
Abstract
Abstract
Background:
The standard procedure of lymph node (LN) dissection for rectal or sigmoid colon cancer remains controversial. Many laparoscopic surgeons cut the inferior mesenteric artery (IMA) at the root; however, this may cause bowel ischemia around the site of anastomosis. We performed D3 or D2 LN dissection with the preservation of the IMA. The aim of this study was to evaluate the oncologic outcomes of IMA-preserving LN dissection.
Patients and Methods:
We retrospectively analyzed 142 consecutive patients with upper-rectal or sigmoid colon cancer who underwent laparoscopic LN dissection with the preservation of the IMA. The number of LNs dissected and the overall and disease-free survival rates were retrospectively evaluated.
Results:
Laparoscopic D3 (n = 92) or D2 (n = 50) LN dissection were performed with the preservation of the IMA. The left colic artery was preserved in all cases, the superior rectal artery was also preserved in 30 cases. The mean number of LNs dissected was 19.6 in the D3 group and 12.9 in the D2 group. The median operative time was 230 minutes, and the median volume of blood loss was 17 mL. There was no treatment-related mortality. The estimated 5-year disease-free survival rates of the stage I, II, and III patients were 93%, 83%, and 74%, respectively. No patients developed LN recurrence.
Conclusions:
Laparoscopic surgery with IMA-preserving LN dissection is an oncologically acceptable treatment strategy in patients with upper-rectal or sigmoid colon cancer.
Introduction
L
Many laparoscopic surgeons perform high arterial ligation (at the root of the IMA) mainly due to oncologic considerations and thereby avoid complicated procedures to minimize the operative time. However, high ligation of the IMA may increase the risk of ischemia proximal or distal to the anastomotic site, and may occasionally result in anastomotic leakage or unnecessarily wide resection of the colon, especially in elderly patients.4,6–8
We performed D3 or D2 LN dissection with the preservation of the IMA. In D3 dissection surgery, the LNs around the root of the IMA were completely dissected and the IMA was preserved to maintain a good blood supply to the remnant bowel. A technique for performing laparoscopic LN dissection with the preservation of the LCA or the SRA has been reported9–12 ; however, the oncologic outcomes of these procedures have not been elucidated. The present retrospective analysis was conducted to evaluate the oncologic and long-term outcomes after IMA-preserving laparoscopic LN dissection.
Patients and Methods
We retrospectively reviewed the records of consecutive patients who underwent laparoscopic surgery for upper-rectal or sigmoid colon cancer with D3 or D2 LN dissection at Hokkaido Cancer Center from 2009 to 2015. This study was approved by the hospital's Ethics Committee and informed consent was obtained from all of the patients.
The TNM classification of malignant tumors (7th edition) was used for staging. The grade of LN dissection was determined according to the general rules of the Japanese Research Society for Cancer of Colon and Rectum. 13 D3 LN dissection was applied for patients with clinical T2–T4 or N1–N2 disease, and D2 LN dissection was used for clinical T1 N0 cases. Basically, we intended to preserve the LCA in all patients regardless of whether D3 or D2 dissection was performed. The SRA was also preserved in patients with cancer located in proximal sigmoid colon. In some cases with bulky LNs, the IMA was cut at the root based on the choice of the surgeon. A standard five-port laparoscopic technique was used and the recto-sigmoid mesentery was mobilized by a median approach.11,14 In cases involving D3 LN dissection around the IMA, the fat tissue and nodes between the root of the IMA and the branching point of the LCA were dissected and excised completely, the artery feeding the tumor was tied and cut, and either the LCA was preserved, or both the LCA and the SRA were preserved, depending on the location of the cancer. In the D2 dissection cases, the IMA was identified at the branching point of the LCA, and the artery feeding the tumor was consequently tied and cut to preserve the LCA or both the LCA and the SRA. (Fig. 1) The majority of the patients underwent multidetector computed tomography (MDCT) preoperatively, and 3D images of the IMA and the inferior mesenteric vein (IMV) branches were obtained.
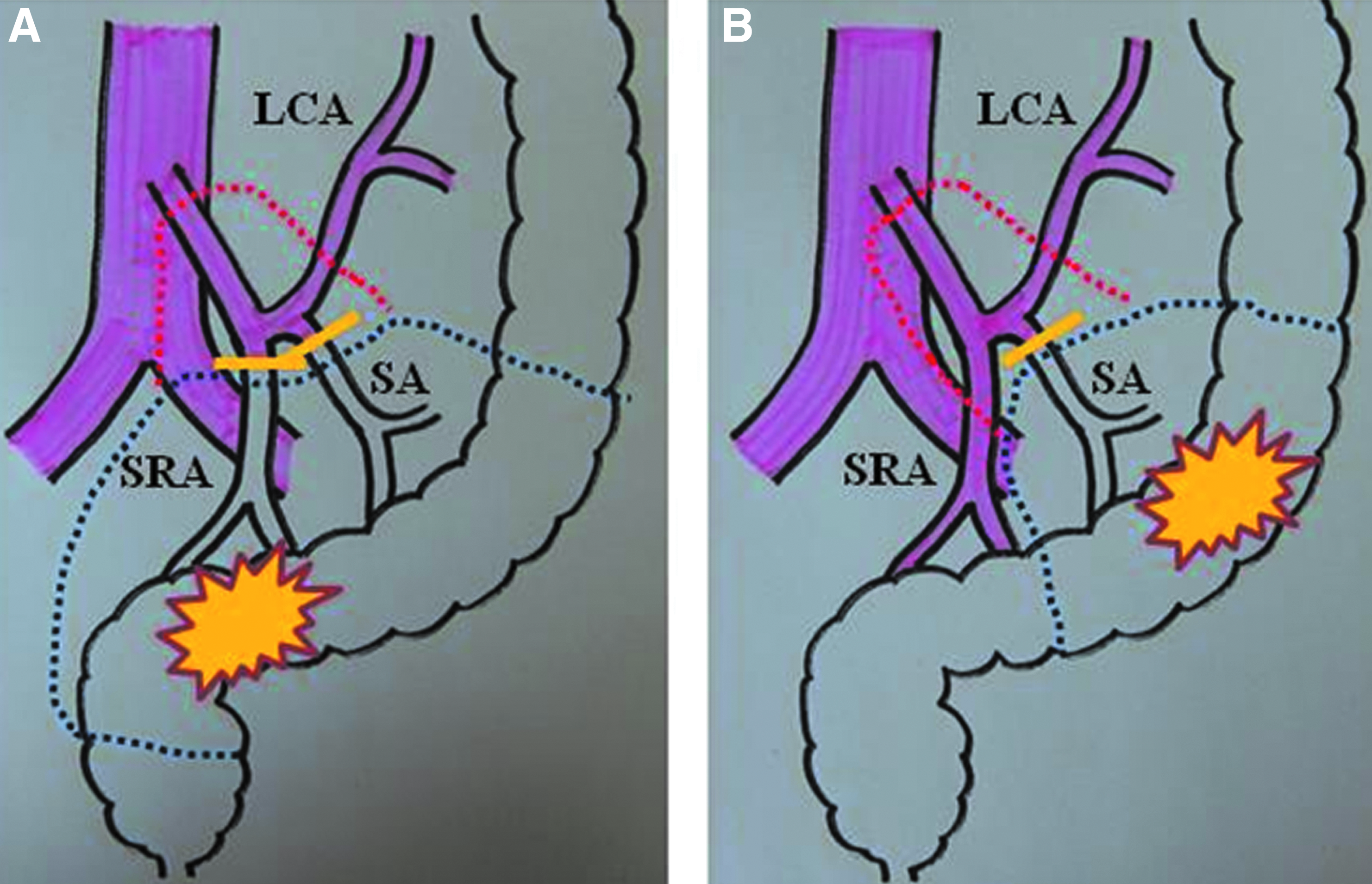
Diagram of LN dissection with preservation of the IMA for upper-rectal or sigmoid colon cancer.
To assess the oncologic and long-term outcomes, the number of harvested LNs, the overall and disease-free survival rates, and the patterns of recurrence were evaluated. The overall and disease-free survival curves from the date of the operation were estimated using the Kaplan–Meier method, and were analyzed using the log-rank test. Fisher's exact probability test and Student's t-test were also used. P values of <.05 were considered to indicate statistical significance. All statistical analyses were performed using the EZR statistical software program. 15
Results
Between 2009 and 2015, 190 consecutive patients underwent laparoscopic surgery for upper-rectal or sigmoid colon cancer. Forty-eight patients were excluded from this study for the following reasons: stage IV disease (n = 20), the IMA was cut (n = 19), only D1 LN dissection was performed (n = 5), and a diagnosis of mucosal cancer (pTis) (n = 4). Consequently, a total of 142 patients with stage I–III upper-rectal or sigmoid colon cancer who underwent D3 (n = 92) or D2 (n = 50) LN dissection preserving the IMA were included in the study population. Preoperative MDCT was performed in 134 patients, and 3D images of the IMA and the IMV branches were obtained.
The baseline clinical characteristics of the patients are shown in Table 1. Tumors were located in the sigmoid colon (n = 74), rectosigmoid (n = 35), and upper rectum (n = 33). Forty-four patients (31%) had pathologically proven LN metastasis, and 69, 29, and 44 patients were diagnosed stage I, II, and III diseases, respectively. No patients had pathologically positive LNs around the IMA. Patients with LN metastasis subsequently received adjuvant chemotherapy (UFT+leucovorin or FOLFOX).
LN, lymph node.
The operative procedures and the short-term outcomes of laparoscopic surgery with IMA-preserving LN dissection are shown in Table 2. The operative procedures included sigmoidectomy or high anterior resection (n = 107), low anterior resection (n = 34), and Hartmann's operation (n = 1). As for LN resection, 92 patients underwent D3 dissection and 50 patients underwent D2 dissection. The IMA and LCA were preserved in all of these patients, and the SRA was also preserved in 30 patients. The median operative time was 230 minutes (range, 105–545 minutes), and the median volume of blood loss was 17 mL (range, 0–310 mL). One patient required conversion to open surgery due to dense adhesion in the pelvis. There were no cases of treatment-related mortality. The postoperative morbidity rate was 19.7%, and reoperation was required in 4 patients (2.8%) who developed anastomosis failure.
Values are range and median.
IMA, inferior mesenteric artery; LCA, left colic artery; LN, lymph node; SRA, superior rectal artery.
The area of dissection with the artery cutting points on the images of preoperative 3D-CT angiography and the intraoperative laparoscopic view of LCA-preserving D3 LN dissection in a patient with upper-rectal cancer is shown in Figure 2.
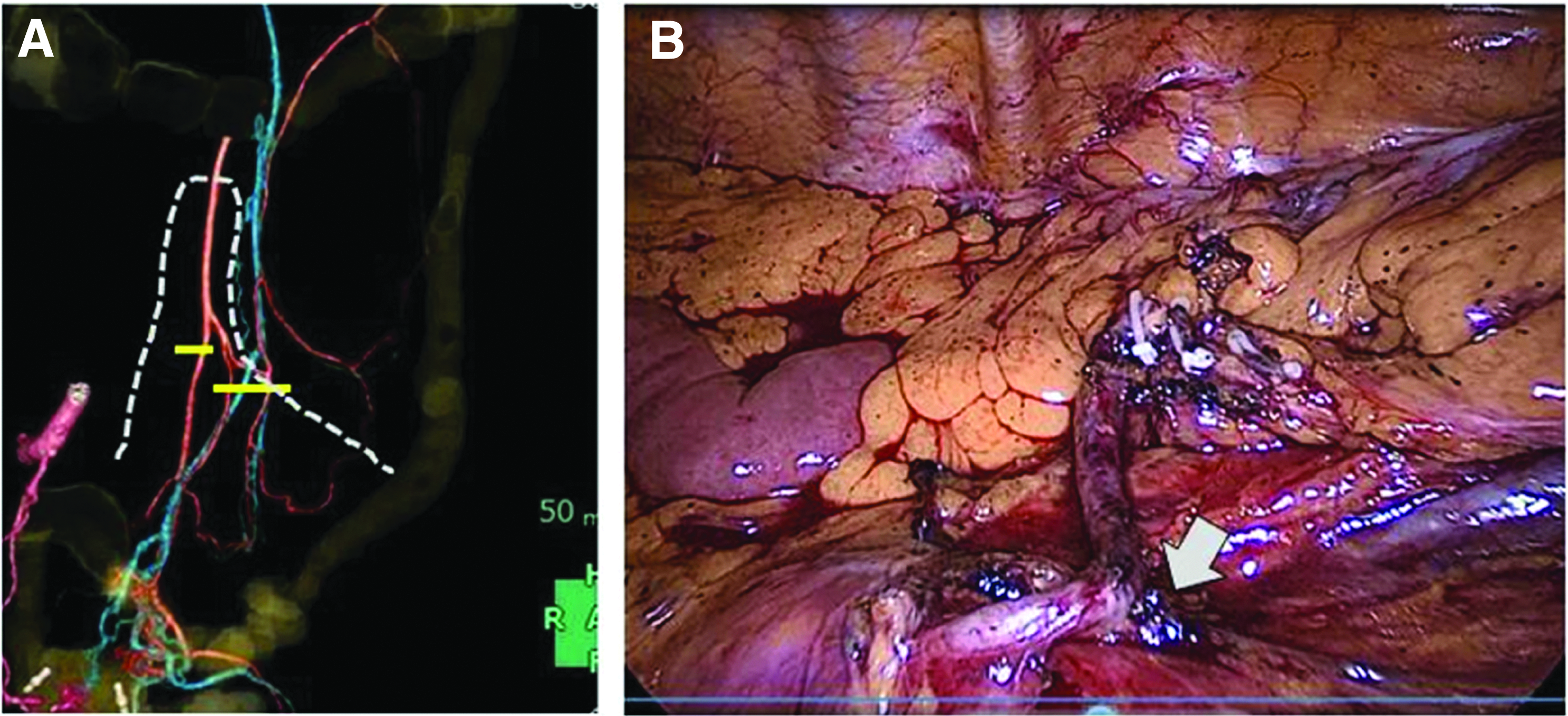
The area of dissection with the artery cutting points on the images of preoperative 3D-CT angiography
The numbers of LNs dissected in IMA-preserving laparoscopic surgery are shown in Table 3. The mean number of LNs pathologically identified in the specimens was 19.6 in the D3 group and 12.9 in the D2 group. The mean number of LNs dissected in the D3 group was significantly higher than that in the D2 group (P = .0002). The average number of LNs dissected in the D3 cases was 20.3 in patients with the LCA preservation and 14.9 in patients with both the LCA and SRA preservation, respectively; they did not differ to a statistically significant extent.
LCA, left colic artery; LN, lymph node; SD, standard deviation; SRA, superior rectal artery.
At the latest follow-up examination, the median follow-up period of the survivors was 48 months (range, 24–105 months). Cancer recurrence had occurred in 10 patients, and 3 patients died from cancer progression. No patients developed LN recurrence after surgery (Table 4). Six patients died due to other diseases without cancer recurrence (Table 5). The overall and disease-free survival curves after surgery are presented in Figure 3. The estimated 5-year overall survival rates of the stage I, II, and III patients were 93%, 92%, and 88%, respectively. The estimated 5-year disease-free survival rates of the stage I, II, and III patients were 93%, 83%, and 74%, respectively.

S, sigmoid colon; Rs, rectosigmoid; Ra, upper rectum.
HAR, high anterior resection; LAR, low anterior resection.
LCA, left colic artery; SRA, superior rectal artery.
Chemo, chemotherapy.
BSC, best supportive care.
S, sigmoid colon; Rs, rectosigmoid; Ra, upper rectum.
HAR, high anterior resection; LAR, low anterior resection.
LCA, left colic artery; SRA, superior rectal artery.
AMI, acute myocardial infarction.
SMA, superior mesenteric artery.
Discussion
We retrospectively analyzed the results of IMA-preserving laparoscopic LN dissection in 142 patients with stage I–III upper-rectal or sigmoid colon cancer to evaluate the long-term oncologic outcomes. In this study, the estimated 5-year disease-free survival rates of the stage I, II, and III patients were 93%, 83%, and 74%, respectively. These rates were not inferior to those of the COLOR trial (5-year-DFS in stage I–III: 67%), 16 COST study (5-year-DFS in stage I, II, and III: 83%, 70%, and 49%, respectively), 17 and CLASICC trial (5-year-DFS in stage I–III: 55.3%),18,19 and were almost identical to the rate of the JCOG0404 trial (5-year-DFS in stage II–III: 79%). 20 Although this study included a limited number of patients and was a retrospective analysis that was performed in a single institution, the result suggests that laparoscopic surgery with IMA-preserving LN dissection for upper-rectal or sigmoid colon cancer was performed with acceptable long-term oncologic results.
It remains controversial whether high or low ligation of the IMA should be the standard treatment for patients with advanced rectal or sigmoid colon cancer. There is no consensus regarding the level of arterial ligation in patients with advanced stage colorectal cancer. No randomized clinical trials have been conducted to compare high and low ligation procedures in colorectal cancer surgery.1–4,21 The high-ligation technique enables the en bloc removal of the lymphatic drainage around the IMA22,23; however, the survival benefit of this procedure is not clear. Some guidelines recommend low ligation for rectal cancer surgery without massive LN involvement 24 ; however, many laparoscopic surgeons prefer high ligation to avoid complicated procedures to preserve the IMA.
The drawback of the high-tie technique with regard to blood flow of the colon has been discussed. The high-tie technique can jeopardize blood supply to the proximal or distal side of the anastomotic site, and may occasionally result in anastomotic leakage or need for wider resection of the colon.4,6–8 A randomized controlled trial by Tocchi et al. demonstrated that the prevalence of anastomotic leakage in an IMA ligation group was higher than that in an IMA preservation group; however, the study involved patients with diverticular disease. 25 Numerous reports using Doppler flowmetry have shown that the blood flow to the colon fell significantly after ligation of the IMA.6,8 Thus, LN dissection with the preservation of the IMA may maintain a good blood supply to the remnant bowel through the LCA or SRA.
Another advantage of IMA-preservation is that the presence of IMA and LCA allows for a wider range of surgical strategies for metachronous colorectal cancer. In case of surgical treatment of metachronous transverse cancer in patients who have previously undergone an operation for rectal cancer, the middle colic artery (MCA) can be cut at its root if the LCA has been preserved in the previous operation. However, if the IMA has been cut in the previous operation, LN dissection around the MCA is impossible without sacrificing the majority of the colon. Metachronous colorectal adenocarcinoma was reported to develop within 4 years after surgery in 1.7%–2.9% of the patients who underwent curative resection for stage I–III colorectal cancer.26,27 The incidence of occurrence of second colorectal cancer after primary colorectal cancer is 1.4 times higher than that in the standard population. 28 Consideration for the second colorectal cancer is especially important when treating patients who are relatively younger. 27
In this study, the median operative time was acceptable (230 minutes), and the median volume of operative blood loss was very low (17 mL). However, D3 LN dissection with preservation of the IMA is technically demanding in comparison to LN dissection with the sacrifice of the IMA. We therefore performed preoperative 3D-CT angiography to gain information about the types of IMA branching in the majority of the patients. Advancements in MDCT scanner technology together with the introduction of contrast mediums have allowed for the acquisition of volumetric data sets and have revealed the human vascular anatomy with a very high level of detail.29,30 Many reports have described the advantages using patient-specific 3D angiography generated by MDCT images in the planning of cancer surgery.31,32 In this study, preoperative 3D-CT angiography images gave us information about the anatomy of the IMA (the branching pattern and length), the course of the LCA, and the anatomical relationship between the LCA and IMV. Although it is difficult to show the advantage of using 3D-CT angiography numerically, the application of preoperative 3D-CT angiography greatly assists the surgeon in planning and performing the operation.
We conclude that IMA-preserving laparoscopic LN dissection is an acceptable treatment strategy for patients with upper-rectal or sigmoid colon cancer based on the long-term oncologic results that were achieved without jeopardizing the surgical curability. To the best to our knowledge, this is the first report to present the long-term oncologic outcomes of laparoscopic LN dissection with the preservation of the IMA.
Conclusions
The present results indicate that the IMA-preserving laparoscopic LN dissection is an acceptable treatment strategy for patients with upper-rectal or sigmoid colon cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.