
Abstract
Abstract
Background:
Case reports and small series of the surgical and radiological management of median arcuate ligament syndrome (MALS) have been described, however, long-term outcome data are lacking. The purpose of this study was to review our experience of the laparoscopic management of MALS, and describe the long-term outcomes after surgical intervention.
Methods:
Data were collected between 2005 and 2016 in a single U.K. institution. All patients with MALS who underwent laparoscopic decompression of the celiac artery were included. Surgical outcomes were recorded from a prospectively collected database. Long-term outcomes were determined by outpatient review and the Gastrointestinal Quality of Life Index (GIQLI).
Results:
Six patients were included. Five were female with a median age of 30 years (22.3–48.3). All six presented with abdominal pain and a bruit. Length of symptoms on presentation was 41 months (19–69). Duplex ultrasonography indicated celiac trunk stenosis in each case, with an elevated peak velocity flow in the celiac trunk of 230 cm/s (210–287.5). All six underwent successful laparoscopic decompression of the celiac artery with no conversions to open. Operating time was 137.3 minutes (95.6–166.3) and intraoperative blood loss was 110 mL (65–225). Length of stay was one day (1–2.3), with no postoperative complications or mortality. Median follow-up was 109.5 months (78–113.5). At this point, all patients remained symptom free with an overall GIQLI score of 129/144 (123.8–134.5).
Conclusions:
MALS is a rare condition. Laparoscopic decompression of the median arcuate ligament is safe and offers long-term resolution of symptoms, and improvement in patient quality of life.
Introduction
T
The diagnosis is elusive and often one of exclusion. Typically, patients have suffered longstanding abdominal symptoms and undergone many investigations, culminating in the identification of an external stenosis of the celiac trunk. Debate remains regarding the exact pathophysiology of MALS, and both ischemic and neuropathic etiologies have mainly been proposed. However, other pathophysiologies such as delayed gastric emptying 3 have also been suggested.
Various surgical and radiological approaches have been described, but mainly limited to a handful of case reports and small case series. Initially, treatment of MALS was typically achieved by open surgical procedures and major vascular reconstructions. Early clinical series reported that the symptoms of celiac axis compression could be relieved by release of the ligament.4,5
More recently, clinicians have focused on laparoscopic techniques to address MALS, although the bulk of this evidence remains restricted to case reports. To date, the literature is further limited by a significant lack of data on the long-term outcomes of patients who have undergone laparoscopic surgery for MALS. Given that the goal of surgery is symptomatic resolution and consequent quality-of-life improvement (QLI), the degree and longevity of symptom relief are the fundamental attributes that will define the success of the operation. Accordingly, we aimed to review our experience of the laparoscopic management of MALS and describe the long-term outcomes and gastrointestinal quality of life after surgery.
Materials and Methods
A prospective evaluation of a cohort receiving usual care in a single upper gastrointestinal surgical unit in the United Kingdom between 2005 and 2016. All patients consented for their data to be used anonymously, and the study complied with the Declaration of Helsinki.
All consecutive individuals with a putative diagnosis of MALS who were referred to our center for surgical opinion were considered. Those with symptoms consistent with MALS and radiographic evidence of external celiac axis compression, and progressed to laparoscopic decompression of the celiac artery, were included. In the patients studied, celiac axis compression was identified by a number of imaging modalities, namely computed tomography (CT), CT angiography (Fig. 1), and magnetic resonance angiography (MRA). Duplex ultrasonography was performed in all patients preoperatively to confirm stenosis. We defined a value of 200 cm/sec as evidence of >70% stenosis of the celiac artery.
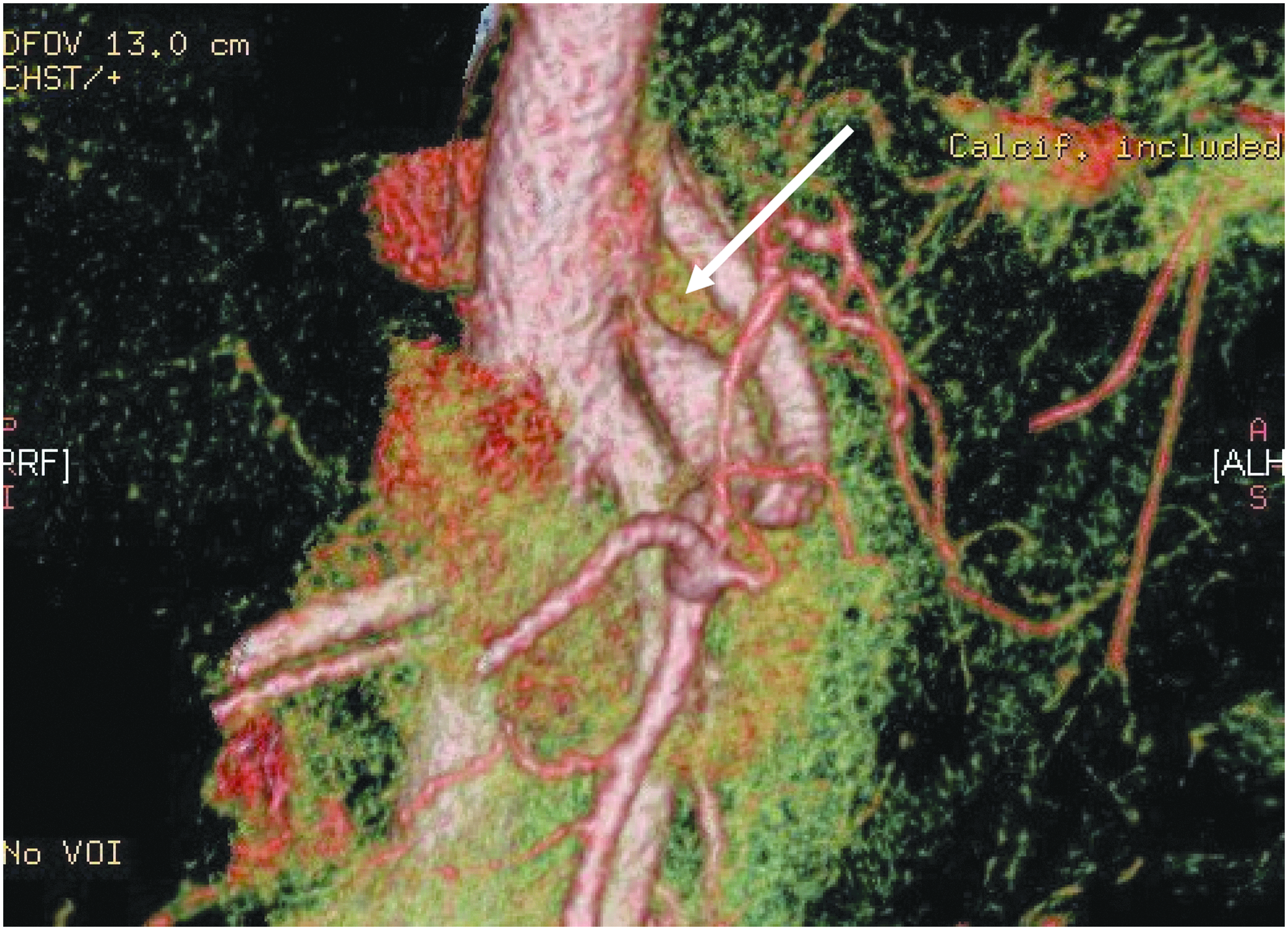
CT angiography, 3D reconstruction showing stenosis of the origin of the celiac trunk with poststenotic dilatation (arrow).
Surgical technique
Under general anesthesia, patients were positioned supine, in a modified lithotomy position with knees slightly flexed. The operating surgeon stands between the legs and the table is placed at 30–45 degrees of reversed Trendelenburg to displace the transverse colon and small bowel. Two 10 mm and two 5 mm ports are utilized. An open Hasson technique is used to insert a supraumbilical camera port, and thereafter a 10 mm port placed in the left lateral position, and two 5 mm right lateral ports all introduced under direct vision. Full laparoscopy is performed with a 30-degree laparoscope. A Nathanson liver retractor is inserted to retract the left lobe of the liver and display the esophageal hiatus. The gastrohepatic ligament is opened with a Harmonic Scalpel® to expose the right pillar of the crus. In our first case, the crural tissue was divided to expose the thoracic aorta. Having established the prevascular adventitial plane, dissection continued inferiorly toward the median arcuate ligament. In all subsequent cases, the approach was modified to reduce the crural dissection and associated surgical trauma. In these patients, the stomach is retracted anteriorly and the left gastric pedicle identified and traced to its origin at the celiac trunk. The median arcuate ligament is thus approached directly, inferiorly (Fig. 2), and bluntly dissected in the prevascular plane beneath the ligament. Once isolated, the ligament is divided by the harmonic scalpel releasing the celiac trunk, which can be confirmed by clear visualization of its origin from the aorta (Fig. 3).
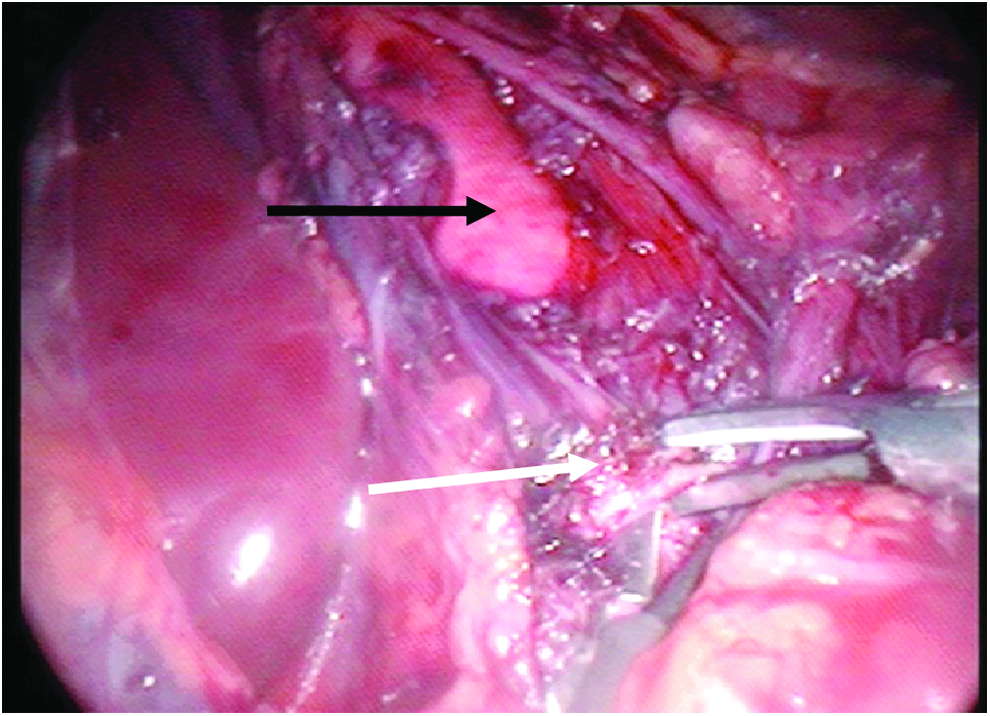
Our laparoscopic approach to the median arcuate ligament (white arrow), with exposure of the aorta (black arrow) by division of the crura superiorly.
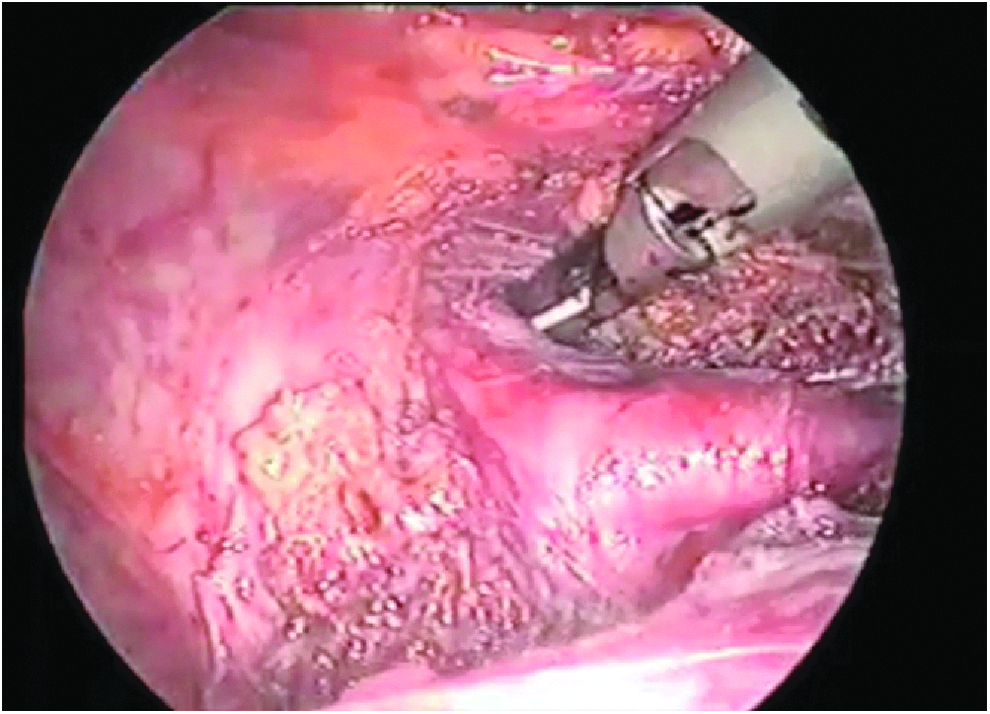
Laparoscopic view of the released celiac trunk and its origin from the aorta, after complete division of the ligamentous tissue.
Follow-up
Patients were reviewed in the outpatient clinic at 6–8 weeks postoperatively. Quality of life was determined using the Gastrointestinal Quality of Life Index (GIQLI), namely a validated questionnaire (scored 0–144) investigating patient status in gastrointestinal disease. 6 The GIQLI determined postoperative quality of life and all patients completed this in January 2017.
Data collection and statistics
All routine data were collected, including patient demographics, investigations, and radiological and operative details and were obtained from a combination of a prospectively collected database and patient records. Categorical data are presented as frequency and continuous variables as median and interquartile range.
Results
Patient characteristics
Twelve patients were referred during the study period. Six patients were not suitable for surgery based on nontypical clinical symptoms of MALS (n = 2). Furthermore, despite radiological evidence of celiac axis compression, duplex ultrasonography of the celiac axis was normal range in all six. These patients were thus excluded from further analysis.
The remaining six individuals with symptoms and investigations in keeping with MALS underwent laparoscopic release of the median arcuate ligament. These six constituted the study group. Characteristics are shown in Table 1.
BMI, body mass index; n, number of patients.
Most patients were young, underweight females. Only two patients had significant medical comorbidities at the time of surgery, namely an IgA deficiency (n = 1) and rheumatoid arthritis (n = 1). Two patients had previous abdominal surgery (a cesarean section and femoral hernia repair in one individual and an appendectomy in the second).
Presenting symptoms
In all six, abdominal pain was the predominant symptom, of which four described the pain as mostly postprandial. Two individuals complained of early satiety and three patients had documented weight loss. All six had an audible abdominal bruit on examination.
The radiological diagnosis of MAL syndrome
The first patient of our series initially underwent balloon dilatation of the celiac axis. Interestingly, during this interventional procedure, balloon inflation precipitated the patient's symptoms, which then resolved on deflation. Her symptom improvement was temporary and she required surgery consequently.
Conventional angiography was not utilized in any of the remaining patients. Duplex ultrasonography showed an elevation in peak velocity flow in the celiac trunk in all individuals undergoing surgery (median 230 cm/sec, IQR 210–287.5), indicative of significant stenosis of the celiac trunk. Additional imaging modalities used in the investigation of these patients included angiography (n = 1), MRA (n = 3) and CTA (n = 2, Fig. 1). These diagnostic studies confirmed normal patency of both the superior and inferior mesenteric arteries in all patients, while confirming extrinsic nonatherosclerotic stenosis of the celiac axis.
Patients had been subjected to other investigations before referral, such as transabdominal ultrasonography (n = 6) and esophagogastroscopy (n = 3), all with normal findings.
Operative details
The laparoscopic division of the median arcuate ligament was the index procedure for the management of MALS in all (Table 2).
ASA, American Society of Anesthesiologists; n, number of patients; HDU, high dependency unit.
All patients resumed oral intake of fluids on the day of surgery and were commenced on a light diet on the first postoperative day. Following discharge, one patient was readmitted on the 15th day after discharge. This was a consequence of opiate analgesic-induced constipation. Abdominal CT scan confirmed no intra-abdominal collection, hematoma, or other postoperative complication.
Symptom resolution and postoperative quality of life
In the outpatient clinic follow-up, all patients reported complete symptomatic relief from their preoperative symptoms and remained well with normal diet and no postoperative morbidity. Only patient 1 of the surgical series was referred back to our service with further abdominal pains, 5 years after intervention. Duplex ultrasonography did not detect restenosis of the celiac axis (flow <200 cm/s). No diagnosis was made and following this temporary relapse, the patient then remained symptom free. The median follow-up of the group is now at 109 months (78–113.5).
At the most recent follow-up, all patients reported to be symptom free with a median GIQLI score of 129/144 (123.8–134.5, Table 3). There have been no surgical or radiological reinterventions on the celiac axis.
GIQLI, Gastrointestinal Quality of Life Index.
The last two patients of the series (patients 5 and 6) underwent follow-up duplex ultrasound, 8 weeks postoperatively. The velocity improvements, respectively, were measured from 300 cm/sec preoperatively to 125 cm/sec following surgery, and in the second, a decrease of 210–150 cm/sec postoperatively.
Discussion
This study has revealed that with careful case selection, laparoscopic surgery is a safe and effective intervention for MALS, with longstanding symptom relief. We found that patients scored highly on the validated GIQLI postoperatively and described a good quality of life many years after surgery. In fact, all individuals reported that they have remained free of their previous MALS symptoms, in what is to date one of the longest follow-ups of patients after laparoscopic decompression of the celiac axis in the existing literature. 7 While the cohort studied is small, it is nevertheless among the largest laparoscopic series reported in contemporary literature.
The need for careful case selection is crucial to the success of the operation. Previous evidence has identified potential predictors of poor outcome, including unprovoked pain, vomiting, 8 and evidence of extensive collateral mesenteric arterial circulation. 9 However, the majority of case reports and series in both adults and children10–13 reveal that surgical division of the median arcuate ligament leads to good symptomatic improvement, and those who present with classical symptoms achieve the best postoperative results. Furthermore, postexertional pain14,15 may be completely resolved by division of the median arcuate ligament, giving weight to a hemodynamic, ischemic basis of the symptoms.
The diagnosis of MALS is frequently one of exclusion. Consequently, patients will often present with longstanding symptoms and have undergone a number of unfruitful investigations, as was the case in our cohort.
The clinical entity of MALS has long been a matter of controversy and the pathophysiology of the symptoms is not clearly understood. Theories of a vascular or neurogenic origin have both been championed, but objective evidence is lacking. The ischemic theory suggests that celiac trunk compression could be responsible for a celiac steal, resulting in shunting of blood from the SMA to the celiac distribution through the collateral system. However, partial or even complete obstruction of the celiac artery should not lead to visceral ischemia. This can be demonstrated first by the presence of rich collateral blood supply, and second, in that surgical ligation of the celiac axis can be performed without untoward consequences. In addition, and as previously stated, celiac axis stenosis may be present in asymptomatic individuals. An alternative theory of MALS put forward is the neurogenic basis of the symptoms, which postulates that the pain is mediated by the celiac ganglion itself. In the two articles where this theory was originally postulated,16,17 compression of the celiac axis occurred either by the nerve fibers themselves or the median arcuate ligament. In these cases, surgical sympathectomies were performed to encourage increased blood flow.
There is evidence to suggest that celiac artery compression is more common than first thought, despite the syndrome itself being diagnosed rarely. It is necessary to distinguish pathological compression of the celiac axis from a normal variant demonstrated in cadaveric studies, where it was reported that the prevalence of median arcuate ligaments overlying the celiac axis is 43.5%. 18
Multiple techniques have been described to address MAL syndrome, including open division of the median arcuate ligament, 5 vascular reconstruction, division of the celiac trunk, 19 or a combination of these procedures.20–23 Radiological interventions by balloon dilatation or stent placement have also been described. 24 These may be performed either as an adjunct or as an alternative to surgical division. 25 Chronic pain management by the injection of intrathecal morphine has also been explored. 26 While endovascular interventions are effective treatment for occlusive vascular disease, the failure rate is significantly higher in cases of external vascular compression. 26 It is proposed that repeated trauma as a result of respiration causes stent failure in such cases. Similarly, poor results have been seen in other vascular compression syndromes such as thoracic outlet syndrome. 28 The use of vascular bypass techniques as a second-line surgical intervention can be considered in the treatment of MALS, but this would negate any advantages achieved by the use of the laparoscopic approach.
In our technique, we reduced the dissection around the hiatus initially adopted in the open technique and its subsequent reconstruction. As a result, we found that postoperative pain was reduced. In addition, and in accordance with other studies,29,30 intraoperative ultrasound was used to demonstrate anatomy and improvement in blood flow following division of the median arcuate ligament. This consequent likely decrease in ischemia with associated symptom resolution adds further gravitas to the theory of ischemia-driven symptomology in the syndrome.
There are a number of limitations to this study. In the first instance, the results are based on a small cohort of patients, which reflects the rarity of the condition. Second, we lack follow-up duplex data in four of the six patients. This would have provided useful objective evidence of the rate of flow following laparoscopic release of the median arcuate ligament. Arguably the ultrasound was not indicated, however, because there had been complete resolution of the symptoms. In addition, we did not perform inspiration and expiration values for the duplex recording, and in future studies these data would be useful to collect. Finally, the length of follow-up revealed that laparoscopic decompression of the celiac axis is a valid and potentially permanent improvement in quality of life. It must be noted, however, that the last patient in the cohort is within 6 months of surgery, and therefore, further follow-up is necessary to ensure that this patient follows the clinical path of the remaining cohort, namely long-term symptom control.
In conclusion, to diagnose the MALS, patients should present with a typical symptom profile, supported by radiological evidence of external celiac axis compression and demonstrably reduced celiac blood flow. The correct diagnosis of this rare condition is essential to identify those patients who are suitable and most likely to benefit from surgery. The laparoscopic technique we describe is safe and effective, and leads to good gastrointestinal quality-of-life indices, as well as excellent long-term symptom control, based on our local evaluation.
Footnotes
Disclosure Statement
No competing financial interests exist.