
Abstract
Abstract
Introduction:
Laparoscopic pyeloplasty is becoming the gold standard procedure for pelviureteric junction obstruction. The outcome of pyeloplasty depends on precise pyeloureteral anastomosis. Though in open pyeloplasty interrupted or continuous suture are practiced, in most of the laparoscopic or laparoscopy-assisted robotic pyeloplasty continuous suturing is practiced. After acquiring a 3-dimensional (3D) camera, we prospectively analyzed the suturing time, complication rate, and success rate between interrupted and continuous suturing in laparoscopic pyeloplasty.
Objective:
To prospectively review the outcome difference between interrupted suturing (group A) and continuous suturing (group B) while using a 3D camera.
Materials and Methods:
Out of 93 patients who underwent laparoscopic pyeloplasty, 6 patients who underwent retro-peritoneoscopic approach, 7 patients who had nondismembered technique, 7 patients with secondary renal calculi, and 3 patients with grossly dilated pelvis were excluded from the study to reduce bias. Hence, the remaining 70 patients who underwent transperitoneal pyeloplasty from 2012 to 2017 were prospectively analyzed, comparing 35 cases of interrupted suturing with 35 cases of continuous suturing using 3D camera in an alternating manner. The primary aim was to know the difference in suturing time. The secondary outcomes were success of pyeloplasty, complications, and drain volume. The statistical analysis was done using SPSS 2.0 software.
Results:
Of the 70 cases, with 35 in each arm studied, the mean suturing time, success rate, and complications were not significantly different. The total drain quantity during the hospital stay was observed to be more in the interrupted suturing group.
Conclusion:
The usage of a 3D camera and experience of the surgeon reduced the time difference between continuous and interrupted suturing in laparoscopic pyeloplasty. The outcome between interrupted and continuous suturing groups were the same. Though the drainage volume was more with interrupted suturing group the outcome was not altered.
Introduction
L
We have prospectively compared interrupted suturing with continuous suturing in pyeloureteral anastomosis to find an answer to whether continuous suturing or interrupted suturing is better. In author's previous reported retrospective study of 107 cases, the same comparison was reported using a 2-dimensional (2D) high definition (HD) camera. 5 However, in this prospective study of the subsequent 93 cases, 3D camera was used.
Materials and Methods
We reviewed all the 200 laparoscopic pyeloplasty patients done at our center from January 1998 to June 2017. A total of 107 patients were excluded from the study as they were retrospectively analyzed and reported earlier. The subsequent 93 patients were prospectively analyzed between 2012 and 2017. Six patients who underwent retro-peritoneoscopic approach, 7 patients who had non-dismembered technique, 7 patients with secondary renal calculi, and 3 patients with grossly dilated pelvis were excluded from the study to reduce bias. Hence, 70 patients were included in this study. There were 35 cases each in continuous suturing and interrupted suturing group. All patients had ultra sonogram, intravenous urogram, or computed tomography urogram and diuretic renogram. A sterile urine culture was mandatory preoperatively. All patients underwent transperitoneal approach using 3D camera by a single surgeon having more than 20 years of laparoscopic experience. Gross reduction of pelvis was not carried out as this could cause variation in the suturing time. Ureter was spatulated laterally for about 15 to 20 mm below UPJ and corresponding length of pelvis was excised so that the suture lines matched approximately. All the patients had ureteric stent placed intraoperatively. A 14F caliber tube drain was placed through the flank port in all patients. Stent removal was done 6 weeks postoperatively. Ultrasonogram was done every 3 months for 1 year and annually for 5 years. Diuretic renogram was done 6 months postoperatively and annually for 5 years. Data on overall operating time, suturing time, total drain quantity till drain was removed, hospital stay, complications, and success rate based on renogram done at 6 months were analyzed. The statistical analysis was done using SPSS 2.0 software. Postoperative pain and analgesia were not analyzed in this study.
Operative technique
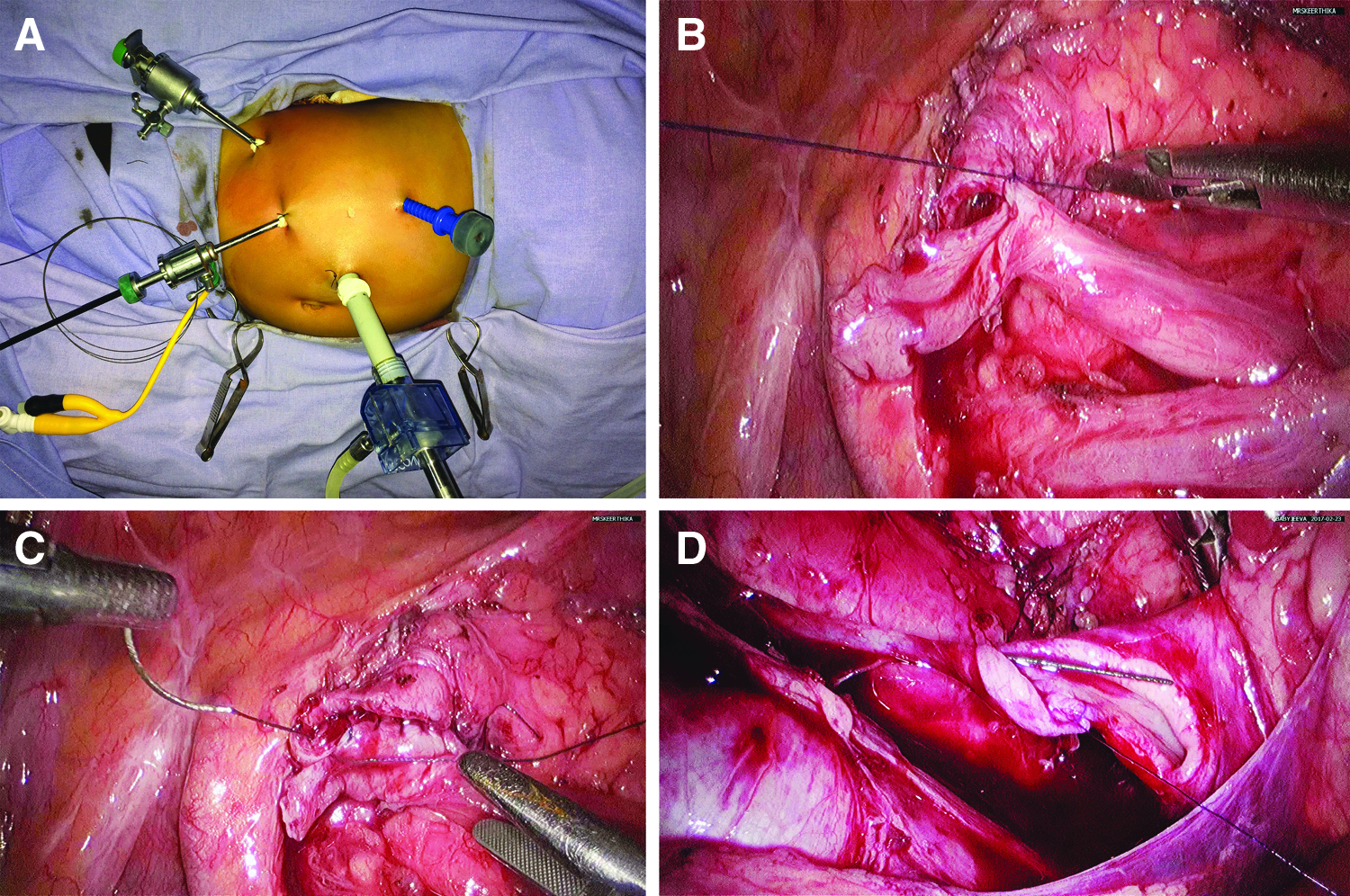
Under general anesthesia patient was placed in lithotomy position and retrograde pyelogram was done to evaluate the length of the UPJ narrowing. Position was changed to 70 degree lateral position and four ports were inserted (10 mm camera port 5 cm above and lateral to umbilicus, one 5 mm port in mid clavicular line in the subcostal region, and one 5 mm port in the mid clavicular line in spino-umbilical line and the fourth port in the flank for using suction or irrigation) (Fig. 1A). For all the right sided cases, right colon was mobilized. However, on the left side if the mesocolon was thin and if there were no large vessels in the mesocolon transmesocolic approach was used. 6 The proximal 5 cm of ureter and just enough of pelvis were mobilized avoiding injury to crossing vessel if any. Oblique pyelotomy was done without disconnecting the pelvis and ureter, to maintain the orientation. The ureter was then spatulated laterally for about 15 to 20 mm depending on the age of patient. A stay suture was placed between the dependant portion of the pelvis and the spatulated part of the ureter (Fig. 1B). Subsequently, pyelotomy was completed. The pyelum flap was retained for retraction purpose to minimize handling of the spatulated ureteral edges. Posterior layer of pyeloureteral suturing was done initially (Fig. 1C). 4-0 polydioxanone (PDS) suture was used in adults and 5-0 PDS suture was used in children for the continuous suturing and 4-0 polyglactin suture was used in adults and 5-0 polyglactin suture was used in children for interrupted suturing (Fig. 1D). Stenting was done antegrade using a Verres needle outer sheath placed in hypochondrium in line with the ureter. Subsequently, anterior layer suturing was done taking care that the sutures are equidistant. If a pyelotomy defect was present it was closed with the same suture. Perirenal fat was tacked to the suture line. Tube drain was placed through flank port in both groups. On the second postoperative day ultrasound scan was done to rule out any collection in perirenal area. Urethral catheter was removed after 48 hours and drain tube was removed when the drain was less than 20 mL in 24 hours.
The laparoscopic pyeloplasty was defined as successful if symptoms are alleviated; or if there is improvement or stabilization of renal function based on the glomerular filtration rate and T1/2 in diuretic renogram.
Results
Out of 70 patients, 35 patients underwent interrupted suturing (group A) and 35 patients underwent continuous suturing (group B) alternatively. Nine patients in group A and 8 patients in the group B had crossing vessels. Nine patients in group A and 6 in group B were children (below 18 years) Age distribution and gender distribution were matching. None needed conversion to open surgery. All procedures were done by a single surgeon with more than 20 years of laparoscopic surgery experience. The follow-up was between 60 to 6 months with a mean of 40.4 months. The demographic characters are illustrated in Table 1.
GFR, glomerular filtration rate.
The mean operating time was 158 minutes in the interrupted suturing group and 157 minutes in continuous suturing group. The mean anastomosis time was 76.4 minutes in interrupted suturing group and 70.9 minutes in continuous suturing group. The mean drain quantity was 76 mL in group A and 49 mL in group B. Mean hospital stay was 4.43 in group A and 4.09 days in group B. The operative and postoperative details are shown in Table 2.
GFR, glomerular filtration rate.
The complication rate was same (20%) in both group A and group B. Three patients in group A and 4 patients in group B had urinary tract infection that settled with a course of antibiotic. Three patients in group A and 2 patients in group B had ileus lasting for 3 days. One patient in the group A had port site hematoma that got absorbed over a week. One child in group B had port site omental herniation at the time of drain tube removal (Clavien-Dindo grade 3). This child needed reduction of port site omental hernia under general anesthesia (Table 3).
One patient in the interrupted suture group had loin pain 2 years after surgery and the renogram showed delayed drainage. She underwent laparoscopic redo pyeloplasty. Renogram done subsequently showed improvement.
Discussion
More and more urologists are doing pyeloplasty using laparoscopy or laparoscopy-assisted robotic approach. The standard technique in open pyeloplasty is to use interrupted or continuous suturing technique. 7 Though laparoscopic suturing consumes more time than open pyeloplasty, it is preferred as the morbidity is far less. Both interrupted and continuous suturing are practiced in laparoscopy. In robot-assisted laparoscopic pyeloplasty, continuous sutures were only used. 8
In the current prospective study of 70 cases we analyzed 35 cases of interrupted suturing with 35 cases of continuous suturing, with one technique alternating with the other. To reduce the bias, patients who had retroperitoneoscopic approach, patients who had nondismembered technique, patients with secondary renal calculi, and patients with grossly dilated pelvis were excluded from the study. Intraoperative stenting may vary a bit from case to case and cause a bias in the duration of suturing. All cases were done by a single surgeon.
Experimental studies on the effect of interrupted and continuous suturing have been done mostly in animals. Lieber et al. in their porcine model study compared interrupted suture against continuous suture and concluded that there is extensive fibrosis in interrupted suture group. 9 Mehl et al. in their animal (cat) experimental study of ureteroneocystostomy indicated that continuous suture causes more tissue ischemia and even necrosis 10 but this cannot be extrapolated to pyeloplasty in human being.
Kass, in a study of pyeloplasty in infants concluded that interrupted suturing would result in reduced purse-string effect 11 and reported a success rate of 100% and overall complication rate of 7.6%.
Papalia et al. compared three groups of patients who underwent laparoscopic pyeloplasty. The first group underwent interrupted suturing with antegrade stenting. The second group underwent running sutures with antegrade stenting and the third group had retrograde stenting with two running sutures and recommended the third group that had the least operating time. 12
Shao et al. compared interrupted and continuous suturing in retroperitoneoscopic pyeloplasty in 105 patients and concluded that continuous suturing was quicker and had less complications. 13 The difference in the suturing time was 19 minutes (47 minutes in interrupted suturing versus 28 minutes in continuous suturing). In the authors' current study the difference in suturing time between interrupted suturing group and continuous suturing group was 6 minutes, which was not statistically significant.
In the authors' previous retrospective study of 107 patients comparing continuous suturing with interrupted suturing using 2D camera, there was a statistically significant increase in duration of suturing, quantity of drainage, and hospital stay while using interrupted suturing. Hence, the authors concluded that continuous suturing may be preferred. 5
In our center we have been doing laparoscopic pyeloplasty for the past 20 years without a single case of conversion to open. 3D camera was used from 2012 onward. The time difference between continuous and interrupted suturing was not statistically significant probably related to the use of 3D camera and experience of the surgeon.
Tung et al. in their study in training models using 2D and 3D camera concluded that 3D camera accelerates the learning curve in younger surgeons with less experience. However, among specialists there was no difference between usage of 2D or 3D camera. 14
In another study by Abou et al. in their initial experience in laparoscopic pyeloplasty using 3D camera and articulating shears reported that it reduces the duration of surgery by 48 minutes and mentioned that this method may be a hybrid of laparoscopy and robot. 15
Rassweiler et al. 16 in their large series of laparoscopic pyeloplasty report that the complications in continuous suturing was 7.9%. Even though the overall complication in our study is 20%, 6 out of 7 were Clavien grade 1 in each group.
Shao et al. reported that the complication rate was more in the interrupted suturing group 14% compared to 3.2% in the continuous suturing group. They reported a success rate of 100% in both groups.
Liatsikos et al. in their study of laparoscopic pyeloplasty using barbed continuous suture remarked that barbed suture induces more fibrosis resulting in 100% failure. 17
The overall success rate was 98.57% in this study with no significant difference between the two groups. In a larger study by Rassweiler et al. 18 the success rate was 95.2%. In the authors' previous study of 107 patients the success rate was 95.24% wherein 2D camera was used. 5 The improvement in the success rate may be due to the use of 3D camera and the surgeons experience.
Conclusion
The usage of 3D camera and experience of the surgeon reduced the time difference between continuous and interrupted suturing in laparoscopic pyeloplasty. The outcome between interrupted and continuous suturing groups was the same. The only difference between the two groups was the drainage volume. However, the drainage volume did not alter the hospital stay or the outcome of surgery.
To the authors knowledge this is the first prospective study comparing interrupted and continuous suturing in laparoscopic pyeloplasty using 3D camera.
Footnotes
Disclosure Statement
No competing financial interests exist.