
Abstract
Abstract
Background and Aims:
The prevailing technique in laparoscopic resection of the right colon has been laparoscopic-assisted procedure with externalization of the bowel for extracorporeal creation of the ileocolic anastomosis. The total laparoscopic technique performing all steps intracorporeally, however, has gained increasing interest. The purpose of this study was to describe our experience with creation of an ileocolic intracorporeal anastomosis (IIA) and to determine anastomotic leakage (AL) rate and short-term outcome of performing IIA.
Materials and Methods:
In the period 2011–2017, 2 surgeons in two centers performed 96 laparoscopic resections of malignant and premalignant diseases in the right colon. A linear stapler was used to construct an isoperistaltic side-to-side anastomosis, closing the residual defect with a running suture. Data regarding the surgical procedure and the postoperative course were recorded prospectively. Complications were defined as postoperative until the 30th postoperative day. Readmission was defined as any readmission related to the surgical procedure within 90 days postoperative.
Results:
AL rate was observed in 4 patients (4.2%, 95% CI = 1.15–10.33). Postoperative complications occurred in a total of 20 patients (20.83%, 95% CI = 13.22–30.33), none of them fatal. Patients with AL had increased risk of other postoperative complications with OR = 14.25 (95% CI = 1.03–757.36, P = .0236) and complications of Clavien-Dindo Grade ≥IIIb (OR = 10.8, P = .012). Smoking was the only factor predisposing to AL. Patients without AL stayed in hospital a median of 3 days, compared with 32 days for patients with AL.
Conclusion:
IIA was found to be a feasible and safe technique in laparoscopic resections of the right colon with an AL rate of 4.2%.
Introduction
O
Many surgeons still favor the laparoscopic-assisted technique with externalization of the bowel through a lateral transverse incision (LTI) for creation of the extracorporeal ileocolic anastomosis (EIA). A total laparoscopic procedure, creating an intracorporeal ileocolic anastomosis (IIA), however, may provide additional benefits with less pain and lower risk of incisional hernia and has regained interest. To date, uncontrolled studies, investigating anastomotic leakage (AL) rates after EIA and IIA, have produced equivocal results.
Aim
The aim of this study is to describe our experience with intracorporeally performed ileocolic anastomosis (IA) in a series of laparoscopic resections of malignant and premalignant disease in the right colon, determining leakage rate and short-term outcomes.
Materials and Methods
Laparoscopic resection of malignant and premalignant disorders in the right colon with creation of an IA was performed in 96 patients from 2010 to 2017 in two centers (Randers, n = 53 and Aarhus, n = 43). One surgeon included patients in Aarhus from August 2010 to August 2015 and one surgeon included patients in Randers from January 2011 to January 2017. Patients scheduled for laparoscopic resection of the right colon were included by the surgeons in a consecutive series.
Patients in Randers all had mechanical bowel preparation (MBP), none in Aarhus. At commencement of anesthesia, all patients received prophylactic antibiotics (cephalosporin and metronidazole). The procedures performed were standard resection (n = 93) or extended resection of the right colon (n = 2), whereas 1 patient with premalignant disorder had an ileocecal resection.
Clinical profile included gender, age, American Society of Anesthesiologists (ASA) score, body mass index (BMI), information about smoking, alcohol, and comorbidity and was obtained from the preoperative anesthesia examination. BMI was calculated using the WHO definition (Table 1).
7 objects a week for females and 14 for males.
ASA, American Society of Anesthesiologists; BMI, body mass index.
Surgical procedure
A small enterotomy was made with diathermy or Thunderbeat (Fig. 1). The IIA was constructed using a linear 60 mm stapler as an isoperistaltic side-to-side IA (Fig. 2). The residual defect created after applying the stapler was sutured laparoscopically using a running Vicryl 3-0® (n = 7), Biosyn (n = 1), or V-loc™ 3-0 (Covidien, Mansfield, MA) (n = 88) suture in one layer (n = 43; Aarhus, Denmark) or two layers (n = 53; Randers, Denmark, Fig. 3). The resected specimen was extracted through a Pfannenstiel incision protected with a wound protector (Alexis®).
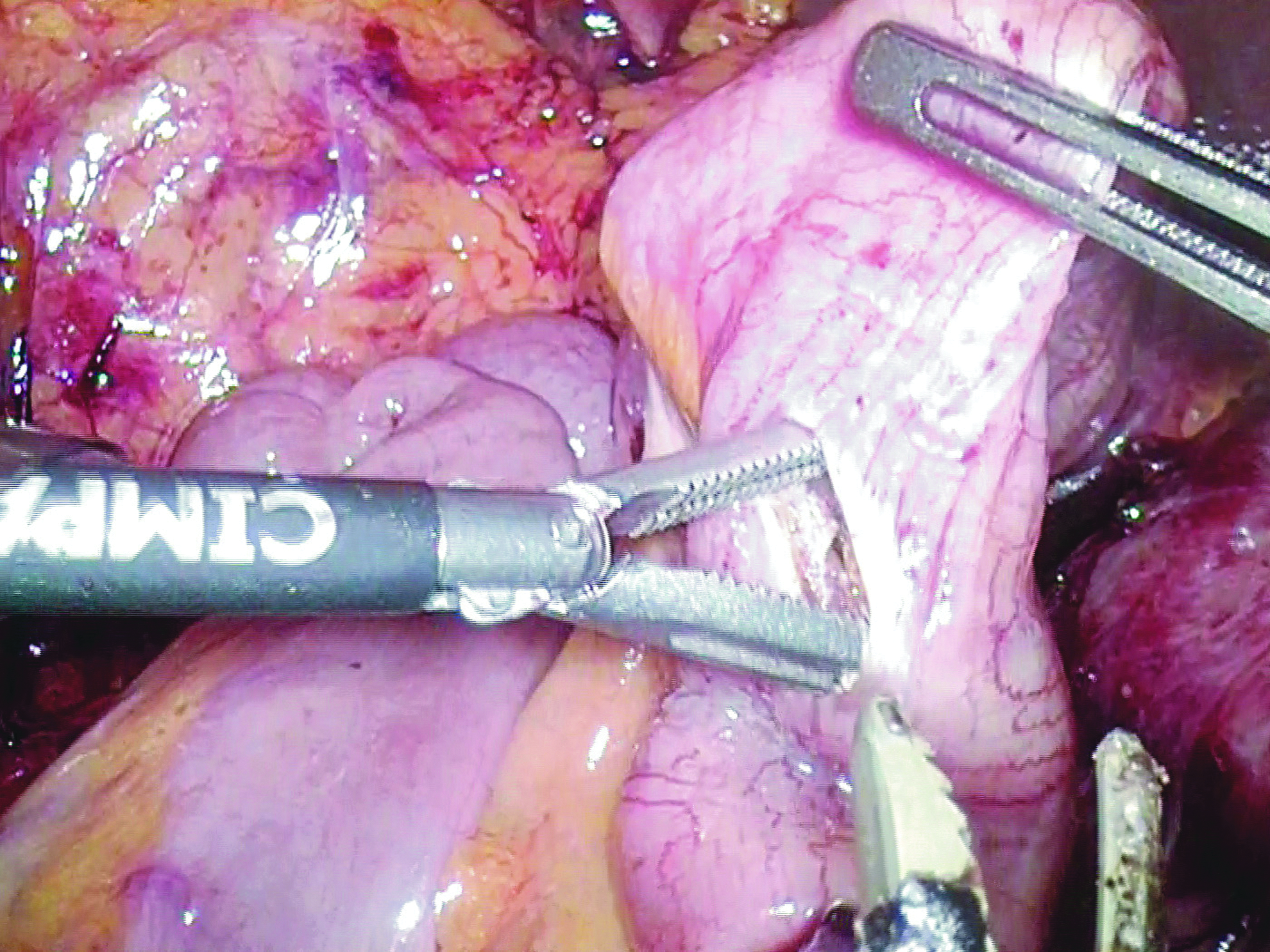
Enterotomy for insertion of stapling device. The enterotomy is made using Thunderbeat and dilated with a forceps grasper. The size of the enterotomy is controlling the size of the defect after stapling.

Insertion of 60 mm linear stapler into the ileum and colon through enterotomies. The stapling device leaves a circular defect that is closed by laparoscopic suturing.
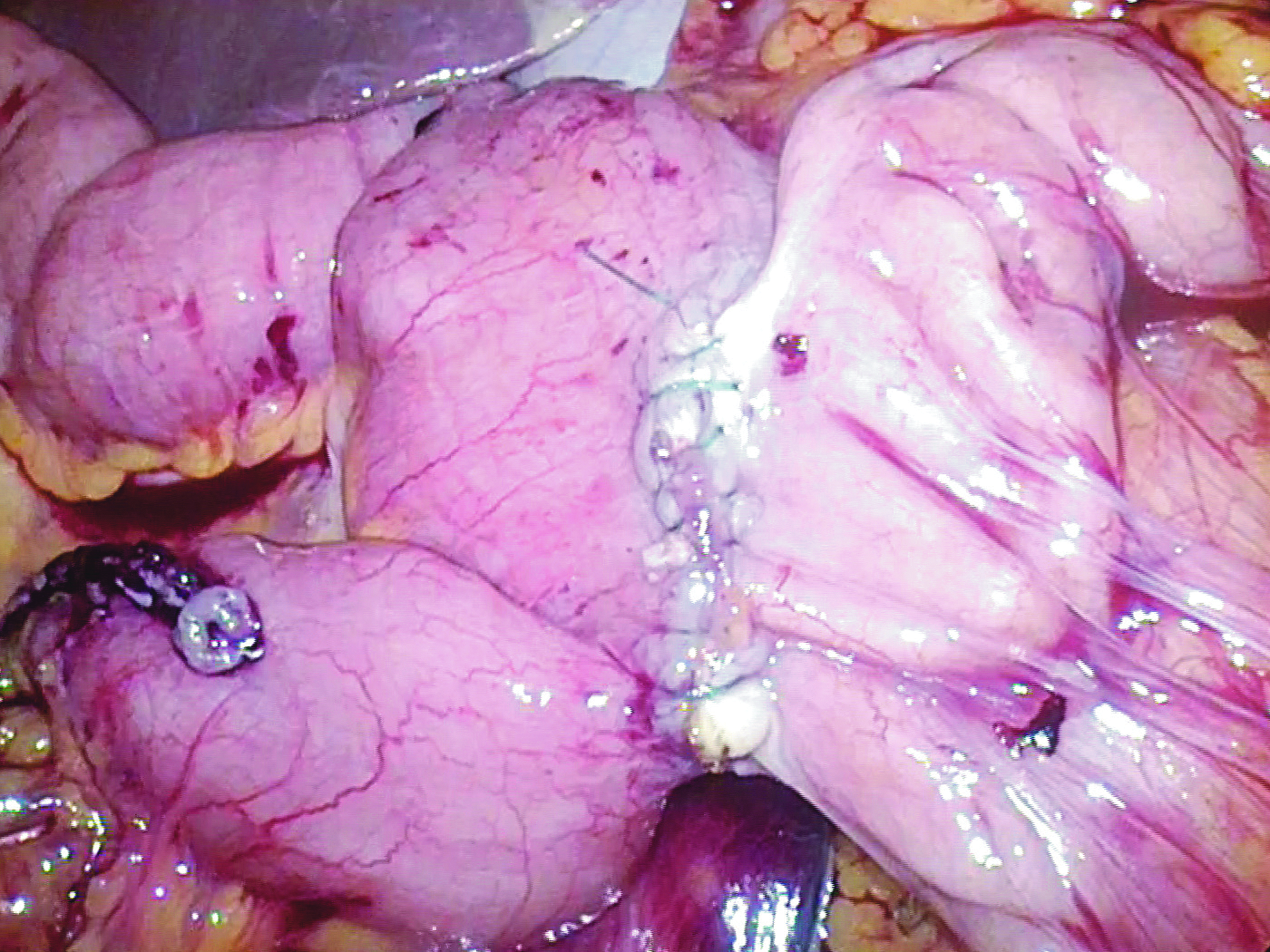
Completed side-to-side isoperistaltic IIA. The defect from stapling is sutured with running V-loc 3-0 in two layers. IIA, intracorporeal ileocolic anastomosis.
Data on surgical procedure, including length of surgery and choice of suture, were registered prospectively. All resected specimens were evaluated by experienced pathologists. In patients with adenocarcinoma Union for International Cancer Control (UICC) stage I–III resection margin, the number of harvested lymph nodes was obtained from the pathologist's evaluation postoperatively.
Definition of endpoints
AL was defined as a leak of gastrointestinal content or the presence of an abscess related to the anastomosis, revealed at reoperation, and requiring surgical correction or lavage. We also recorded whether the leak was located at the stapler or the suture line.
Complications were defined as postoperative occurring within 30 days after surgery and included complications related to the surgical procedure and the hospital admission. Complications were as follows: bleeding other than rectal bleeding, wound infection, fascial dehiscence, pneumonia, pulmonary edema, urinary tract infection, atrial fibrillation, acute myocardial infarction, shock, acute renal failure, and thromboembolic events. Postoperative complications were graded according to the Clavien-Dindo classification. 7
Readmission was defined as any readmission related to the indication for surgery and the surgical procedure within 90 days postoperative. All patients were checked for readmissions at other Danish hospitals retrospectively at the end of the study.
Statistical analyses
Descriptive statistics were used to summarize patients' preoperative characteristics. Continuous variables were reported as median (range: minimum–maximum) due to potential data skewness. Categorical variables were expressed as proportions (%).
Based on clinical relevance, variables were dichotomized: American Society of Anesthesiologists score of three or more and BMI of 25 kg/m2 or more, postoperative complications of Clavien-Dindo Grade IIIb or more, and prolonged operation time was defined as 150 minutes or more. Alcohol use was dichotomized in 7 U a week or more for women and 14 U a week or more for men according to the national guidelines from the Danish Health Authorities.
All tests used a type I error set at α 0.05. Statistical analyses were carried out using Stata software (version 14; SataCorp LLC, Texas).
Ethical consideration
According to national guidelines, the procedure of EIA and IIA performed laparoscopically is not prohibited and the current literature do not support IIA being inferior to EIA. For this type of study, formal consent is not required and we therefore find the study to be ethically sound.
Results
A total of 96 patients were included in the study. Table 1 presents an overview of the clinical profile of the patients. Age ranged between 12 and 92 with a median age of 70 years, similar between genders with a median of 71 years in women and 70 years in men. Patient BMI ranged from 17.5 to 50.8 with a median BMI of 25.5, similar between genders with a median of 24.8 in women and 25.6 in men.
There was no conversion from laparoscopic IIA to laparoscopically assisted EIA or to open surgery. Four patients had AL, resulting in an AL rate of 4.2% (95% CI = 1.15–10.33) with no significant association between BMI above 25 and risk of AL (OR = 2.45, 95% CI = 0.19–131.71, P = .628). Neither were any significant differences in risk of AL found when analyzing: gender (OR = 1.19, 95% CI = 0.08–17.05, P = 1.000) and ASA-score of three or more (OR = 1.04, 95% CI = 0.02–13.79, P = 1.000). No multivariate analysis has been performed. The single clinical profile increasing risk of AL significantly was present smoking (OR = 11.53, 95% CI = 0.84–612.97, P = .037).
As can be seen from Table 2, 16 patients (16.67%) were readmitted within 90 days. In total, 9 patients were assessed to require reoperation. Table 3 presents an overview of indication, method, and findings at reoperation in the 9 patients. In 4 patients AL was confirmed intraoperatively. In 2 of the patients with AL, an end ileostomy and stapled closure of colon sutured to the abdominal wall were constructed during open procedure. One patient with AL was reoperated laparoscopically and converted to open procedure. In this case, an end ileostomy and stapled closure of colon were constructed. In all three cases the leakage was situated in the suture line. The fourth patient with AL presented with a perianastomotic abscess during relaparoscopy. A defect in the stapling line was found after lavage and closed with running suture. Apart from this patient, intraperitoneal infection was not observed, but 3 patients not receiving MBP developed port-site infection.
No complications other than AL.
Number of complications.
AL, anastomotic leakage.
AL, anastomotic leakage; LOS, length of stay; n.a., nothing abnormal; POD, postoperative day.
In further 5 patients, reoperated on clinical or radiological suspicion of AL or suspicion of other complications, the anastomosis was intact. One patient presented with a partial omental necrosis and after laparoscopic lavage in 1 patient with suspicion of intraperitoneal bleeding, no bleeding source could be identified. Four reoperations were completed laparoscopically, while one reoperation was converted to open surgery.
Surgery-related variables are presented in Table 2. Length of surgery ranged from 95 to 269 minutes with a median of 151 minutes. Length of surgery longer than 150 minutes did not show significant increase in risk of AL with OR = 2.63 (95% CI = 0.20–141.35, P = .622).
Postoperative complications occurred in 20 patients (20.83%, 95% CI = 13.22–30.33), none of them fatal. Twenty-three postoperative complications other than AL were observed in 16 patients without AL and eight complications were registered among 3 patients with AL, resulting in increased risk of postoperative complications for patients with AL (OR = 14.25, 95% CI = 1.03–757.36, P = .024). Eleven complications required surgical, endoscopic, or radiological intervention under general anesthesia or were life-threatening complication requiring IC/ICU management (Clavien-Dindo Grade IIIb or more). AL increased the risk of Grade ≥IIIb complications with OR = 10.8 (95% CI = 1.27–128.79), P = .012.
Patients without AL stayed in hospital for a median of 3 days (Range: 1–16) compared with a median of 32 days (Range: 13–54) for patients with AL. The difference in length of stay was significant with P < .0001.
Seventy-one resected specimens with adenocarcinoma and UICC stage I–III were analyzed by pathologists, yielding a median of 25 harvested lymph nodes (range: 12–86) with an R0 and R1 resection margin in 60 and 9 patients, respectively. In two specimens, the resection margin was not established. No specimen had an R2 resection margin.
Discussion
The laparoscopic-assisted colonic resection involves externalization of the bowel through an LTI for extracorporeal creation of the anastomosis. In the total laparoscopic technique, all steps of the procedure are performed intracorporeally, including creation of an ileocolic anastomosis and extraction of the specimen through a transverse suprapubic Pfannenstiel incision. Pfannenstiel incision is reported to offer lower risk of incisional hernia and less postoperative incisional pain compared with LTI.8,9 IIA may lead to faster intestinal recovery, shorter length of stay, and decreased morbidity due to reduced bowel manipulation and reduced traction of the mesentery.10,11 Despite potential benefits of IIA, previous uncontrolled studies did not show significant advantages of the technique.12–15 However, other studies, also uncontrolled, show benefits in short-term morbidity and shorter length of stay and claiming laparoscopic resection with IIA to be a safe and oncologically adequate procedure.16–18
The aim of this study was to describe our experience with intracorporeally performed ileocolic anastomosis in a series of laparoscopic resections of the right colon, investigating leakage rate and short-term outcomes. We present a series of 96 patients ranging widely in clinical profile. Four patients of 96 developed AL resulting in a leakage rate of 4.2%. The single significant difference in clinical profile of the patients between the AL group and the non-AL group was current smoking correlating with findings in other studies. Patients with AL had increased risk of postoperative complications and complications of Clavien-Dindo Grade IIIb or more. Also, patients with leakage had a significantly longer hospital stay than patients without leakage as shown in other studies. Our experience indicates that IIA is feasible in laparoscopic resection of the right colon. There were no conversions to laparoscopic-assisted colonic resections with extracorporeal anastomosis or to open surgery.
The readmission rate of 16/96 and the reoperation rate of 9/96 patients might appear to be high. However, introducing a new laparoscopic method in the department, it is well advised to have a low treshhold for readmission and reoperation as overlooked bowel injuries or delayed diagnosis of AL or other complications may have fatal consequencies.
Advantages of the present study include its prospective design using well-defined selection criteria, including only patients with malignant or premalignant disease, standardized surgical procedure throughout the period of investigation, and a prospective follow-up.
In addition, all resected specimens with adenocarcinoma UICC stage I–III were reviewed by experienced colorectal pathologists ensuring uniformity in the registration of harvested lymph nodes and resection margins. The number of harvested lymph nodes and resection margins in the present study indicate sound oncological quality.
A disadvantage of the present study is the case-series design and the sample size. Insignificant differences between the two techniques (one-layer versus two-layer closure and MBP versus no-MBP) might turn significant in a larger sample size.
AL is a serious complication and has been found to increase recurrence and decrease long-term survival after curative resection for colonic cancer.19,20
When analyzing AL after colonic resection, ileocolic anastomoses need to be analyzed separately from colocolonic or colorectal anastomoses. In ileocolic anastomosis, the involved bowel ends are different with regard to diameter and wall structure. 21 The stapling technique for ileocolic anastomosis differs from distal anastomoses and anastomotic leak rate is higher with distal anastomoses. 22
In a Cochrane review of series from prevailingly open surgery, handsewn ileocolic anastomoses performed side-to-side were compared to functional end-to-end using stapler. The enterotomy remaining after withdrawal of the stapler was closed by stapler or manually sutured. It was concluded that entirely stapled anastomoses were associated with significantly fewer leaks than handsewn anastomoses (2.5% versus 6.1%). 23
A meta-analysis published in 2007 involving patients with Crohn's disease found a higher leakage rate at open surgery when end-to-end anastomosis was performed claiming that side-to-side configuration should be preferred. 24
Creating laparoscopic IIA, however, neither a functional end-to-end using a double stapling tecnique nor an exclusively manually sutured anastomosis is an option. At present, it is constructed as a side-to-side anastomosis by means of a stapler closing the remaining enterotomy by suture. The leakage rate in our study compares favorably with published results of ileocolic anastomoses performed at open surgery.
A systematic review and meta-analysis from 2016 comparing IIA and EIA in 14 uncontrolled studies of 1717 patients found that AL was similar in the IIA and the EIA group (3.4% versus 4.6%, P = .120). 25 The review found the IIA group to have a lower overall complication rate, shorter length of hospital stay, and a trend toward a lower incisional hernia rate. The study found no differences in operative time, conversion rate, reoperation, mortality, and number of lymph nodes harvested. These findings indicate that our leakage rate of 4.2% and a postoperative overall complication rate of 19.8% are equivalent to international standards.
Compared to handsewn anastomosis, the double stapling technique has been reported to be associated with a significantly lower rate of intraoperative spillage of bowel content. 21 In the view of the authors, it confers a theoretical advantage of the functional end-to-end stapling technique. The stapling technique has been claimed to cause less tissue trauma and decreased risk of peritoneal contamination. 24 Intraoperative septic conditions have been shown to be a risk factor for a clinically significant anastomotic leak. 26
The incidence of leakage after either a single-layer (SL) or double-layer (DL) enterotomy closure by running suturing has been shown to be significantly lower for DL closure. 27 In the present study, SL and DL were used to close the residual defect in 43 and 53 patients, respectively. Our insignificant findings of increased risk of AL after DL (OR = 2.52 [0.19–135.37], P = .625) may indicate that DL closure causes more damage to the bowel than SL and the difference may turn significant in a larger sample size. Our only AL after SL closure was not located in the suture line, but the stapler line. We have no estimates that peritoneal spillage nor the time to construct the anastomosis influenced leakage rate.
All 53 patients with DL closure of the residual defect received preoperative MBP compared to none with SL closure. Controlled studies have not found statistically significant evidence that patients benefit from MBP before elective open colonic surgery. 28 We found three cases of port-site infections in patients without MBP compared with none in patients receiving MBP, suggesting that MBP may contribute to reduced risk of contaminating the port-site. However, we have no diagnostics of the agents from the port-site infections, leaving speculation on skin-based or gastrointestinal-originated agents causing the infection. Apart from 1 patient with an abscess related to the anastomotic defect at the stapler line no other intraperitoneal infections were encountered.
Further research should be conducted to explore possible benefits of performing IIA instead of EIA and to investigate the safety of IIA in relation to AL and short-term morbidity and mortality. A blind randomized controlled trial would be of choice, but will, due to the relatively small differences in published results, require inclusion of a vast number of patients not easily obtained. Another option is a prospective collection of data in a multicenter, preferably nationwide database.
Interpretation
Creation of a laproscopic intracorporeal ileocolic anastomosis was found to be feasible and safe in laparoscopic resections in patients with malignant or premalignant disorders of the right colon.
Footnotes
Acknowledgments
All authors have made substantial contributions to the study. JN conducted the research, data interpretation and analysis, preparation of article, and guarantor of the article; TS study design, data interpretation and analysis, and critical review; PW study design, data interpretation and analysis, and critical review. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure Statement
No commercial associations or disclosures may pose or create any conflict of interest with the information presented in this article.