
Abstract
Abstract
Introduction:
Peptic ulcer disease (PUD) is a rare condition in children. Perforated peptic ulcer (PPU), a complication of PUD has an estimated mortality between 1.3% and 20%. We evaluate incidence and outcomes of PPU in children using an administrative database, perform a review of the literature, and report our technique for laparoscopic omental patch repair for PPU in two pediatric patients.
Materials and Methods:
Kids' inpatient database (KID's) was analyzed for demographics, incidence, and outcomes. Incidence for each year was calculated based on the reported pediatric population in the United States for 2000, 2003, 2006, 2009, and 2012 by the U.S. Census Bureau. Additionally, we present two PPU cases, accompanied by a comprehensive review of the literature.
Results:
The annual number of primary discharge diagnosis of PPU in the KID was 178 cases for 2000, 252 for 2003, 255 for 2006, 299 for 2009, and 266 for 2012. An increase trend over time was noted between 2000 and 2009; however, it was not statistically significant (0.05). PPU appears to be more common in Caucasian teenage boys. The mean length of stay was 8.02 days and with a statistically significant increase in healthcare charges ($33,187 versus $78,142, P = .002) when comparing year 2000–2012.
Discussion:
PPU is a rare cause of abdominal pain in children, but still a PUD complication that requires surgery. PPU should be included in the differential diagnosis in patients presenting with acute abdominal pain of uncertain etiology and pneumoperitoneum. Laparoscopy is both diagnostic and therapeutic. Laparoscopic omental patch repair is a safe and effective treatment for PPUs.
Introduction
P
The operative techniques for PPU have been described extensively in the adult population and laparoscopic omental patch repair has become the standard of care. However, the pediatric operative experience has not been described as extensively. To our knowledge, the largest case series for pediatric laparoscopic omental patch repair was published by Wong et al. Their series demonstrated the feasibility of the technique and satisfactory outcomes. 11
Data on demographics, incidence, outcomes, and associated risk factors in children are scarce. A large, multicenter database was used to evaluate the incidence, demographics, and healthcare resource utilization for children with PUD and PPU. Additionally, two pediatric cases of PPU are described highlighting the importance of considering PPU when assessing patients with abdominal pain, pneumoperitoneum, and no identifiable pathology on imaging. A comprehensive review of the literature was performed.
Materials and Methods
Data source
We analyzed data collected as part of the administrative Kids' Inpatient Database (KID), Healthcare Cost and Utilization Project (HCUP), administered by the Agency for Healthcare Research and Quality produces the National Inpatient Sample and its pediatrics-only version, KID. 12 This all-payer database collects annual information from hospital administrative discharge (i.e., billing) records from about 4000 hospitals across 44 states in the United States. These hospitals range in scope from primary to tertiary, university academic to general, and the payer mix is diverse. About 100 data elements (International Classification of Disease, Ninth Revision, Clinical Modification [ICD-9-CM] diagnoses, Current Procedural Terminology codes, demographic and hospital characteristics, discharge status, length of stay (LOS), severity, and comorbidity measures) for each hospital stay are included from the discharge abstract. KID data are available every 3 years between 1997 and 2012 and include a random sample of 80% of other pediatric discharge codes from participating institutions.
Disease definition
International Classification of Diseases, 9th revision Clinical Modification (ICD-9-CM) codes used to identify patients with primary discharge diagnosis of PPU and PUD from the KID data for the years 2000, 2003, 2006, 2009, and 2012 were as follows:
PPU—ICD-9-M codes 531.0X, 531.1X, 531.5X, 532.0X, 532.1X, 532.2X, 532.5X, 532.6X, 533.5X, 533.6X PUD—ICD-9-M codes 531.0X, 531.1X, 5311.2X, 531.3X, 531.5X, 531.7X, 531.9X, 532.0X, 532.1X, 532.2X, 532.3X, 532.4X, 532.5X, 532.6X, 532.7X, 532.8X, 532.9X, 533.0X, 533.1X, 533.2X, 533.3X, 533.4X, 533.5X, 533.6X, 533.7X, 533.9X, V1271
Statistical analysis
For the purpose of this study, patients with ages 0–18 years enrolled in the KID for the years 2000, 2003, 2006, 2009, and 2012 were included. Data were abstracted for demographics, diagnosis of PUD and PPU (only the primary diagnosis was considered), LOS, and total charge on discharge. Data analysis was performed for each edition of the KID. Incidence for each KID year was calculated based on the reported pediatric population in the United States for the years 2000, 2003, 2006, 2009, and 2012 by ChildStats.gov from the United States Census Bureau (data were weighted as per the KID data analysis guidelines). 13 Kendall's tau B test was used to determine statistical significance for incidence trend over years for PUD and PPU. The data analysis was performed using SPSS version 24 (IBM SPSS, Chicago, IL).
Results
The annual number of primary discharge diagnosis of PPU in the KID database was 178 cases for 2000, 252 for 2003, 255 for 2006, 299 for 2009 and 266 for 2012. The incidence of PPU ranged between 0.25 and 0.40, with a steady increase noted from 2000 and 2009. Then incidence from 2009 to 2012 went down (Table 1). Kendall's tau B test was used to test for trend over the years. For PPU the correlation coefficient was 0.80 indicating a strong positive relationship, however, it was not statistically significant (P = .05). For PUD the correlation coefficient was −0.60 indicating a moderately strong negative correlation, but again it was not statistically significant (P = .14).
Sources: HCUP KID. Healthcare Cost and Utilization Project (HCUP). 2000, 2003, 2006, 2009, and 2012. Agency for Healthcare Research and Quality. ChildStats.gov. Child population: Number of children (in millions) ages 0–17 in the United States by age, 1950–2016 and projected 2017–2050. ChildStats.gov.
PUD, peptic ulcer disease; PPU, perforated peptic ulcer.
The mean and median ages for a discharged child with a principal discharge diagnosis of PPU were 15.7 years and 17 years, respectively. PPU presented most commonly in Caucasian (50%) men (76%). The majority of patients were between 16 and 20 years of age. The mean length of stay for PPU was 8.02 days. The mean hospital charge per hospitalization was $53,137 (Table 2). There was a statistically significant increase in healthcare charges ($33,187 versus $78,142, P = .002) when comparing year 2000–2012.
Sources: HCUP KID. Healthcare Cost and Utilization Project (HCUP). 2000, 2003, 2006, 2009, and 2012. Agency for Healthcare Research and Quality. ChildStats.gov. Child population: Number of children (in millions) ages 0–17 in the United States by age, 1950–2016 and projected 2017–2050. ChildStats.gov.
LOS, length of stay; KID, kids' inpatient database; SD, standard deviation.
Case Reports
Case 1
A 16 year-old male presented with 1 day of severe abdominal pain and nonbloody, nonbilious vomiting. The pain was initially periumbilical and eventually migrated to the right lower quadrant (RLQ). The pain continued to worsen, prompting the patient to seek medical attention. Past history was significant for a right humerus fracture following a motor vehicle accident 3 months earlier. On initial evaluation the patient had a history of unsupervised ibuprofen use secondary to the humerus fracture. Physical exam demonstrated RLQ tenderness with guarding and rigidity and leukocytosis of 23,000/μL. Abdominal computed tomography (CT) scan demonstrated per outside report pneumoperitoneum. Diagnostic considerations included ruptured appendicitis versus bowel perforation. The decision was made to proceed with diagnostic laparoscopy.
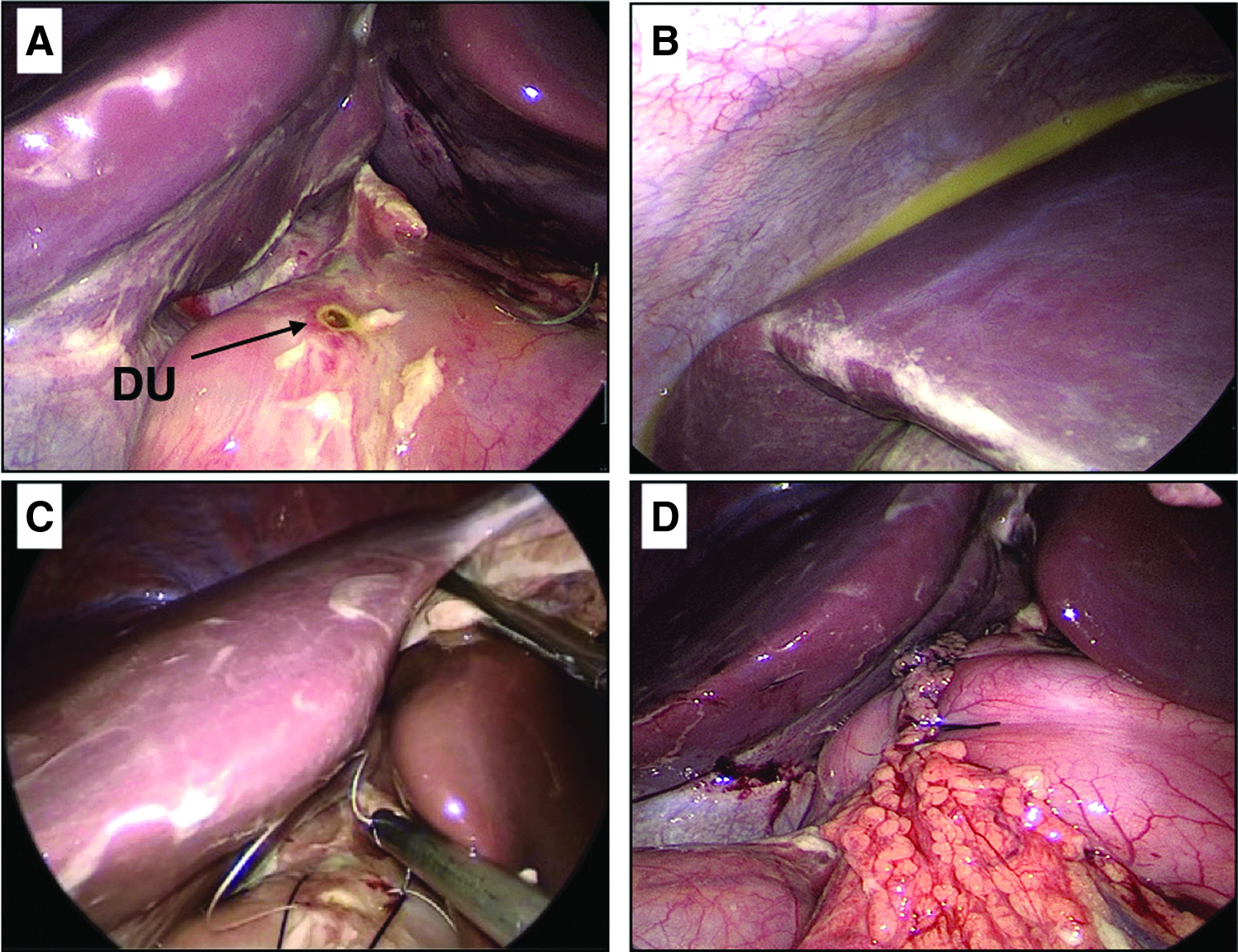
Upon accessing the abdomen, diffuse fibrin purulent peritonitis was noted, and ∼500 mL of pus was aspirated. The cecum and appendix were both mildly inflamed, but no perforation was identified. Appendectomy was performed. The small bowel was evaluated over its entirety; diffuse inflammation was identified, however there was no evidence of perforation or anatomic abnormality. Upon further inspection of the upper abdomen, bilious drainage was noted under the left lobe of the liver, anterior to the lesser curvature of the stomach. A 5 mm perforated ulcer was found at the anterior aspect of the first portion of the duodenum. A laparoscopic Graham (Omental) patch repair was performed. One figure-of-eight suture with 3-0 vicryl was placed to approximate the edges of the perforated ulcer. A pedicle of omentum was placed without tension over the partially closed perforation and stitched in place with five interrupted 3-0 silk sutures (Fig. 1). A closed suction drain was placed through the right upper quadrant port site and positioned anterior to the repair.
The postoperative course was unremarkable. An upper gastrointestinal series was obtained on postoperative day 3 without evidence of leak, the diet was advanced, and the patient was discharged home on postoperative day 5 following removal of the drain. He was discharged on a proton pump inhibitor and oral antibiotics. His H. pylori antibody was negative and H. Pylori antibiotics discontinued as outpatient. The patient followed up in clinic 4 weeks postoperatively and was tolerating regular diet, and had resumed normal activities.
Case 2
An otherwise healthy 16 year-old male presented with a 10 day history of abdominal pain. He previously sought medical attention, however, all evaluations were negative though he was provided with a prescription for ketorolac. His pain was sharp, located in the left lower quadrant (LLQ), and exacerbated by eating. He experience some relief with defecation and emesis. He reported nausea and chills, and denied any fever or emesis in the last 24 hours. He had taken ibuprofen several times for his pain and noted some improvement. CT scan of the abdomen demonstrated free intraperitoneal air and inflammatory changes in the second and third portions of the duodenum (Fig. 2). The appendix was noted to have slightly thickened walls, and there was moderate free fluid in the pelvis. The decision was made to proceed with diagnostic laparoscopy.
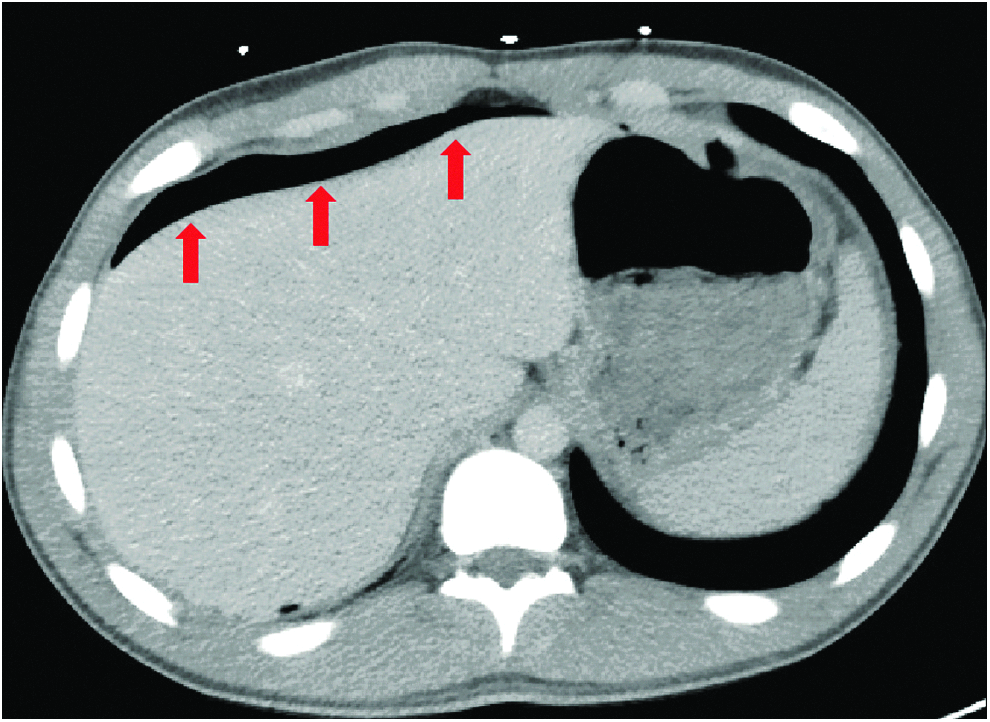
Computed tomography of the abdomen demonstrating intraperitoneal free air consistent with perforation. The red arrows indicate the location of intraperitoneal free air.
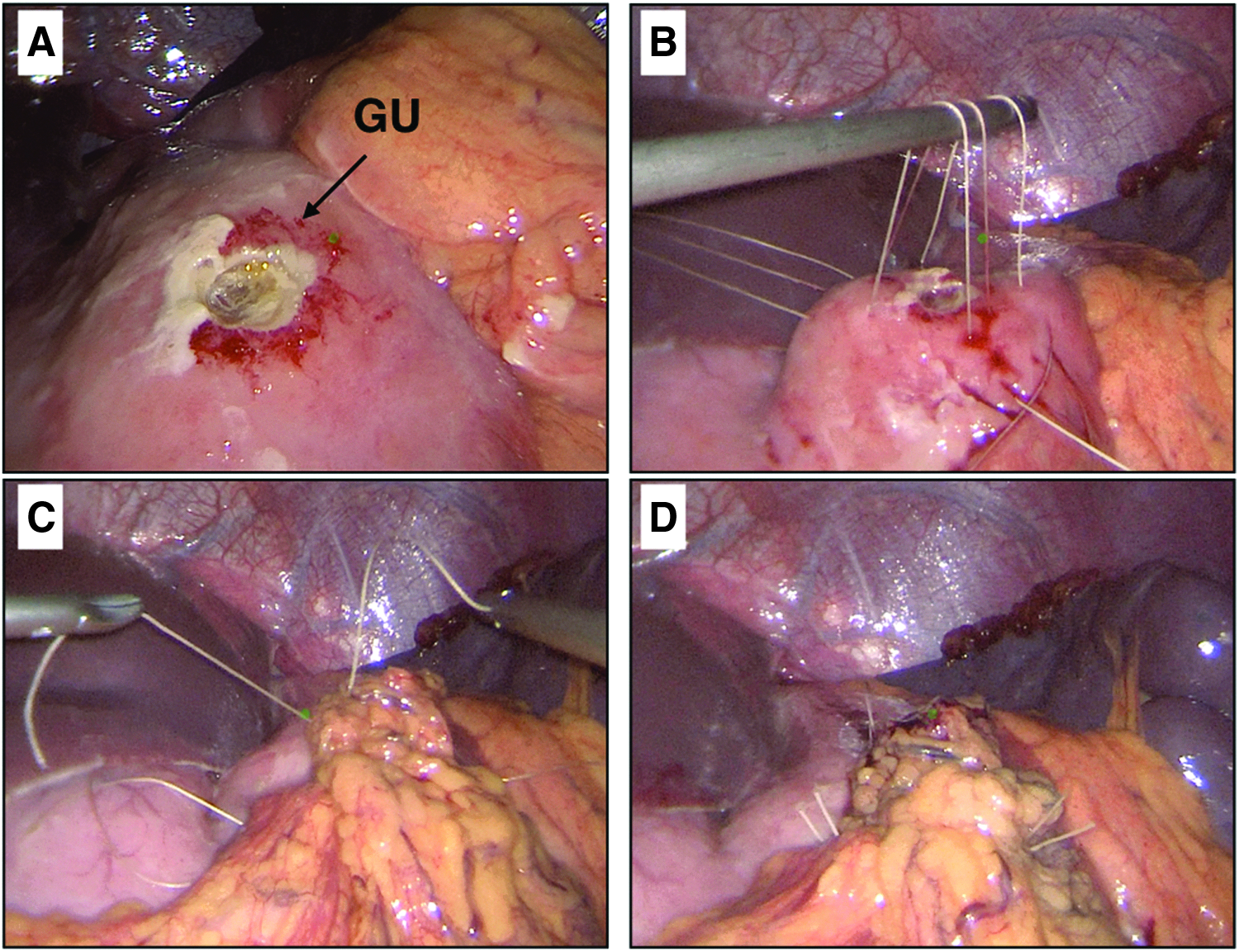
Upon visualization of the abdomen, purulent fluid was noted around the liver and stomach, and murky fluid was noted in the pelvis. There appeared to be an inflammatory process occurring around the right lateral portion of the gastrocolic ligament. The hepatic flexure was mobilized to expose the duodenum. There were no inflammatory changes noted in the first and second portions of the duodenum. The lesser sac was entered, and the third and fourth portions of the duodenum were visualized and no evidence of inflammation. The entirety of the small bowel from the terminal ileum to the ligament of Treitz was examined without evidence of inflammation or perforation. The entire colon was examined without evidence of additional inflammation. The liver was elevated off the stomach. The omentum was adhered to an area of the anterior surface of the stomach along the greater curvature. When the omentum was mobilized, a focal 5 mm perforation was revealed. The defect was repaired with a Graham patch. Three sutures of 3-0 vicryl were placed across the perforation, and the omentum was placed under the stitches and secured (Fig. 3).
The patient tolerated the procedure well and there were no complications. The postoperative course was unremarkable and the patient was discharged on postoperative day 5 on a regular diet. He was discharged with a treatment regimen for H. Pylori with proton pump inhibitor, amoxicillin, and clarithromycin for 14 days. His H. pylori antibody was negative and antibiotics were discontinued as outpatient.
Discussion
PUD has an annual incidence rate of 1.5%–3% worldwide though data specific to the pediatric population is limited. PUD is a rare clinical condition in children. PPU is a serious complication of PUD with an estimated overall mortality between 1.3% and 20%. 14 A 2008 study from the United States reported an incidence of bleeding pediatric peptic ulcer cases of ∼4.4 per 100,000 patients. 15 Recently, there has been an increase in pediatric cases of both PUD and PPU3,4,6,16 with more cases attributed to non-H. pylori related and secondary causes. 16 Using the KID, we were able to estimate the total number of primary discharge diagnosis of PPU was 178 cases for 2000, 252 for 2003, 255 for 2006, 299 for 2009 and 266 for 2012. An increase trend over time was noted between 2000 and 2009, although a small drop was noted in 2012. We speculate that the increased incidence of PPU/PUD could be related to improved critical care outcomes with increased survival of sicker and sicker patients, and possibly use of unsupervised over-the-counter medications.
This disease appears to be more common in teenage boys of Caucasian background. The mean length of stay for PPU was 8.02 days and with a statistically significant increase in healthcare charges ($33,187 versus $78,142, P = .002) when comparing year 2000–2012.
Both of the cases discussed in this report presented to the emergency room with abdominal pain, which is the most commonly reported symptom of a PPU in adults. 14 Our patients' abdominal pain was localized to either the RLQ or LLQ with their respective CTs demonstrating free air under the diaphragm. Given the increased incidence of PUD and PPU in children, this condition will continue to challenge many surgeons across the globe due to its rarity and vague clinical presentation. A study from Taiwan examining data from pediatric Emergency Room visits in a 6 month period of patients presenting with RLQ pain found one case of PPU among 100 cases. 17 Despite the rarity of PPU, this report highlights the importance of a thorough evaluation, including diagnostic laparoscopy. PPU should be included in the differential diagnosis in pediatric patients with abdominal pain, pneumoperitoneum, and no signs of other common diseases on imaging, since patients with PPU in most cases will require surgery. 18 The first case presented with RLQ pain and concerns for perforated appendicitis, but was ultimately diagnosed with PPU. This is consistent with the rare clinical presentation of Valentino Syndrome.
Valentino Syndrome, a rare clinical occurrence within the spectrum of disease of PPU, occurs when patients develop a perforated duodenal ulcer, but have symptoms of acute appendicitis and are therefore frequently misdiagnosed. The RLQ pain seen in Valentino Syndrome is attributed to retroperitoneal perforation of a duodenal ulcer.19,20
Although PPU is an uncommon cause of abdominal pain in children, a retrospective chart review demonstrated that the most common location for the perforation was in the duodenum (78% of cases), mainly on the anterior wall. 4 PPU, which encompasses gastric and duodenal perforation, is a medical emergency and as such timely treatment is of utmost importance.
Both patients reported use of NSAIDs before the onset of their clinical presentation. Though information on frequency and length of intake was not available, ibuprofen was used by both patients with additional consumption of ketorolac in the second case. The association between NSAID use and GI injury is well studied and documented in the adult population and though the data is scarce, there are studies that have shown a similar association in children.19–22 NSAIDs inhibit cyclooxygenase (COX1 and COX2) thereby diminishing the production of prostaglandins that have been shown to play an important role in maintaining the integrity of gastric mucosa. 23 A long-term, prospective study showed a relative risk of 4.8 (P = .09) for gastroduodenal injury in children with reported NSAID use. The symptom of abdominal pain is present in these children twice as frequently as children without NSAIDs ingestion. 9 Numerous studies have found ibuprofen to be commonly associated with peptic ulcers and perforations. Even the short-term use showed GI related adverse effects.8,9,24 See Table 3 for a review of the literature of the reported pediatric cases of perforated duodenal ulcer.
R
CBC, complete blood count; CT, computed tomography; DC, discharge; FH, family history; NSAIDs, nonsteroidal anti-inflammatory drugs; LLQ, left lower quadrant; LOS, length of stay; LUQ, left upper quadrant; PMH, past medical history; POD, postoperative day; PUD, peptic ulcer disease; RLQ, right lower quadrant.
Omental patch repair is considered one of the safest options for surgical management of an acutely PPU. Although laparoscopic omental patch repair has been described extensively in the adult population, the pediatric literature is limited to case series. Wong et al. published a case series highlighting two of the main advantages of laparoscopic approach: first, the advantage of pathology identification when there is uncertainty of the diagnosis, along with the avoidance of misplacing an abdominal incision. 11 Reusens et al., published a 5 patient case series with good results and they advocate for laparoscopic repair with omental patch as the standard for PPU in children. 25
Unclear clinical presentation and the difficulty of diagnosing PPU in children led to delay of treatment in 1 of our patients before being transferred to our facility. Delayed surgical intervention (>12 hours) are associated with greater complications.4,26 Fortunately, diagnostic laparoscopy was performed in both cases revealing PPU in both cases leading to Graham patch repair with uneventful postoperative outcomes.
Conclusions
PPU is an uncommon cause of acute abdominal pain in the pediatric population, however the incidence is increasing. It should be included in the differential diagnosis in patients presenting with acute abdominal pain of uncertain etiology and pneumoperitoneum. Laparoscopy is both diagnostic and therapeutic. Laparoscopic omental patch repair is a safe and effective treatment for PPUs.
Footnotes
Acknowledgment
The authors would like to acknowledge Paula Buchanan, MPH, PhD, from the Center of Health Outcomes Research at Saint Louis University for his assistance with the statistical analysis.
Disclosure Statement
No competing financial interests exist.