
Abstract
Abstract
Background:
Laparoscopic surgery for T4 colon cancer remains controversial according to many colorectal cancer guidelines. The aim of this study was to compare short- and long-term outcomes in patients who underwent T4 colon cancer resection by laparoscopy versus open surgery.
Methods:
Patients who underwent T4 colon cancer resection either by laparoscopy or by open surgery between January 2012 and January 2017 were included and used to perform a retrospective cohort analysis. Demographics, patient characteristics, short-term outcomes, and long-term oncological outcomes were compared between two groups. Multivariate analyses were used to define prognostic factors of overall survival.
Results:
Groups were comparable in terms of preoperative characteristics and demographics. Intraoperative blood loss (127.3 versus 226.1 mL, P = .001) and hospital stay (11.6 versus 14.8 days, P = .001) were significantly reduced in the laparoscopic group compared with the open group. Operative time, bowel movement, time to soft diet, and lymph nodes harvested did not significantly differ between the two groups. R0 resection achieved 100% in both the groups. Similarly, the overall survival rate and disease-free survival rate in stage II and stage III disease showed no significant differences. Multivariate analyses showed that intraoperative blood loss was a significantly independent factor related to a poor prognosis.
Conclusions:
This study suggests that laparoscopy for T4 colon cancer can be safely performed with superior short-term outcomes, such as less intraoperative blood loss and shorter time of hospital stay compared with open surgery, and with similar long-term oncological outcomes. Therefore, laparoscopic procedure could be a viable option in selected patients.
Introduction
C
Laparoscopy is in widespread use for the surgical management of colon cancer. Many randomized controlled trials and meta-analyses identified laparoscopic colectomy for colon cancer with benefits of early postoperative recovery, and with no significant difference in long-term outcomes compared with open resection.3–9 Nevertheless, locally advanced colon cancer and metastatic disease are excluded from these clinical trials.
Based on the American Joint Committee on Cancer (AJCC) staging manual, T4a colon cancer penetrates the surface of the visceral peritoneum; T4b directly invades or is adherent to other adjacent organs or structures. 10 Multivisceral en bloc resection could provide radical cure in the case of locally advanced colorectal cancer. 11 However, according to many international guidelines and consensus, laparoscopic surgery as treatment for locally advanced T4 tumor remains controversial considering the technical difficulty and suboptimal oncological results.12–14 To date, only few studies specially focused on the efficacy of laparoscopic surgery and open surgery for T4 colon cancer.15–22 Moreover, most of these studies had limitations, such as small sample size, including emergent surgery or involving rectal cancer.15,17–20 Emergent conditions, including obstruction and perforation resulting from cancers, result in a difficult surgical environment. 23 In addition, T4 rectal malignant tumor is recommended to undergo neoadjuvant therapy to improve resectability. 24 Therefore, we consider that patients with an emergent setting and rectal cancer should be precluded from the study. In consequence, there are serious queries about safety, technological feasibility, and oncological outcomes on laparoscopic treatment for T4 colon cancer.
The aim of this retrospective study was to investigate the efficacy of laparoscopic surgery of locally advanced T4 colon cancer compared with open treatment.
Methods
Patients
In this retrospective cohort study, the records of all patients (n = 1776) who underwent colorectal cancer resection either by laparoscopy or by open surgery between January 2012 and January 2017 were collected. A total of 200 patients with nonmetastatic pathological T4 colon cancer were eligible and accepted elective curative treatment. Among them, 149 patients underwent laparoscopic surgical resection, 51 patients were approached by conventional laparotomy, and 15 underwent laparoscopic procedures that were converted to open surgery (Fig. 1). The choice of surgery access mainly depended on tumor location, on pattern of the nearby organs' infiltration, and patient's family economic status. The study was approved by the Institutional Review Board of our hospital, and all patients provided written informed consent.

Patients selection.
Inclusion criteria were a clinical diagnosis of adenocarcinoma of the colon (histological confirmation was required at surgery), and the absence of serious abdominal adhesions. Exclusion criteria included pTis-pT3 colon cancer or metastatic disease, rectal cancer, emergent setting, such as acute bowel obstruction or perforation from cancer, and severe medical illness. Inflammatory bowel disease, familial polyposis, pregnancy, or concurrent or previous malignant tumor also precluded enrollment.
Study endpoints
The primary endpoint was distinction in short-term and oncological outcomes between laparoscopic and open surgery. The secondary endpoints were the time to tumor recurrence, defined as the time from randomization to the first confirmed recurrence.
Surgical technique
Both open and laparoscopic colon surgery were performed by surgeons with extensive experience. All laparoscopically assisted and open colectomies were performed according to protocol guidelines, with the same operative principles of radical lymphadenectomy for both groups, and combined resection of invaded adjacent organs.
The time of diet until fluid and solid intake was based upon patient tolerance in both surgical groups.
Histopathological examination
Histopathological examination included assessment of wall depth of invasion (T stage), N stage, distal margin status, and number of lymph node harvest. Tumor classification was by the AJCC staging system. 10 In this, the T4 stage was divided into T4a (penetrates the surface of the visceral peritoneum) and T4b (directly invades or adherent to other organs or structures).
Resections were generally defined as R0 resection (negative microscopic margins), R1 resection (positive microscopic margins without gross residual disease), and R2 resection (incomplete resection with gross residual disease).
Postoperative adjuvant chemotherapy and follow-up
FOLFOX (folinic acid, 5-fluorouracil, and oxaliplatin) has been the most recommended adjuvant chemotherapy proposal for patients with stage III colon cancer. Patients with stage II colon cancer in this study were potential candidates for adjuvant chemotherapy because all enrolled patients were considered high risk (T4 tumors). All patients were advised to adjuvant postoperative chemotherapy unless elder patients (age more than 80), but some patients refused additional chemotherapy for various reasons.
Complications were recorded for the first 30 days following operation. Patients were evaluated at 3 monthly intervals for the first 2 years, and then at 6 months for the next 3 years. Physical examination and tumor-associated antigen assays (include CEA, CA-125, CA-199, etc.) were performed every 3 months. Colonoscopy was performed once a year for 5 years. Total body CT scan was done every 6 months or when requested, where there was clinical suspicion of recurrence.
Statistical analyses
All statistical analyses were conducted using software SPSS 16.0 (Statistical Product and Service Solutions, version 16.0 for Windows, Guangdong, China). Quantitative data were reported as mean, median, standard deviation (SD), and interquartile range (25%–75%). Student's t-test and chi-squared test (or Fisher's exact test when appropriated) were used to compare normally distributed continuous variables and categorical variables, respectively. Survival curves were performed using the Kaplan–Meier method, and the difference between curves was assessed by the log-rank test. Cox regression analysis was conducted to identify possible prognostic factors with adjustment for confounders. Results were reported as hazard ratio (95% confidence interval [CI]). P values <.05 was considered statistically significant.
Results
Characteristics of the patients and tumors
Of the 200 patients who are available for analysis, 51 had an open surgery and 149 had a laparoscopic surgery in our center.
No relevant differences were noted between the two groups in terms of age, sex, body mass index, American Society of Anesthesiologists (ASA) score, and operative procedure. Fifteen patients (10.1%) were converted to open operation from laparoscopic surgery. The reasons for conversion were insufficient visualization of large tumor for complete resection in 3 cases, 11 patients for tumor fixation, and 1 case was required to deal with an intraoperative bowel perforation (Table 1).
ASA, American Society of Anesthesiologists; SD, standard deviation.
Combined resection
The number of cases with combined resection in the laparoscopic surgery group was the same as the open group. The details of the multivisceral resection are presented in Table 2.
Short-term outcomes
Blood loss (mean 127.3 laparoscopy; 226.1 open; P = .001) and hospital stay (mean 11.6 laparoscopy; 14.8 open; P = .001) were significantly lower in the laparoscopic group compared with the open surgery group. The outcome of operative time was noted in 222.0 (81.2) in the laparoscopic group and 203.2 (66.0) in the open surgery group, with no significant difference between groups. The rate of 30-day complications (8.7% versus 17.6%) and Clavien–Dindo score were similar between the laparoscopic and open surgery groups. Similarly, the laparoscopic group showed no difference from the open group in bowel movement (P = .068), time to soft diet (P = .746), and rate of preventive stoma (P = .682) (Table 3).
Significance based on P value <.05.
SD, standard deviation.
Pathological and oncological outcomes
No difference was noted in tumor diameter in the two groups. Two groups were similar in overall staging (P = .477), with 82 (55.0%) of the patients at stage II and 29 (56.9%) at stage III. Similarly, pT stage and pN stage were comparable between the two groups. Each patient in two groups achieved R0 resection. The median number of lymph nodes harvested during surgery was 15 and 16 in the laparoscopic group and open group, respectively.
No patient received preoperative chemotherapy. Adjuvant chemotherapy was given in 105 (70.5%) patients in the laparoscopic group and in 30 (58.8%) patients in the open group (P = .125). No patients received radiation therapy for various reasons.
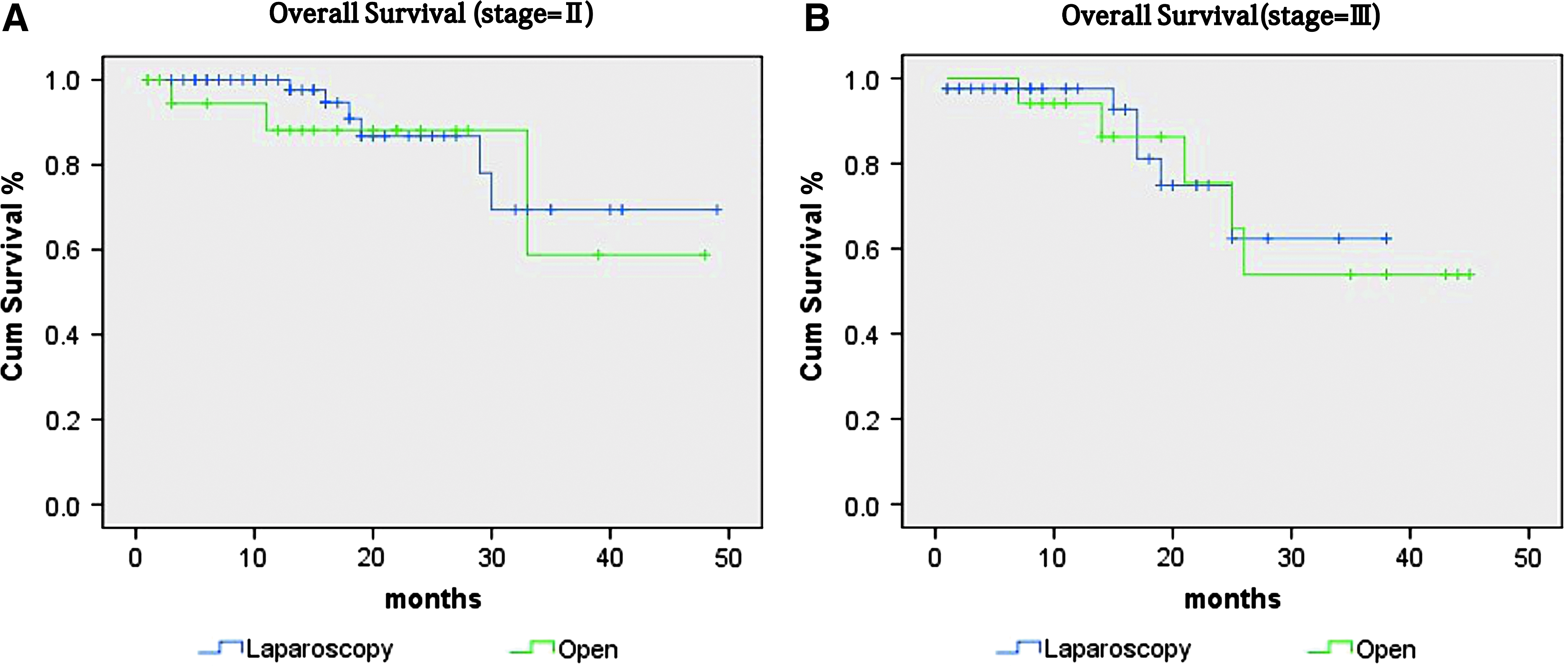
The median follow-up period was 21 months (interquartile range 10–31 months) and 20 months (interquartile range 10–30 months) in the laparoscopic surgery group and the open group, respectively (Table 4). In stage II tumor, the ratio of 3-year overall survival was 69.2% 95%CI [51.5%–87.4%] and 58.7% 95%CI [40.6%–81.7%] in the laparoscopic surgery group and the open group, respectively (P = .651). In stage III tumor, the ratio of 3-year overall survival was 62.5% 95%CI [34.5%–86.2%] and 53.1% 95%CI [37.9%–72.2%] in the laparoscopic surgery group and the open group, respectively (P = .205). In stage II tumor, the ratio of 3-year disease-free survival was 70% 95%CI [54.5%–92.1%] and 61% 95%CI [40.3%–82.1%] in the laparoscopic surgery group and the open group, respectively (P = .730). In stage III tumor, the ratio of 3-year disease-free survival was 47.3% 95%CI [30.2%–72.6%] and 53.4% 95%CI [38.3%–78.1%] in the laparoscopic surgery group and the open group (P = .453) (Figs. 2 and 3).

IQR, interquartile range.
Advanced cancer stage was as well an independent prognostic factor for overall survival in our analysis (Table 5).
Significance based on P value <.05.
Discussion
The feasibility and superiority of laparoscopic resection for colorectal cancer had been proved by many studies.3–9 However, for T4 locally advanced colon tumor, the safety and the efficacy of laparoscopic resection remains controversial due to the potential inadequacy of resection and technical difficulty.12–14 This study suggested that laparoscopic surgery pathologically confirmed that T4 colon cancer was safe and superior compared with the laparotomy, with faster postoperative recovery and acceptable oncological outcomes.
According to some previous studies,15,16,19 laparoscopic surgery for T4 colon cancer required a longer operative time than open surgery. However, Kim et al. 17 and other authors21,22 found that the laparoscopic surgery group had a shorter operative time than the open group. Fewer patients accepted combined resection in the laparoscopic surgery group in these studies, which affected the results. In our study, we detected that the laparoscopy group needed less time for bowel movement and to tolerate a soft diet after surgery compared with the open group, although there were no statistical differences. Moreover, laparoscopic resection could significantly reduce intraoperative blood loss and postoperative time of hospital stay, which were consistent with the results from other studies.15,17,21,22 In addition, 30-day complications and Clavien–Dindo score showed no statistical difference between the two groups, but showed less frequent 30-day complications in the laparoscopic group. These short outcomes of laparoscopic surgery for T4 colon cancer demonstrated that minimally invasive approach was superior to conventional laparotomy, with faster recovery after surgery.
In our center, preventive stoma was mainly decided by intraoperative anastomotic situation of anastomotic stoma, nutritional status of patients, and gradient of infection. The rate of preventive stoma in the laparoscopy surgery group was comparable to the open group. Our recent study demonstrated that ileostomy closure (<3 months) is practical and safe, with no increasing morbidity. 25 Therefore, we routinely closed the iliac stoma in 3 months.
The rate of conversion to laparotomy ranged from 7.7% to 21% based on some previous studies.15–22 It is well recognized that laparoscopic surgery for pT4 malignant tumor increases the risk of conversion to laparotomy. In the COLOR trial, 17% patients had laparoscopic procedures converted to open surgery intraoperatively, whereas 50% patients with T4 colon cancers were converted to open surgery. 6 Fifteen patients (10.1%) were converted to open surgery intraoperatively in our study. As Vignali et al. 16 already pointed out, this low conversion rate could be explained by the extensive experience of a dedicated surgical team, the exclusion of patients with rectal cancer, and emergency procedures. In addition, the R0 resection is already known as one of the most important prognostic predictors of treatment for locally advanced colorectal cancer.26,27 Reported by some studies, the rate of R0 resection for T4 colon cancer ranged from 88.2% and 88.5% to 100% and 96% in laparoscopic surgery group and open surgery group, respectively.15,17,21,22 The R0 resection rate achieved 100% both in the laparoscopic group and the open group in this study. Moreover, the median of lymph nodes harvested reached 15 and 16 in the laparoscopy group and open group, respectively, which were corresponding with the recommendation of NCCN guideline. 14 Furthermore, a recent meta-analysis of laparoscopic surgery for T4 colon cancer, which included 13 observational cohort studies published between 2012 and 2017, showed no significant differences between laparoscopic and open surgery for oncological outcomes. 28 In our study, the overall survival rate and disease-free survival rate in stage II and stage III disease between laparoscopic surgery group and open surgery group showed no significant differences, which were corresponding with other studies.15–17,19,21,22 Moreover, intraoperative blood loss and perioperative blood transfusion rate have been identified as independent factors on long-term survival.16,29 Our multivariate analyses showed that intraoperative blood loss was a significant independent factor related to a poor prognosis. A single-center retrospective study of 7 years' experience showed locally advanced stages (IIIB–IIIC) and R1 resections were independent prognostic factors for overall survival. 21 However, the overall stage showed no significant relationship with overall survival, which may be explained by selection bias of patient. Altogether, these results suggest that laparoscopic surgery for T4 colon cancer might not endanger the long-term oncological outcomes.
The limitations of this study are retrospective and nonrandomized design of a single center and selection bias of patient. The surgical approach for colorectal cancer in our hospital is mainly based on preoperative imaging results, economic situation of patients, and doctor's preference. However, this study supports us to carry out a minimally invasive laparoscopic procedure for locally advanced colon cancer.
In conclusion, the results of this study suggest that laparoscopic procedure for T4 colon cancer is safe and technically feasible, does not increase the postoperative morbidity, does not adversely affect oncological outcome, and provide faster recovery. Selected patients with locally advanced colon cancer should not be precluded from laparoscopic surgery. Moreover, larger prospective randomized studies are needed to resolve these issues in the future.
Footnotes
Acknowledgments
This work was supported by the Science and Technology Planning Project of Guangdong Province of China (2015A030313729012), and Guangzhou Science Technology and Innovation Commission (201804010073).
Disclosure Statement
All authors have no conflicts of interest or financial ties to disclose.