
Abstract
Abstract
Background/Purpose:
Posterior tracheopexy directly addresses membranous tracheal intrusion in severe tracheomalacia (TM). We have previously reported our experience of posterior tracheopexy through open approach in a large series of patients. This study aimed to review lessons learned from our initial series posterior tracheopexy through the video-assisted or robotic video-assisted thoracoscopic approach.
Methods:
We retrospectively reviewed our single-institution experience on all patients who underwent video-assisted or robotic video-assisted posterior tracheopexy for treatment of symptomatic TM between October 2016 and February 2018.
Results:
Ten patients underwent video-assisted (n = 4) or robotic video-assisted (n = 6) thoracoscopic posterior tracheopexy (age range: 8 months–19 years). One patient, the youngest in our cohort, had a type C esophageal atresia repair; none of the other patients had undergone prior thoracic operations. All had symptomatic TM; 1 patient with tracheostomy dependence also had severe distal bronchomalacia, including segmental airways. Postoperatively, patients were hospitalized 3–7 days, with 1–2 days for ICU observation. Improved respiratory symptoms were noted in 9/10 patients following the operation. The 1 patient with preexisting tracheostomy had reduced ventilator dependence but remained hospitalized with ongoing respiratory symptoms.
Conclusions:
The thoracoscopic approach for posterior tracheopexy, while challenging, can be applied to a select cohort of children with severe TM. Thoracoscopic surgery with robotic assistance can eliminate some technical limitations of the video-assisted approach by providing an easier platform for more complicated suturing angles.
Introduction
Tracheomalacia (TM) refers to segmental or diffuse changes of the trachea, which render the airway more susceptible to collapse with changes in pressure or compression by adjacent structures. This condition may extend to one or both mainstem bronchi, which is referred to as tracheobronchomalacia (TBM). The consequences of TM/TBM comprise a broad spectrum of clinical presentations from feeding difficulties, noisy breathing with typical barking cough, and recurrent pulmonary infections, to severe respiratory distress episodes and acute life-threatening events (ALTEs). Airway collapse can occur with anterior vascular compression and/or cartilage shape abnormality, posterior membranous tracheal intrusion, or both leading to TM/TBM. Even though milder cases of TM/TBM may become asymptomatic as the diameter of the airway enlarges with the child, in cases of severe TM/TBM, airway collapse impairs clearance of secretions producing recurrent infections or airway obstruction resulting in ALTEs. When the frequency of infections is high or when ALTEs occur, prompt accurate diagnostic evaluation and more aggressive management is warranted. Airway pathology associated with TM has historically been addressed with aortopexy, and minimally invasive surgery (MIS) techniques for aortopexy are well established.1–5 Aortopexy, which indirectly elevates the anterior wall of the trachea, may not be a sufficient strategy in patients with dynamic airway collapse caused by posterior intrusion of the membranous component. Our Esophageal and Airway Treatment (EAT) Center has a growing experience with posterior tracheobronchopexy to address posterior membranous intrusion directly with a significant improvement in respiratory status.6–8 We have recently incorporated minimally invasive and robotic techniques into our operative approach for select cases. This study aimed to review lessons learned from our initial series of MIS posterior tracheobronchopexy.
Methods
Patients
After approval of study protocol by the Institutional Review Board (IRB-P00021702), a retrospective review was performed for all patients suffering from severe TM/TBM who had undergone video-assisted or robotic video-assisted thoracoscopic posterior tracheopexy at Boston Children's Hospital between October 2016 and February 2018. Data retrieved included patient demographics, clinical symptoms, bronchoscopic findings, surgical approach, and postoperative course.
Thoracoscopic technique
In the operating room, after semi-prone lateral decubitus positioning and using a bronchial blocker for single-lung ventilation in children older than 1 year, ports were inserted in standard locations for tracheoesophageal surgery. The azygos vein was divided between ligatures, resecting a segment to use as autologous pledget material (Fig. 1). The esophagus was dissected so that it could be pushed either left or right in the posterior mediastinum. The anterior spinal ligament was exposed, pushing fatty tissue, including the thoracic duct toward the left chest (Fig. 2). Posterior tracheobronchopexy was performed by placing autologous pledgeted horizontal mattress sutures' partial thickness into the longitudinal midline portion of the posterior tracheal/bronchial membrane and suturing them to the anterior longitudinal spinal ligament (Fig. 3). Flexible bronchoscopic imaging was continuously displayed to confirm that sutures were not placed intraluminally and that the airways were optimally opened without distortion. Some patients with a wider membranous trachea required two parallel rows of tracheopexy sutures. Finally, the pleura was closed, and the esophagus was rotated either left or right of the trachea, that is, rotational esophagoplasty (Fig. 4). The side to which the esophagus was translated was based on its natural position for each patient, and whether left bronchopexy was necessary (in which case the esophagus was translated toward the right). Rotational esophagoplasty was performed to prevent the esophagus from assuming a position posterior to the trachea, which would contribute to the posterior compression, and also to improve long-term durability of scarring for the tracheopexy.

Azygous vein used for autologous pledgets.
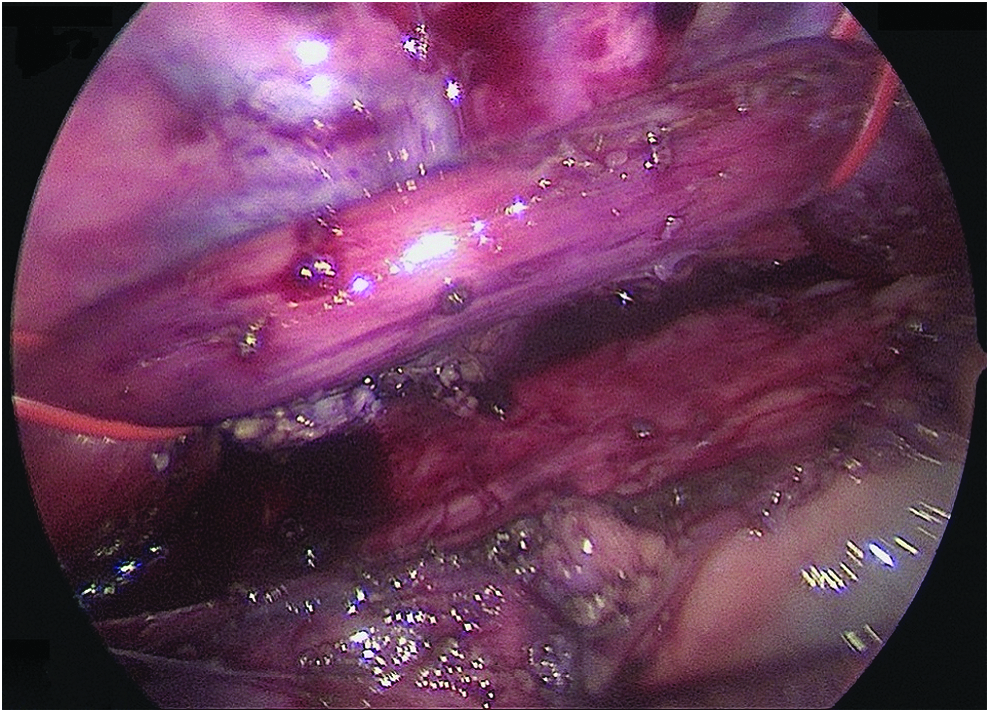
Esophagus suspended, exposing trachea and spinal ligament.

Posterior tracheopexy completed: posterior tracheal membrane secured to anterior spinal ligament.

Pleura closed between trachea and esophagus.
Results
Preoperative data
Ten patients were identified, ranging in age from 8 months to 19 years (Table 1). All patients underwent rigid dynamic bronchoscopy preoperatively to correlate their symptoms with the presence of severe TM/TBM (Table 2). Symptoms included life-threatening events with episodes of profound desaturations, exercise intolerance with increased work of breathing, prolonged cough, and recurrent respiratory infections. One patient with prolonged tracheostomy and ventilation dependence (case 3) was a former 26-week premature infant, who suffered from bronchopulmonary dysplasia and diffuse TBM, including segmental bronchi. Only 1/10 patients (case 2) had a prior type C esophageal atresia repair. All patients had preoperative dynamic airway multidetector computed tomography (MDCT) to evaluate anatomic relationships of the trachea to the esophagus, spine, and vasculature, and to assess for aberrant blood vessels. None of the patients in this series was found to have aberrant posterior subclavian vessels.
Demographics and Clinical Features
EA/TEF, esophageal atresia/tracheoesophageal fistula; ALTE, acute life-threatening event.
Preoperative Bronchoscopic Evaluation
TM/TBM scores based on our standardized bronchoscopic evaluation: scores are percentage of open airway out of 100 for each of five anatomical airway regions; Lower overall score correlates with worse tracheomalacia.
TM/TBM, tracheomalacia/tracheobronchomalacia; RMB, right mainstem bronchus; LMB, left mainstem bronchus.
Intraoperative findings
Of 10 performed thoracoscopic cases, 4 were video assisted, and 6 were robotic video assisted (Table 3). The size of patients for video-assisted cases ranged 5.6–101 kg (mean 30, median 8), whereas the robotic cases ranged 25–73 kg (mean 46, median 42). The patient weighing 101 kg was our very first MIS posterior tracheopexy patient. One patient (case 2) with a prior right thoracotomy required open conversion to achieve the desired precision of suture placement. Operative times ranged from 4.5 to 10.5 hours (mean 7.5). Additional procedures included in operative times consist of rigid dynamic bronchoscopy for all cases, central line placement, tracheostomy removal and temporary closure, and tracheal diverticulum resection. The intraoperative bronchoscopic evaluation showed marked improvement in airway patency of all patients at the conclusion of each case.
Surgical Approach
VATS, video-assisted thoracoscopic surgery; R-VATS, robotic video-assisted thoracoscopic surgery; LMB, left mainstem bronchus; RMB, right mainstem bronchus.
Postoperative course
Patients were hospitalized 3–7 days, with 1–2 days for ICU observation. Long-term follow-up after surgery ranged from 1–16 months (mean 6 months) (Table 4). Follow-up was performed by combination of clinic visits and phone communication for out-of-state patients. Four patients have had follow-up bronchoscopy for ongoing symptoms. The patient with preexisting tracheostomy and ventilator dependence remained hospitalized for over 8 months with a variety of problems, including respiratory. This patient was found to have improved airway patency for the trachea and proximal bronchi, but persistent severe distal bronchomalacia. Three patients required subsequent anterior aortopexy and tracheopexy through ministernotomy to achieve optimal airway patency. In all 3 of these cases, rigid bronchoscopy demonstrated that the posterior tracheopexy remained intact; nonetheless, anterior airway support was still required to prevent symptomatic dynamic anterior airway collapse. One patient (case 1) with BMI of 35 developed a left thigh pressure injury thought to be related to patient positioning during the case that resolved without intervention. One patient required a single esophageal dilation after the posterior tracheopexy for esophageal compression at the level of the thoracic inlet. All patients continue to be followed in our long-term EAT clinic, with plans for routine repeat bronchoscopy at around 1 year and as needed thereafter.
Postoperative Course
Discussion
Our multidisciplinary care team at the EAT Center has made efforts to standardize the diagnosis and treatment of TM/TBM by creating a scoring system based on endoscopic evaluation of the airway anatomic regions.6,7 To determine TM/TBM scores, the tracheobronchial tree is evaluated by anatomical region and percentage of airway patency as noted during multiple types of spontaneous breathing, including gentle, vigorous, and coughing. The degree of open airway was scored out of 100 at each anatomic region: upper, middle, and lower trachea, and right and left mainstem bronchi with a maximum score of 500 (Table 2). Patients with greater severity of airway collapse alongside the presence of severe clinical symptoms are offered surgical intervention. Dynamic airway MDCT provides important preoperative information about aberrant vascular anatomy and intrathoracic structures that may affect surgical planning.9–11 For patients that require surgical intervention, each operation needs to be customized to the airway anatomy obtained from preoperative diagnostic evaluation, including decisions about the desired anatomic relationships of the trachea to the esophagus and major vasculature in cases of aberrant arteries or descending aorta impingement on the left mainstem bronchus. Aberrant posterior subclavian vessels require mobilization, division, and sometimes reimplantation depending on their size and relationship to the affected levels of posterior tracheal intrusion. Descending thoracic aortopexy is sometimes needed for cases of severe left mainstem bronchial compression. We have only addressed these vascular issues by open thoracotomy, and consider these to be exclusions for the MIS approach at this time, although this is certainly open for evolution of the techniques. 8
Previously, our group reported a large series of patients with severe symptomatic TM/TBM who had undergone posterior tracheobronchopexy through open approach, proving bronchoscopic and clinical evidence of improvement in airway collapse. 7 This current series represents our initial experience of performing thoracoscopic posterior tracheobronchopexy through video-assisted or robotic video-assisted approach in pediatric patients with posterior airway intrusion. To our knowledge, this represents the first such series in the literature. We have strongly favored patients without prior thoracic operations for our initial patients to perfect the technique before attempting reoperative cases. We intent to maintain or increase the degree of precision of surgical technique that we utilize for open posterior tracheopexy operations. Minor degrees of imprecision can lead to a distorted airway shape that must be prevented and corrected during the procedure. The simultaneous use of intraoperative flexible bronchoscopy is mandatory to confirm precision of suture placement by providing luminal visualization during suture placement, both for location and proper orientation to the spinal ligament, and to avoid full-thickness sutures. We prefer interrupted autologous pledgeted horizontal mattress sutures for improved scarring with knots tied on the spinal ligament to prevent suture or foreign body erosion into the airway that could lead to granulation tissue or intraluminal bleeding.
The location of the esophagus compared with the tracheopexy is an important issue to consider. It must be moved to the side adequately to make space for the posterior tracheopexy. For patients with a significant component of left mainstem bronchomalacia that require posterior left mainstem bronchopexy, it is generally necessary to dissect and move the esophagus toward the right. We suspend the esophagus proximally and distally after dissection to provide exposure for the tracheopexy during the operation, and then exclude the esophagus from assuming a posterior position compared with the membranous trachea by closing the pleura between them. Care must be taken to avoid compression of the esophagus at the thoracic inlet where space is limited. Our single patient that required esophageal dilation following the operation highlights this issue. The posterior tracheopexy sutures can be placed slightly more leftward on the spinal ligament at this level to accommodate the esophagus. For cases where the left mainstem bronchus is not a problem regarding bronchomalacia, and for which the esophagus is naturally positioned more to the left, the esophagus can be dissected and pushed more leftward in the posterior mediastinum. The pleural closure is not possible between esophagus and tracheopexy for these cases. Esophageal compression at the level of the thoracic inlet has not been an issue when the esophagus is pushed toward the left posterior mediastinum, although concerns about posterior tracheal compression by the esophagus must be balanced in this decision. Longer follow-up will be necessary to look at comparative outcomes regarding rotational esophagoplasty to the right versus the left.
An additional important consideration during the dissection of the posterior mediastinum is to avoid injury to the thoracic duct and recurrent laryngeal nerves. Exposing the anterior spinal ligament to allow secure suturing for the tracheopexy requires that the thoracic duct being mobilized to the left. It does not have to be identified and dissected specifically but is contained within the fatty tissue of the posterior mediastinum just in front of the anterior longitudinal spinal ligament. By dissecting and exposing the spinal ligament, this fatty tissue containing lymph nodes and the thoracic duct can be moved altogether. The left recurrent laryngeal nerve will be encountered during separation of the esophagus and membranous trachea in the thoracic inlet; it is important to avoid excessive (or really any) cautery in this area to prevent inadvertent nerve injury.
Taking all of these points into account, thoracoscopy provides excellent visualization during the dissection and suturing, and can provide an ideal operative approach for successful posterior tracheobronchopexy. We have seen that patients have less postoperative pain, less ventilator dependence, shorter ICU stays, and less hospitalization time compared with open thoracotomy, while maintaining effective improvement in respiratory symptoms in the majority of patients. Further studies comparing the open and MIS techniques will be needed in the future once the MIS techniques are optimally developed. For patients of adequate size, thoracoscopic surgery with robotic assistance can eliminate some technical limitations of the standard video-assisted approach. We currently consider patients over 20–25 kg for the robotic approach, although this number will likely decrease over time. Robotic instruments can articulate in small degree angles, providing a more accessible platform for complicated suturing angles. Also, the robotic system allows for picture-in-picture bronchoscopic guidance, such that the view from the bronchoscope is available to the surgeon on the console in real time. Side-by-side video monitors have been employed for standard thoracoscopic cases thus far to allow the surgeons to see the bronchoscopy and thoracoscopy simultaneously.
It is important to discuss the cases in this series that remained significantly symptomatic and/or required further intervention. Each of these cases had followed up bronchoscopy to further delineate their problems; and in all cases, it was apparent that the posterior tracheopexy scarring remained intact with successful prevention of posterior tracheal intrusion. This illustrates a salient point that we have seen in our open tracheopexy series as well, namely that some patients will have multifactorial airway problems both anatomically and functionally, for which posterior tracheopexy (and even with added anterior aortopexy) cannot solve completely. The patient with severe chronic lung disease of prematurity with tracheostomy and ventilator dependence illustrates that we need to further clarify optimal patient selection for posterior tracheopexy in patients with multifactorial chronic respiratory failure. We have several similar patients in our open posterior tracheopexy series that showed improvement in frequency of ALTEs and ventilator settings, despite ongoing need for a more prolonged ventilator wean. The 3 cases in this series that required subsequent anterior aortopexy represent a subgroup of patients that have been found in our series of open tracheopexy cases as well. A certain percentage of patients will require airway procedures from both posterior and anterior approaches to achieve optimal airway patency. We have seen the best results when the posterior work is performed first to allow adequate scarring of the posterior tracheal membrane before pulling the anterior trachea in the opposite direction with anterior aortopexy and anterior direct tracheopexy.
Conclusions
MIS techniques can be applied safely and effectively for successful posterior tracheobronchopexy in the treatment of TBM. These techniques require extensive experience and expertise with esophageal and tracheal surgery, in addition to MIS expertise. Furthermore, a dedicated multidisciplinary team, including anesthesiologists facile with flexible bronchoscopy, is critical for optimal outcomes. Evaluation for and treatment of additional airway, pulmonary, cardiovascular, and esophageal anomalies, including laryngomalacia, laryngeal clefts, esophageal strictures, vascular rings/aberrant arteries, and chronic lung disease, are commonly necessary for these patients.
Footnotes
Disclosure Statement
No competing financial interests exist.