
Abstract
Abstract
Purpose:
Neonatal exploratory laparotomies are often performed with a transumbilical incision in our institution, so umbilical ostomy placement has become more common. The purpose of our study is to evaluate the outcomes of neonates with ostomy placement at the umbilicus in comparison to more traditional stoma locations.
Material and Methods:
Retrospective study of neonates that underwent an exploratory laparotomy with ostomy creation between January 2010 and September 2015. Demographics, presentation, feedings, ostomy position, postoperative complications, and outcomes were collected. Comparative analysis was performed in STATA with P-value <.05 determined as significant. Results reported as means ± standard deviation and medians with interquartile ranges.
Results:
Fifty-four children were included, 37% (n = 20) had stomas at the umbilicus. Most common other stoma location was the right lower quadrant (63%, n = 34). Necrotizing enterocolitis (NEC) was the most common indication for surgery in both groups. Days to stoma output were similar between the two groups, [3 (1, 6) versus 2 (1, 5), P = .96]. Days to initiation of feeds were delayed in the umbilical ostomy group [15 (9.5, 23.5) versus 6 (4, 10), P = .02]. Comparing only NEC patients, initiation of feeds was similar [22 (14, 56) versus 15.5 (8, 43), P = .73]. Umbilical ostomies had an increase in prolapse/peristomal hernias (7 versus 3, P = .01), but no patients required operative revision.
Conclusion:
Umbilical ostomies had similar time to stoma function compared to other sites, but a delay in initiation of oral feeds likely secondary to a higher percentage of patients with NEC.
Introduction
I
Materials and Methods
Following IRB approval (#17080503), a retrospective chart review of neonates who underwent an exploratory laparotomy with ostomy creation between January 2010 and September 2015 was conducted. Patient lists were obtained from our IT department utilizing International Classification of Disease (ICD-9 and ICD-10) diagnosis codes correlating to malrotation and the current procedure terminology codes for ostomy creation, ileostomy, jejunostomy, colostomy, mucus fistula, necrotizing enterocolitis, intestinal stricture, intestinal atresia, anorectal malformations, bowel perforations, and bowel obstruction. Patients with ostomies were classified according to whether or not placement occurred at the umbilicus. Demographics, anthropometrics, presentation, diagnostic tests, elements of surgical interventions, time to initial and full feeds, postoperative care, and any associated short- (<30 days) and long-term (≥30 days) complications were reviewed. Complications reviewed included obstruction, wound issues, prolapse, high ostomy output, perforation, hernia, and death. We also collected information on issues with ostomy care, the two issues we focused on were ostomy prolapse/peristomal hernia and bagging issues. Bagging issues most commonly involved difficulty creating a seal around an ostomy or finding the appropriate bag size for the patient.
At our institution, typically an abdominal exploration is done through a periumbilical incision. After extrusion of the bowel through this incision, the appropriate operation is performed. When an ostomy is required, it is created either as an end ostomy or ostomy with mucous fistula at the superior or inferior edge of the incision.
Descriptive statistics was performed with all means reported ±standard deviation. Comparisons between groups were analyzed on STATA (StataCorp 2017, Stata Statistical Software: Release 15; StataCorp LLC, College, Station, TX) using T tests with a significance of <0.05.
Results
Fifty-four children were identified, 37% (n = 20) had stomas at the umbilicus and 63% (n = 34) had stomas at other sites. Patients who had an umbilical ostomy were similar in age at the time of surgery (19.35 ± 17.5 days versus 33.5 ± 99.5 days, P = .51) and had similar weights (1.8 ± 1.1 kg versus 2.4 ± 2.2 kg, P = .25) when compared with children with ostomies at other sites. NEC was the most common indication for surgery in both groups: 11 (55%) umbilical versus 10 (29%) other. Other indications for surgery included intestinal or colonic atresia (n = 3, 15% umbilical versus n = 8, 24% other), perforation (n = 3, 15% umbilical versus n = 8, 24% other), and obstruction (n = 3, 15% umbilical versus n = 7, 21% other) (Table 1).
Reported as mean (SD).
SD, standard deviation.
In those patients who did not have an umbilical ostomy, the most common site of ostomy placement was the right lower quadrant (n = 21, 61%) with other sites, including the right upper quadrant (n = 9, 26%), left lower quadrant (n = 2, 5%), and midline (n = 1, 2%). In patients with ostomies at other sites 61% (n = 21) had their ostomies placed at the end of their incision. Both groups had a high rate of bowel resection secondary to their underlying pathology with 90% (n = 18) of patients with an umbilical ostomies requiring resection and 82% (n = 28) of patients with nonumbilical ostomies needing resection (P = .45). Patients with an umbilical ostomy had longer segments of bowel resected (17.6 ± 14.5 cm versus 10.4 ± 8.5 cm, P = .03). The most common type of ostomy was an ileostomy in both groups. Operative time did not differ significantly based on ostomy location, although umbilical ostomy patients had a slightly shorter operative time (73.4 ± 33.6 minutes versus 87.3 ± 75.7 minutes, P = .44) (Table 2).
p < 0.05.
Reported as mean (SD).
LLQ, left lower quadrant; RLQ, right lower quadrant; RUQ, right upper quadrant; SD, standard deviation.
Days to stoma output were similar between the two groups [3 (1, 6) versus 2 (1, 5), P = .96], however, days to initiation of feeds were greater in the umbilical ostomy group [15 (9.5, 23.5) versus 6 (4, 10), P = .02]. When comparing only patients who had NEC, days to initiation of feeds were similar between groups [22 (14, 56) versus 15.5 (8, 43), P = .73]. Both groups had postoperative complications with 16 patients (30%) requiring a second operation for these complications. Four (20%) patients in the umbilical ostomy group required an operation for postoperative complications, which included obstruction in three patients and perforation in one patient. Eight (23%) patients in the nonumbilical ostomy group required an operation for complications, including obstruction (n = 3); wound issues, including dehiscence or infection (n = 2); perforation (n = 1); high ostomy output (n = 1); and hernia (n = 1).
Umbilical ostomies had an increase in documented ostomy appliance difficulties [8 (40%) versus 6 (17%), P = .07] and prolapse or peristomal hernias (7 versus 3, P = .01). However, no patient required operative intervention for prolapse or peristomal hernia (Table 3). No patients with umbilical ostomies died during their treatment course, while eight patients in the nonumbilical ostomy group died during their treatment course. The causes of death in the eight patients who died in the nonumbilical ostomy group included seven from sepsis and one from withdrawal of care. Patients were followed until after closure of their ostomy site. There was no difference in time to ostomy reversal between the umbilical ostomy and nonumbilical ostomy groups (112 ± 86 days versus 130 ± 120 days, P = .56). Patients with an umbilical ostomy were followed for longer than patients without [763 (243, 1716) days versus 233 (95, 611) days, P = .001]. There were no hernias reported at the stoma site after take down.
p < 0.05.
Reported as median (IQR).
Reported as mean (SD).
IQR, interquartile range; NEC, necrotizing enterocolitis; SD, standard deviation.
Discussion
Intestinal diversion with ostomies occurs commonly in neonates. With the advent of laparoscopic and minimally invasive techniques, the question of diversion while limiting incisions and subsequent scars has been raised.10,11 Therefore, the optimal position for stoma function, and later cosmetic appearance, has been debated. There is a paucity of literature regarding the use of umbilical ostomies, however, it has been shown to be effective with anorectal malformations,4,5,9 Hirschsprung's disease, 8 and some colorectal disease processes. 12 Our institutional transition from the use of transverse laparotomy incisions to transumbilical incisions has led to an increased use in umbilical ostomies and prompted our review.1,13,14
The umbilicus is an attractive site for ostomy placement due to the lack of an additional incision for ostomy placement as well as a potentially less obvious scar after reversal (Figs. 1 and 2). The ability to improve postoperative cosmesis through usage of the umbilicus has been previously described.9,15 Not only is there an improvement in the aesthetic outcome, there is a demonstrable improvement in patient and parental scar assessment with a decreased number of incisions used during surgery. 16 Finally, avoidance of a transverse lower quadrant incision decreases the regions of the anterior abdominal wall architecture that is violated.
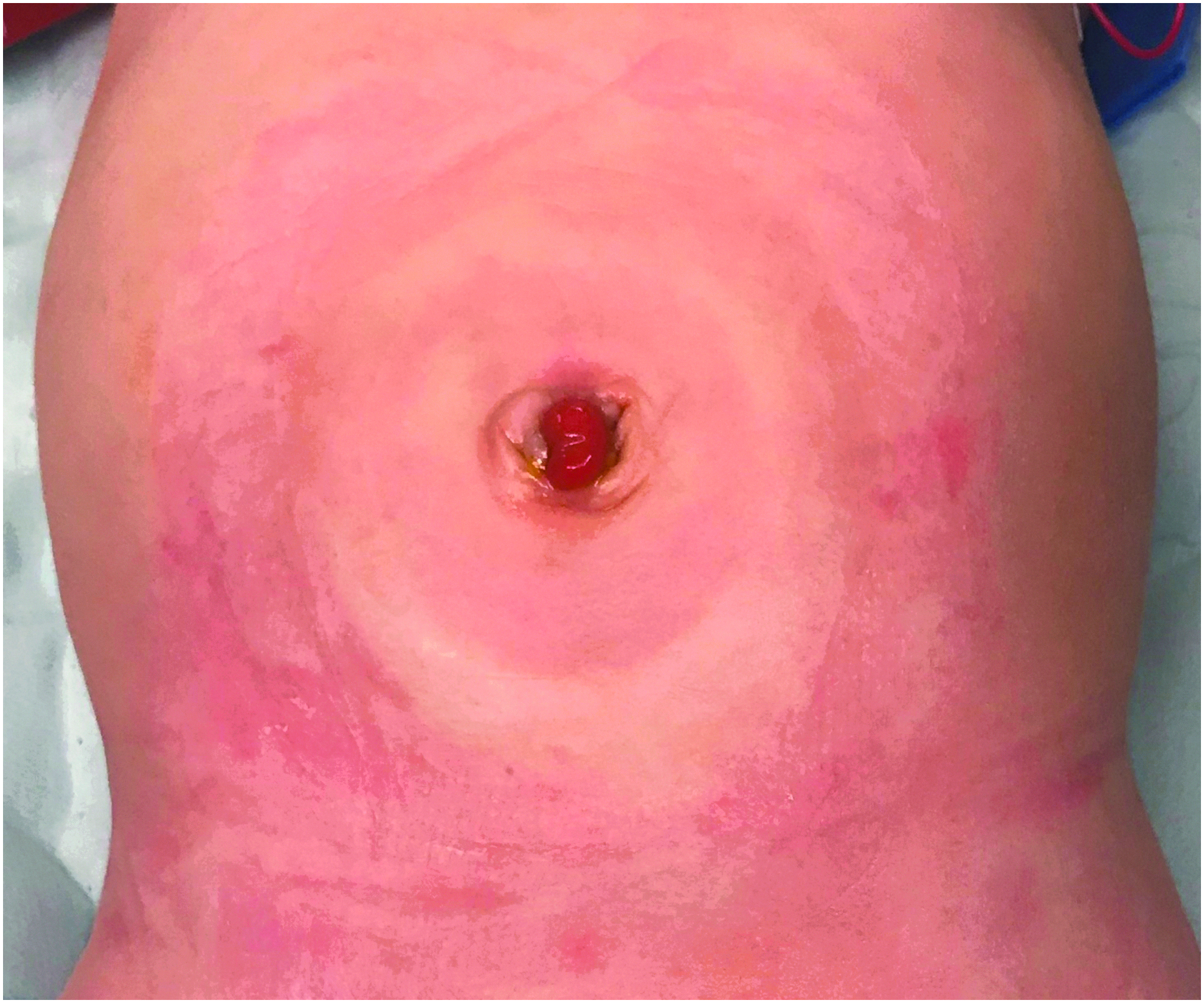
Umbilical leveling colostomy for Hirschsprung disease immediately before reversal.

Umbilical ostomy after reversal and laparoscopic pull-through for Hirschsprung disease, postoperative day 1.
Early experiences in patients with Hirschsprung's disease or high imperforate anus suggested the viability of umbilical ostomies. One study examined 47 infants with umbilical ostomies that included both small and large bowel ostomies. Of these patients, 15 had complications, which included infection, prolapse, retraction, fistula, and stenosis. Seven patients required surgical revision for prolapse and retraction.4,5 The authors concluded that umbilical ostomies are a useful location for temporary ostomies in infants and children. The overall complication rate of 32% in this study corresponds to our finding of a 40% complication rate in patients with umbilical ostomies. However, these series are difficult to directly compare due to their age difference.
More contemporary studies have examined the use of transumbilical colostomy in patients with Hirschsprung's disease, intermediate anorectal malformation (ARM), and high-ARM. While these studies were small with only 4, 7, and 20 patients, respectively, they reported complication rates of 14%–30%, which is similar to our findings.6–8 Another small study examined the use of a temporary diverting ileostomy in the setting of colorectal disease. This study examined 12 total umbilical stomas across 10 patients. The study reported low overall morbidity and excellent cosmesis in the three patients who had stomas reversed. 12
In our study, patients with umbilical ostomies were found to have a higher overall complication rate in comparison to the nonumbilical ostomy patients, but both groups had similar reoperation rates. Previous studies have shown that children operated on for NEC have more stoma complications. 17 Our higher complication rate in the umbilical ostomies group may be due to the fact that they also had a significantly higher rate of NEC. In addition, the umbilical ostomy group had a longer time to initiation of feeds and reaching goal feeds. Similar to the increased complication rate, this may be attributable to the fact that the umbilical ostomies group had a significantly higher number of NEC patients. In our institution, we have a standard seven day period of bowel rest in patients diagnosed with NEC. When comparing only the NEC patients between the umbilical ostomies and nonumbilical ostomy patients, there is no difference in initiation of feeds and reaching goal feeds. The length of bowel resection and the need for jejunostomies were significantly higher in the umbilical ostomy group.
Previous studies indicated that ostomy care at the umbilicus was well tolerated, with multiple studies finding that peristomal skin excoriation was the most common complication of umbilical ostomies.9,12 In our study, patients with an umbilical ostomy had a higher rate of ostomy appliance application issues and ostomy prolapse, but did not require operative correction as a result of this higher rate. The most common ostomy appliance issue in patients with an umbilical ostomy was creating an adequate seal around the umbilicus. Increased experience in the care of these ostomies will most likely decrease this issue. In one case, upsizing the appliance to an adult size achieved a satisfactory seal. At this time, literature on the appropriate method of umbilical ostomy care is sparse. 18
In our study, patients who had an umbilical ostomy had an increase in the rate of ostomy prolapse, however, there was no associated ischemia, obstruction, or strangulation; and therefore, operative stoma revision was not required. The rate of reoperation for stoma complications was similar in the two groups, indicating that although there were increased stoma complications in the umbilical stoma group, they were not clinically significant.
Limitations to our study include the small patient population and the variable length of follow-up. There were eight deaths in the group with ostomies at other sites, while there was none in the umbilical ostomy group. It is unclear from our data what is responsible for this finding; the variety of underlying pathologies as well as the small study population may account for the difference in mortality.
In conclusion, umbilical ostomies are a safe and effective option for neonatal intestinal diversion and may augment the versatility, effectiveness, and improved cosmetic outcome of a transumbilical incision for neonatal exploration.
Footnotes
Acknowledgments
The authors recognize and thank Yara Duran, RN, and Pete Muenks for their contributions as our research coordinators.
Authors' Contribution
J.S., concept and design, data collection, data analysis and interpretation, drafting article, critical revision of article, approval of article, and statistics; H.A., concept and design, data analysis and interpretation, drafting article, critical revision of article, and approval of article; L.A.B., concept and design, drafting article, critical revision of article, and approval of article; J.S., concept and design, drafting article, critical revision of article, and approval of article; S.D.S.P., concept and design, drafting article, critical revision of article, and approval of article; J.D.F., concept and design, drafting article, critical revision of article, approval of article, and statistics.
Disclosure Statement
No competing financial interests exist.