
Abstract
Abstract
Background:
Single-incision laparoscopic surgery has emerged; however, the procedures might be complicated for trainees. We compared the clinical outcomes of conventional three-port laparoscopic appendectomy (CLA) and single-incision and one-puncture laparoscopic appendectomy (SIOPLA) by attending pediatric surgeons (APSs) and surgeons in training (SITs).
Materials and Methods:
We reviewed the clinical outcomes of 72 randomized laparoscopic appendectomies that were consecutively performed by SITs and APSs for a 2-year period. The cases were categorized according to type of surgeon. Finally, 10 CLA and 18 SIOPLA procedures were performed by SITs, and 24 CLA and 20 SIOPLA procedures were performed by APSs. The operative time, blood loss, analgesic use, complications, and hospital stay were analyzed.
Results:
There were no significant differences in any of the evaluation points between CLA and SIOPLA.
Conclusions:
SIOPLA is not inferior operation to CLA, and the postoperative outcomes of SIOPLA were satisfactory. Thus, SIOPLA was safe and feasible for young surgeons to perform.
Introduction
L
We believe that laparoscopic appendectomy is a crucial procedure for inexperienced surgeons, such as junior residents, as it allows them to develop their endoscopic surgical techniques. We adopted a single-incision and one-puncture laparoscopic appendectomy (SIOPLA) procedure in which two ports were introduced through an umbilical wound and one fine puncture port was introduced through the suprapubic region of the lower abdomen to maintain the manipulation angle.
The aim of this study was to compare conventional three-port laparoscopic appendectomy (CLA) to SIOPLA in terms of the clinical outcomes when performed by surgeons with equivalent levels of experience, and to evaluate the safety and feasibility of SIOPLA, when the operation is performed by inexperienced surgeons.
Materials and Methods
Study design
We conducted a randomized prospective study of surgical procedures performed from January 2015 to December 2016. Each operation was performed by 2 surgeons; 2 attending pediatric surgeons (APSs) or 1 APS and 1 surgeon in training (SIT). Surgical procedure (CLA or SIOPLA) was determined at the start of each operation by APS who was an assistant operator independently of operator (APS or SIT). Seventy-two appendectomies (CLA, n = 34; SIOPLA, n = 38) were registered regardless of the disease severity or the surgeon's experience. These surgical procedures were then divided into groups based on the surgeon's experience. In this study, we defined the surgeons' experience as follows: SITs had 1–6 years of experience as a surgeon; APSs had >6 years of experience.
In this study, to compare CLA with SIOPLA, we categorized the groups according to the surgeon's experience. Finally, 10 CLA and 18 SIOPLA procedures were performed by SITs, and 24 CLA and 20 SIOPLA procedures were performed by APSs.
To evaluate the safety and feasibility of CLA and SIOPLA, we compared the outcomes of procedures performed by APSs and SITs.
This study was approved in accordance with the Ethical Guidelines for Clinical Research from the Japanese Ministry of Health, Labor and Welfare. The Research Ethics Committee of Kagoshima University Hospital approved this clinical study (Registration No. 27-119). All of the patients provided their informed consent.
Surgical procedures
The CLA procedure
A 12 mm trocar was placed at the umbilicus using the open access procedure and the abdominal cavity was identified using a 5-mm 30° telescope. The abdomen is insufflated to 8 mmHg with CO2. A 5-mm trocar was placed at the left lower abdominal quadrant, and another 5-mm port was placed at the suprapubic region as working ports (Fig. 1A). The appendix was identified and then grasped by laparoscopic grasper. The mesoappendix was dissected using an ultrasonically activated device (Harmonic ACE plus®; Ethicon Endo-Surgery, Cincinnati, OH). Ligation was performed at the base of the appendix with an ENDOLOOP® (Ethicon Endo-Surgery) and another ligation was performed 1 cm distal from the previous ligation and the appendix was dissected using the ultrasonically activated device.
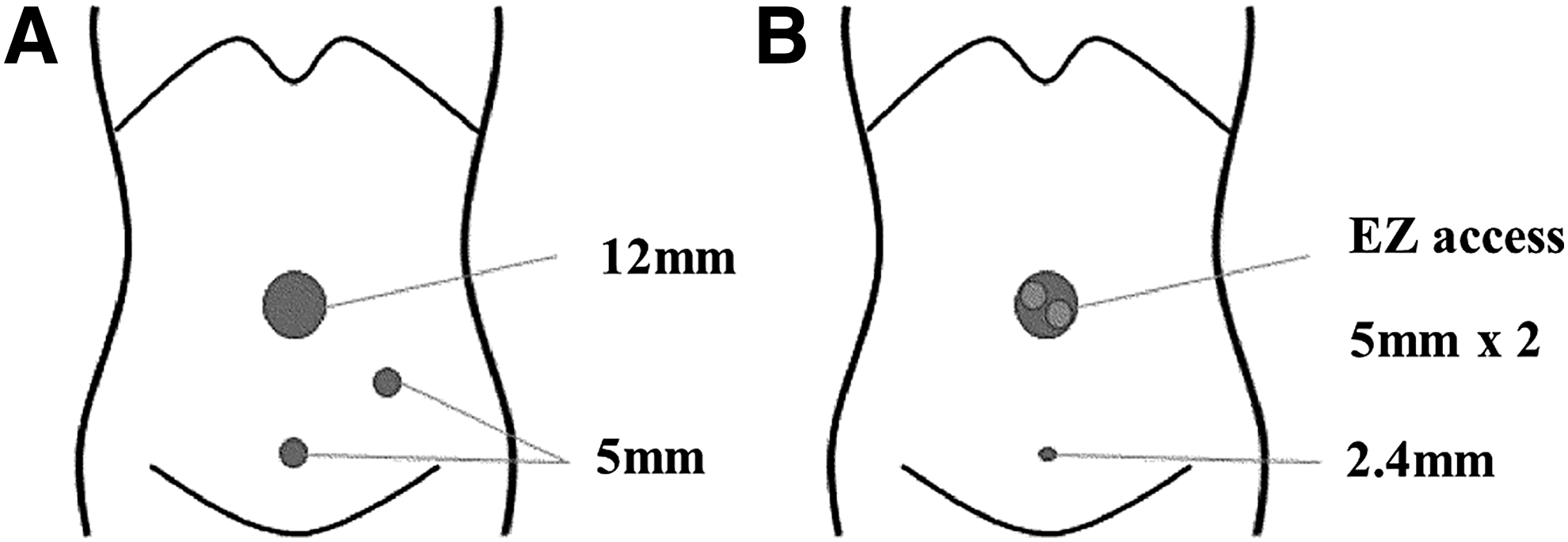
Port layout for CLA and SIOPLA.
The SIOPLA procedure
A 15 mm skin incision was made at the umbilicus and laparotomy was performed; then a Lap-Protector® (size, XS; Hakko Co., Ltd., Tokyo, Japan) was inserted into the umbilical wound and an EZ Access port® (Hakko) was attached. Two 5 mm trocars were inserted through the EZ access port. One trocar was used for a 5-mm telescope and the other trocar was used for a working port. The 2.4 mm percutaneous insertion grasper without the use of a trocar (MiniLap®; Teleflex, Morrisville, NC) was placed using puncture technique at the suprapubic region as a working port (Fig. 1B). Appendectomy was performed using the same procedure as described earlier.
In the case of perforated appendicitis, the abdominal cavity was irrigated using 10 L of normal saline; a drainage tube was not placed.
Statistical analysis
The following factors were evaluated: age at operation, operative time, bleeding, and frequency of analgesic use, postoperative complications, and hospital stay. All data are expressed as the mean ± standard deviation. The chi-squared test, Welch's t-test, and Mann–Whitney U study were used, as appropriate, for the statistical analyses. A P value of <.05 was considered to indicate statistical significance.
Results
The characteristics of the patients who underwent CLA or SIOPLA divided according to the surgeon's type
Table 1 shows the characteristics of the CLA and SIOPLA groups divided according to surgeon's type. There were no significant differences in the characteristics of the patients with the same surgeon's experience. The postoperative complications that occurred included abscess (n = 2; 0.03%), ileus (n = 1; 0.01%), and renal failure (n = 1; 0.01%).
APSs, attending pediatric surgeons; CLA, conventional three-port laparoscopic appendectomy; SIOPLA, single-incision and one-puncture laparoscopic appendectomy; SITs, surgeons in training.
The operative outcomes of CLA and SIOPLA divided according to the surgeon's type
No significant differences were observed in any of the evaluated factors between the CLA and SIOPLA groups when the procedures were performed by surgeons with equivalent experience (Table 2).
APSs, attending pediatric surgeons; CLA, conventional three-port laparoscopic appendectomy; SIOPLA, single-incision and one-puncture laparoscopic appendectomy; SITs, surgeons in training.
Discussion
In our study, no significant differences were observed in any of the points of evaluation between CLA and SIOPLA when the procedures were performed by surgeons of equivalent experience.
In the first report of laparoscopic appendectomy described by Semm, the operation was performed using three trocars (one telescope and two surgical instruments). 1 Recent advances in laparoscopic instrument technology and surgical techniques have led to the performance of SILS, which is associated with reduced wound pain and superior cosmetic results. However, several studies have reported that SILS is associated with a longer operation time in comparison with multiport surgery. 4 SILS is associated with problems such as interference and collision between surgical instruments due to the parallel placement of the scope and the surgical instruments; thus, several studies have suggested that SILS may be difficult for inexperienced surgeons to perform. In our study, however, the operation time of CLA and SIOPLA did not differ to a significant extent when the procedures were performed by surgeons of equivalent experience. One remarkable finding was that there was no significant difference in the operation time of CLA and SIOPLA performed by SITs. In the SIOPLA procedure that we adopted, it is possible to maintain the manipulation angle toward the organ (appendix), and procedure provides a reasonably wide field of view and allows for the use of both hands. Some authors have stated that the preservation of the manipulation angle is of great importance in laparoscopic surgery. 5 The addition of suprapubic port also leads to increased maneuverability of the instruments and better retraction of the appendix. 6
The frequency of analgesic use could be correlated with postoperative pain. Donmez et al. presented that the frequency of analgesic use would be associated with the number and size of the incisions for trocars in laparoscopic surgery. 7 Although the number of trocars was decreased from three to two and the incision size was decreased from 5 to 2 mm in the SIOPLA operation that we adopted, the frequency of analgesic use did not differ to a statistically significant extent between SIOPLA and CLA. Kang et al. showed that SILS did not reduce the frequency of analgesic use due to the increased length of the umbilical incision. 8 Referring to Kang's study, in our study, the frequency of analgesic use when CLA was converted to SIOPLA was not increased.
In this study, the intraoperative blood loss did not differ to a statistically significant extent between CLA and SIOPLA. As the intraoperative blood loss was recognized when the mesoappendix was dissected, the procedure applied in the dissection of the mesoappendix and the devices that are used would be very important. In all of the cases in which SIOPLA was performed in this study, the operators were able to dissect the entire mesoappendix using an ultrasonically activated device (the same as CLA); thus, we did not observe any cases of serious intraoperative blood loss.
With regard to postoperative complications, intraperitoneal abscess and wound infection are the complications that most commonly affect the duration of postoperative hospital stay. In some reports, laparoscopic appendectomy clearly reduced the incidence of wound infection and intraperitoneal abscess in comparison with open appendectomy.9,10 This reduction of infectious complications was definitely observed in cases involving the gangrenous and perforated appendectomy. 11 Referring to these results, the irrigation of the abdominal cavity after the resection of appendix is of great importance. The SIOPLA operation that we adopted could achieve local and wide views with a favorable manipulation angle for surgical instruments the same as CLA. Thus, purulent ascites located in the bilateral hypodiaphragmatic space could be thoroughly irrigated. Since the operation time of SIOPLA for gangrenous appendicitis performed by SITs did not differ to a statistically significant extent from CLA performed by SITs, SIOPLA is considered to be an optimal procedure for severe cases, such as gangrenous or perforated appendicitis.
The hospital stay would be associated with postoperative complications and pain. In this study, there were no significant differences in the incidence of postoperative complications, the frequency of analgesic use, or the length of hospital stay between SIOPLA and CLA. Based on these results, we considered that SIOPLA and CLA achieved the same outcomes.
The incidence of postoperative complications, the frequency of analgesic use, and the length of hospital stay after operations performed did not differ to a statistically significant extent. In this study, experienced expert surgeons were always on hand to supervise CLA and SIOPLA operations performed by SITs. Thus, inexperienced operators, such as SITs, could perform laparoscopic appendectomy safely and satisfactory postoperative outcomes could be obtained. We, therefore, believe that SIOPLA has become an optimal surgical procedure, even for young SITs.
Our study is associated with several limitations. This study was performed in a single institution. The comparisons between SITs and APSs were based only on their experience as pediatric surgeons and not on their previous experience in performing CLA before performing SIOPLA.
Conclusions
In conclusion, SIOPLA was associated with satisfactory postoperative outcomes in comparison with CLA. SIOPLA obtained good postoperative outcomes and was a safe and feasible surgical procedure, even for young SITs.
Footnotes
Acknowledgment
We thank Mr. Brian Quinn for his comments and help with the article.
Disclosure Statement
No competing financial interests exist.