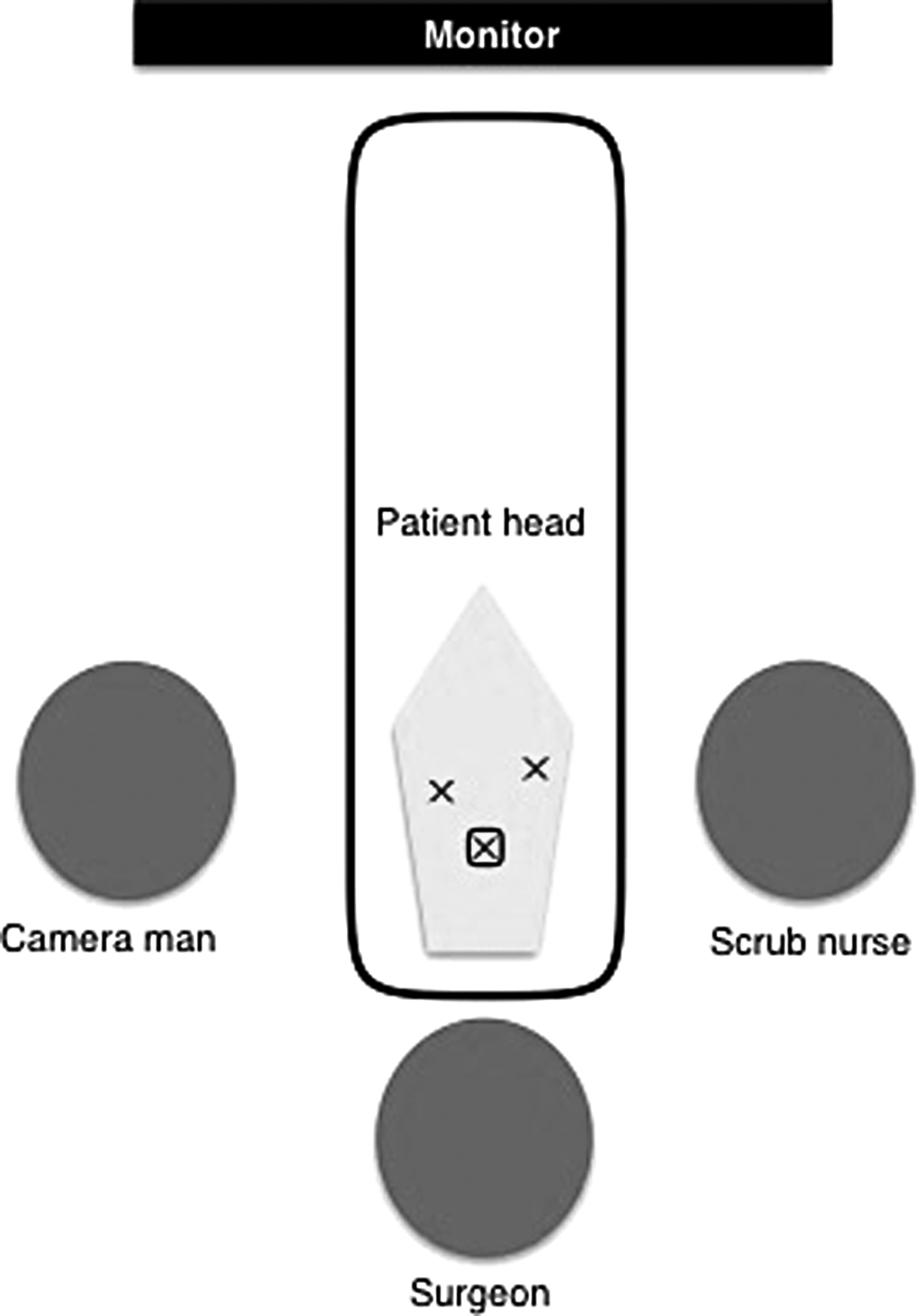
Patient positioning and port-site placement.
Laparoscopic exploration started with evaluation of the contracted cicatrized pyloric ring. Two stay sutures were applied: one hitching the falciform ligament up to the abdominal wall to retract the liver and the other one hitching the anterior gastric wall close to the antrum.
A monopolar cautery device was used to introduce a transverse enterotomy in the healthy pyloric antrum and an equal longitudinal one in the first part of the duodenum. Diamond antroduodenostomy was then accomplished through a single-layered interrupted intracorporeal sliding tumble-square knots, using 4/0 Vicryl.™ No abdominal drains were left by the end of the procedure.
Under C-arm, 24 hour postoperative, a diluted contrast was injected through the nasogastric tube to check anastomotic integrity and to assess gastric motility. Oral fluids were gradually allowed when appropriate, and patients were discharged home a day later.
Regular clinic visits were scheduled for follow-up of operated cases. Upper GI series was ordered a month, postdischarge.
Results
During the inclusion period of the study, 1554 children presented to Cairo University Hospital with corrosive substance ingestion; 736 chloracetic acid and 818 varieties of other corrosive materials (including hydrochloric acid, potassium hydroxide, sulfuric acid, and others). Five cases referred to Pediatric Surgery Unit for management of GOO were included in this study.
The ingested substance was floor detergent (containing hydrochloric acid) in 2 cases, caustic potash (potassium hydroxide) in 1 case, and nonwitnessed in 2 cases. The presenting complaint in 4 cases was recurrent attacks of nonbilious foul-smelling vomiting, 17 days on the average from witnessed events (range 14–25 days). No oropharyngeal stigmata of corrosives were detected on physical examination.
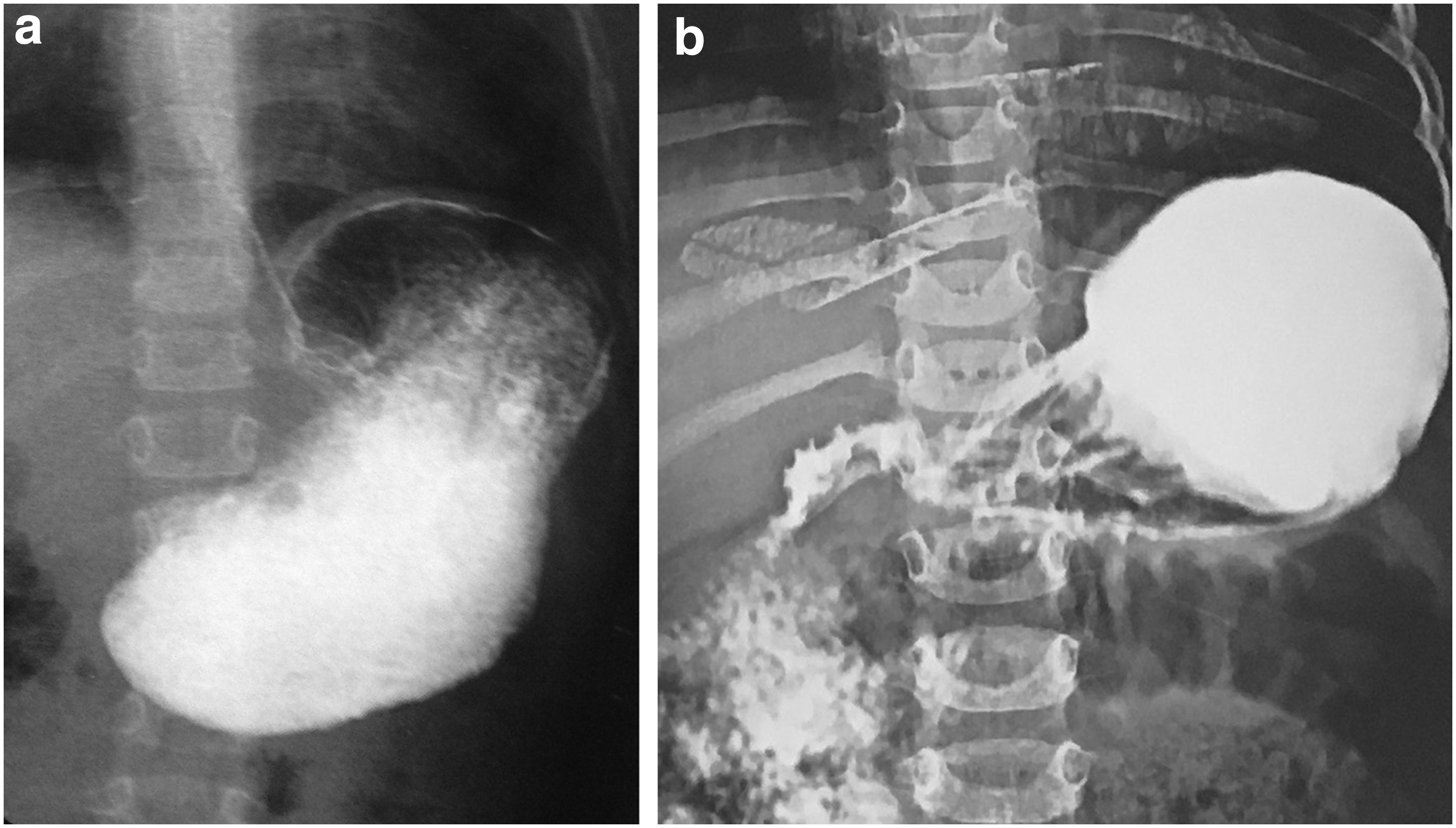
Contrast studies showed near complete pyloric obstruction in all 5 cases (Fig. 2a), with additional stricturing of mid-esophagus in 1 case that had dysphagia as the leading complaint. Upper GI endoscopy denoted nonreactive pylorus; distorted and stenotic, with grade A reflux esophagitis and hyperemic gastric mucosa.
Under general anesthesia (GA), laparoscopic diamond anastomosis between pyloric antrum and first part of duodenum was carried out to bypass the obstructed fibrotic pyloric ring. Patients' ages at operation were 1 year 6 months, 1 year 9 months, 2 years, 5 years, and 3 years 3 months; weighing 6.2, 8, 7, 18, and 9.5 kg, respectively.
Operative time ranged between 72 and 89 minutes (average 81 minutes). Contrast studies, 24 hour postoperatively, assured no radiological leaks in the presented series (Fig. 2b), with delayed gastric emptying in 2 cases. Enteral feeding was gradually commenced on the third postoperative day, and all patients were discharged home a day later.
Eight weeks postdischarge, weight gain in the included cases was ranging between 2.1 and 3.8 kg, with an average of 2.35 kg (nearly 24% of preoperative weight). After a mean follow-up of 13.5 months (range: 8.8–18.6 months), neither recurrence of obstructive symptoms nor dumping was displayed. Cosmetic outlook inherent to the minimally invasive approach was appreciated by the parents.
Discussion
Although initial description was in 1828,12,13 it was not till 1962 where the natural history of gastric burn caused by corrosive acids was thoroughly reported by Karon as “the delayed gastric syndrome with pyloric stenosis and achlorhydria.” He reported a quiescent phase (1–2 weeks) after the acute event, before the launch of gastric obstructive symptoms (2–6 weeks). 14
Once diagnosed, early intervention for management of GOO should be prompted. 10 However, reports are divided between primary and delayed surgical repair, as they are for the nature of surgical repair.10,15
Tekant et al. 10 in his series (n = 6) of postcorrosive GOO carried out early definitive surgical intervention (average 5 weeks postingestion); balloon dilatation of the pylorus, pyloroplasty, or Billroth I procedure; based on findings at laparotomy. During a mean follow-up period of 22 months, one of his cases needed reoperation (because of intestinal obstruction after a Billroth I procedure), whereas the rest were free of obstructive symptoms.
In contrast, Chaudhary et al. 15 adopted a staged approach in his series (that included 25 cases of postcorrosive GOO); initial feeding jejunostomy to optimize the nutritional status and allow the inflammatory process to settle down, and delayed elective definitive surgery after an interval of 7 months on the average. He argued that mural response to burn is ongoing for 3 months postevent, and earlier surgical intervention would be risky and un-definitive.15,16 Furthermore, he preferred radical excision of scarred tissues (Billroth I or II), and preserved gastrojejunostomy with or without truncal vagotomy for otherwise risky patients. Apart from 1 case that developed early postoperative duodenal fistula, his cases were doing well at regular follow-up.
However, in the presented series (n = 5), for the recurrent nonbilious vomiting ascribable to postcorrosive GOO, we applied early definitive surgical repair to regain early continuity of the bowel, utilizing a minimally invasive approach.
The following operative steps were taken from the description of laparoscopic repair of neonatal duodenal atresia, 11 rather than been a novel description. The concurred merits of laparoscopic diamond duodenoduodenostomy, 17 and the proximity of pyloric ring to duodenum inspired the application of the same approach for management of the studied cases. This minimally invasive approach allowed precise performance of the anastomosis with minimal bowel handling that helped greatly early enteral feeding, with fastened patient recovery. None of the included cases needed reoperation at a mean follow-up of 24 weeks.
Midterm follow-up of the included cases proved the efficacy of the described approach for management of postcorrosive GOO. However, longer follow-up period and bigger patient sample seemed necessary to prove these results.
Conclusion
Laparoscopic diamond antroduodenostomy is a feasible minimally invasive approach for management of children with postcorrosive pyloric cicatrization. It allowed early enteral feeding, with no dumping symptoms, in addition to the fundamental advantages of minimally invasive surgery. A bigger series and longer follow-up is recommended to verify the reported results.
Footnotes
Disclosure Statement
No competing financial interests exist.