
Abstract
Abstract
Background:
Pectus excavatum and carinatum are two of the most commonly observed chest wall deformities in pediatrics. The standard diagnostic evaluation for these conditions includes either chest radiograph (CXR) or computed tomography (CT). Our research aims to develop a novel and reliable way of quantifying chest wall deformities in the clinic setting without radiation exposure.
Methods:
Using a handheld structured light scanner, we created three-dimensional (3D) models of patients with chest wall deformities through an IRB-approved protocol. Raters from a variety of backgrounds were then asked to take measurements based on the 3D model utilizing commercially available 3D graphical software. The standard deviation of the measurements and intraclass correlation coefficient (ICC) were then calculated to quantify inter-rater reliability.
Results:
Sixty patients with pectus excavatum (Haller index range 2.0–6.38) and pectus carinatum were enrolled and imaged in our outpatient clinic using a structured light scanner. Five patients were used to verify interuser reliability. The standard deviation of all the measurements was 2.2 mm. The ICC for absolute agreement was 0.99139, with 1.0 being perfect correlation.
Conclusion:
Structured light scanners provide an alternative approach to quantifying chest wall deformities in pediatric patients without radiation exposure. Our method is highly reliable, even among users with minimal image processing or 3D modeling experience. Our protocol can potentially be used to track treatment progress in children with chest wall deformities.
Introduction
P
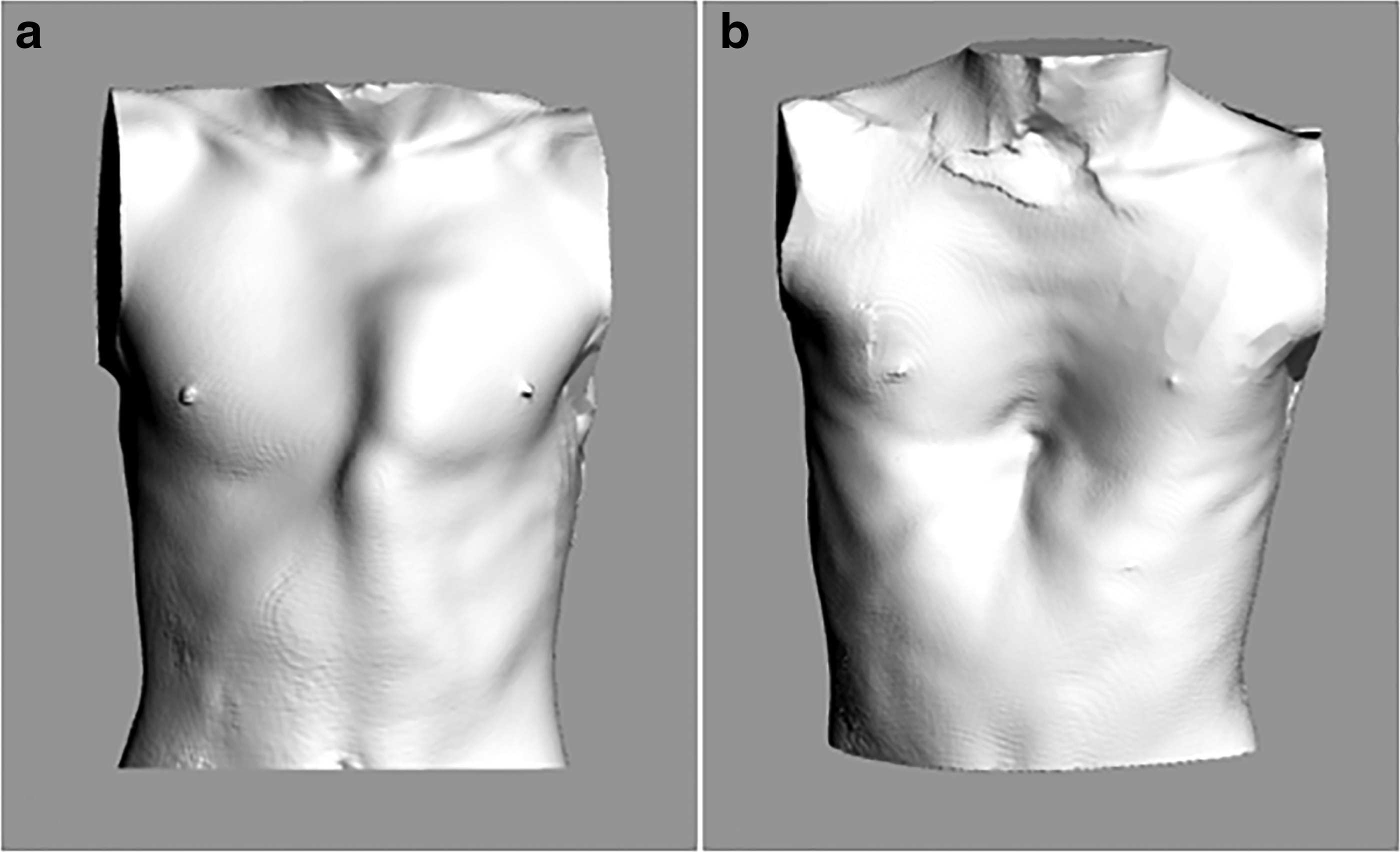
Three-dimensional optical image model of
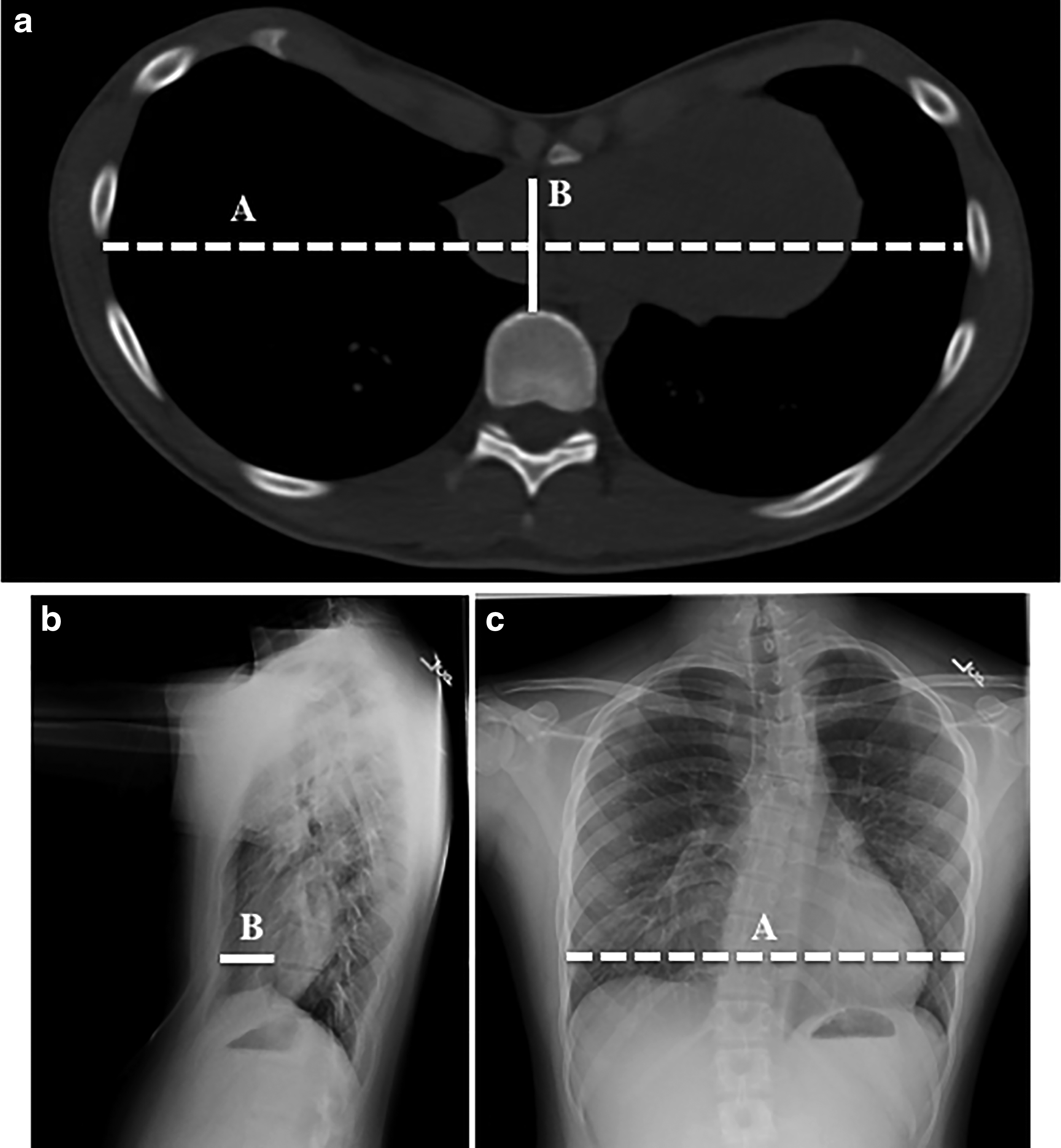
The Haller index, calculated from
These measurements have been traditionally obtained from computed tomography (CT), although the cost and radiation exposure of serial CT scans have made it impractical for serial monitoring. Recent studies have shown that lateral and PA chest radiographs (CXR) can provide the same information with much lower radiation exposure. 4 However, the advent of portable three-dimensional (3D) optical scanning technology presents an opportunity to image patients without ionizing radiation. Although similar methods have been attempted in the past, improvements in technology have now made 3D optical imaging more feasible and advantageous. 5
This study seeks to describe our method of using a 3D structured light scanner and commercially available software to effectively capture and process chest wall images in the clinic. This method of scanning uses cross-sections of the chest to obtain transverse and PA chest measurements. We also aim to show that our method is reliable and reproducible among various users.
Methods
Equipment
Scans were obtained using the Artec Eva (Artec 3D, Santa Clara, CA) (Fig. 3). The Artec Eva is a handheld structured light scanner that is commercially available. Structured light scanners, such as the Artec Eva, operate by projecting a grid onto an object and then analyze the pattern distortion on the object's surface to identify a series of points by which to orient itself. Triangulation is then used to determine the distances between points on that grid to reconstruct the object as a digital mesh. Image quality can be achieved with precision to a resolution of 0.5 mm.6,7

The Artec Eva is a handheld structured light scanner that is able to identify up to 2 million points per second. 7
Scanning subjects
Under an IRB-approved protocol, patients with pectus excavatum and pectus carinatum were enrolled during their routinely scheduled clinic visit. Demographic and clinical data were obtained from participants, including any previous treatment for chest wall deformities or traditional measurements such as the Haller index. Patients removed any clothing covering their torso and stood with best posture, while holding their arms slightly abducted. The scanner was moved at a gradual and consistent pace around the patient and the machine was kept at optimal distance from the subject, as calculated by the accompanying software.
Image processing
Scans were edited using the Artec Eva's accompanying software, Artec Studio 12 Professional (Artec 3D). In the event that the Artec Eva momentarily lost tracking while the scan was being obtained, multiple scan files were aligned before commencing postprocessing. The 3D model was further refined using algorithmic tools within the software to (1) resolve image frames into a single coordinate system and (2) fuse the images to create a model composed of a single surface. Next, editing tools embedded in the software program were used to manually isolate the torso by removing identifying or extraneous features (e.g., face, extremities).
Image analysis
After processing, the scans were segmented and measured using the computer-aided design software Rhinoceros (Robert McNeel & Associates, Seattle, WA). Scans were oriented with the subject in the upright, standing position. The point of maximal depression (for pectus excavatum) or maximal protrusion (for pectus carinatum) was visually identified by the user, referencing the four viewing angles within the program.
A horizontal plane was created at the height of maximum deformity and axially bisected the 3D image of the model. The edges of both of these halves were duplicated using a premade function within Rhino (Fig. 4). This function produced two closed curves that matched the edge of the model at the cross-section where it was cut.
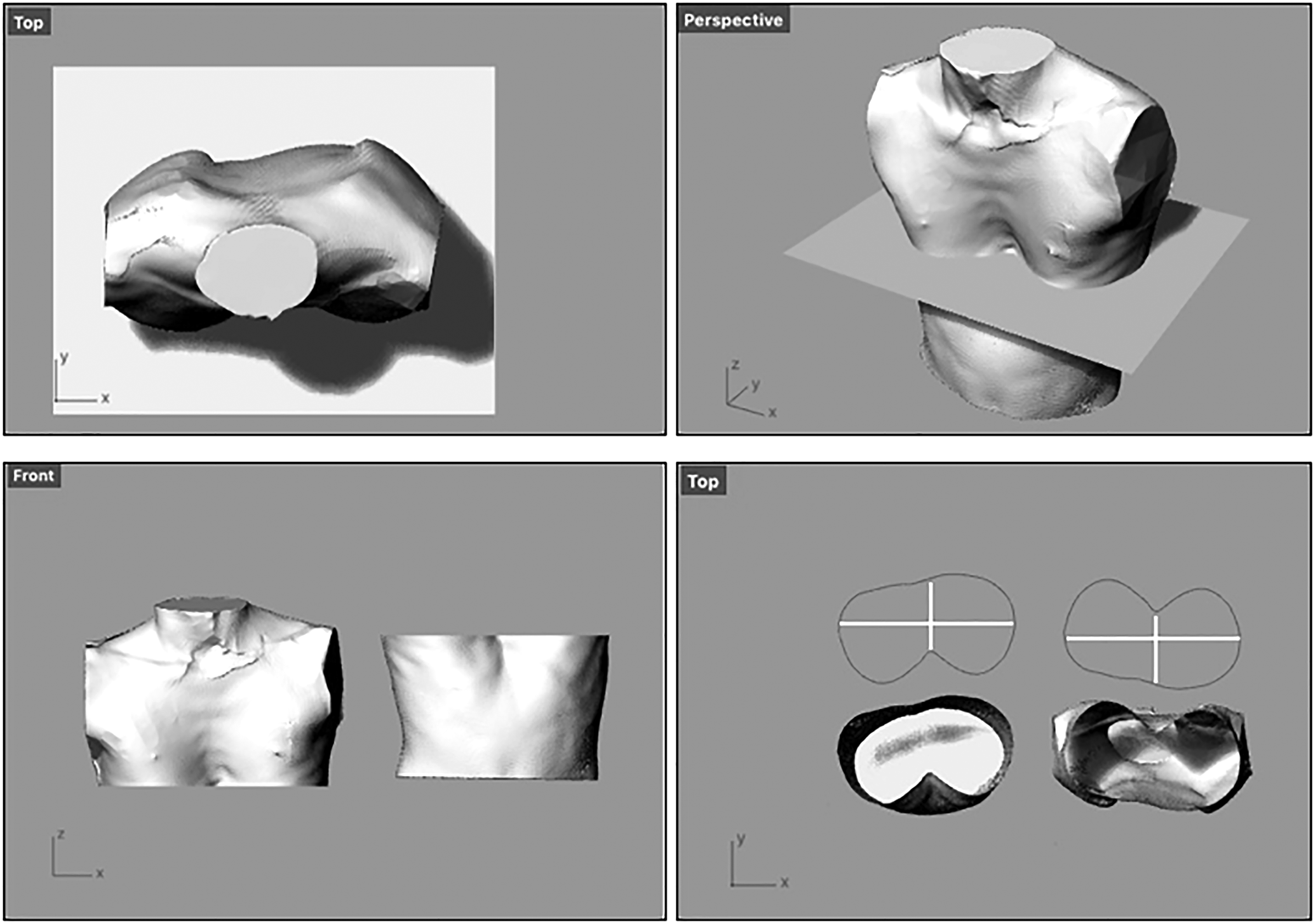
A cross-section of the three-dimensional torso model at the point of maximal deformity; the plane is used to measure the lateral and PA dimensions. These measurements define the optical index. PA, posterior–anterior.
Initially, we asked users measure transverse and PA distances through the plane of maximal deformity. Each distance was measured twice; once on the border from the upper half of the torso and once on the border from the lower half of the torso. The duplicate measurements acted as internal validation for user consistency.
Verifying interuser reliability
Users from various backgrounds (clinicians, researchers, and administrative staff) were asked to complete the above measurements and record the optical index (OI) for several subjects. We defined the OI as the skin-to-skin transverse distance across the chest divided by the skin-to-skin PA distance from the point of deepest deformity (Fig. 4). Each user made four separate measurements per subject. Intraclass correlation coefficient (ICC) was used to judge interuser reliability of the method.
Measurement automation
We automated the measurement process by exporting the closed curves into MATLAB (The Mathworks, Inc., Natick, MA) as binary matrices. At each x-value, the program calculates the distance between the upper and lower bounds of the curve in the y-direction. It iterates along the entire x-axis and then returns the maximum or minimum distance (depending on whether the patient's condition is pectus carinatum or pectus excavatum, respectively) and the x-value that it occurs at. The same process is performed along the y-axis, to retrieve the maximum transverse distance and the y-value at which it occurs.
Results
Sixty patients were enrolled from our clinics. Patients had an average age of 12.7 ± 4.2 years (range 4–29 years). The vast majority of patients were male (91.6%). Patients were evenly split between pectus excavatum (n = 30) and pectus carinatum (n = 30). Of those with pectus excavatum, 28/30 (98.3%) had a radiographic Haller index; 18 patients (60%) had CXR on the same day as their 3D scan, and all but 1 patient had a CXR within a year of their 3D scan. The average Haller index for patients with pectus excavatum was 3.81 ± 1.23 (range 2.0–6.38).
The 60 patients were imaged in clinic without any technical failures. No patients opted out during the scan. Scans took a maximum of 90 seconds to complete in clinic. Postprocessing of the images was performed in less than 5 minutes for each scan, resulting in STL files that contained embedded spatial data that allowed for the measurement of the models. The OI calculation was performed in less than 3 minutes per scan.
Five different users (clinicians, researchers, administrative staff, and students) without any formal training in optical imaging were trained within an hour to both use the scanner and take measurements on the scans. Users performed image processing and measurements on 5 test participants with either pectus excavatum (n = 4, Haller index range 2.40–6.07) or pectus carinatum (n = 1). Each user made a total of 20 measurements; the standard deviation of all the measurements was ±2.2 mm. ICC for absolute agreement was 0.99139, indicating extremely strong correlation.
Discussion
We have presented a straightforward and reliable method for utilizing optical imaging to quantify anterior chest wall deformities without ionizing radiation. Our protocol does not require a large investment of training time or patient time, as a single patient scan can be completed in under a minute and can be done without a physician or professionally trained technician present. This flexibility allows for virtually any clinic staff to operate the scanner in an effort to incorporate this technology into the workflow of a busy clinic environment. At present, procuring the scanner may be cost-prohibitive for individual clinics. However, the cost may be amortized across multiple specialties as more clinical uses are developed for this technology, some of which may become eligible for healthcare reimbursement.
There are several limitations to this method. Our study is somewhat limited in the number of patients evaluated, although we have sufficient data to test the fidelity of our method. This technique provides precise topographic information on chest wall deformities and is suitable for monitoring disease progression or improvements over time; however, it cannot completely replace the diagnostic capabilities of radiographs or CT scans. It will not detect intrathoracic details that can be important for preoperative management, such as compression of the right atrium. Furthermore, the OI does not replicate the Haller index, given that the measurements are taken from external points on the skin, rather than internal ones. Future research will have to investigate how closely the OI correlates to the Haller index, possibly by incorporating patients' biometric data (height, weight, body mass index).
Finally, we demonstrated that multiple users can accurately and consistently use the 3D scans to measure various distances. While this could be useful in patients with pectus excavatum as a way to replace radiographic measurements, it can also be applied toward designing custom-fit compression braces and other devices for patient use. Objective measurements obtained from optical 3D scanning may also enable more uniform and objective measurement of pectus carinatum, rib flare deformities, or mixed deformities in the future.
Conclusion
Commercially available structured light scanners allow patients with pectus carinatum and excavatum to be imaged easily without exposing patients to ionizing radiation. Our technique for quantifying these deformities is reliable, easily integrated into the clinic setting, and does not require specialized training. Future work will include validating our OI against the traditional radiographic Haller index and standardizing processing for other types of chest wall deformities.
Footnotes
Disclosure Statement
The authors have no conflicts of interest related to this research, and no external funding was obtained for this research.