
Abstract
Abstract
Introduction:
Innovative strategies to reduce costs while maintaining patient satisfaction and improving delivery of care are greatly needed in the setting of rapidly rising health care expenditure. Intensive care units (ICUs) represent a significant proportion of health care costs due to their high resources utilization. Currently, the decision to admit a patient to the ICU lacks standardization because of the lack of evidence-based admission criteria. The objective of our research is to develop a prediction model that can help the physician in the clinical decision-making of postoperative triage.
Materials and Methods:
Our group identified a list of index events that commonly grants admission to the ICU independently of the hospital system. We analyzed correlation among 200 quantitative and semiquantitative variables for each patient in the study using a decision tree modeling (DTM). In addition, we validated the DTM against explanatory models, such as bivariate analysis, multiple logistic regression, and least absolute shrinkage and selection operator.
Results:
Unlike explanatory modeling, DTM has several unique strengths: tree models are easy to interpret, the analysis can examine hundreds of variables at once, and offer insight into variable relative importance. In a retrospective analysis, we found that DTM was more accurate at predicting need for intensive care compared with current clinical practice.
Discussion:
DTM and predictive modeling may enhance postoperative triage decision-making. Future areas of research include larger retrospective analyses and prospective observational studies that can lead to an improved clinical practice and better resources utilization.
Introduction
T
At present, due to the lack of well-established guidelines, postoperative triage decision-making is highly variable among different hospitals, leading to greatly different admission rates to ICUs after major surgery, ranging from 2.7% to 88%. The process is based on clinical judgment of patient factors (e.g., age, comorbidities, type of surgery, and intraoperative events), systemic factors (e.g., bed availability, operating room schedule, local clinical culture, and medicolegal climate), and physician factors (e.g., personality, specialty, training, type of practice, prior experience, and input from consultants)6,7 (Fig. 1).
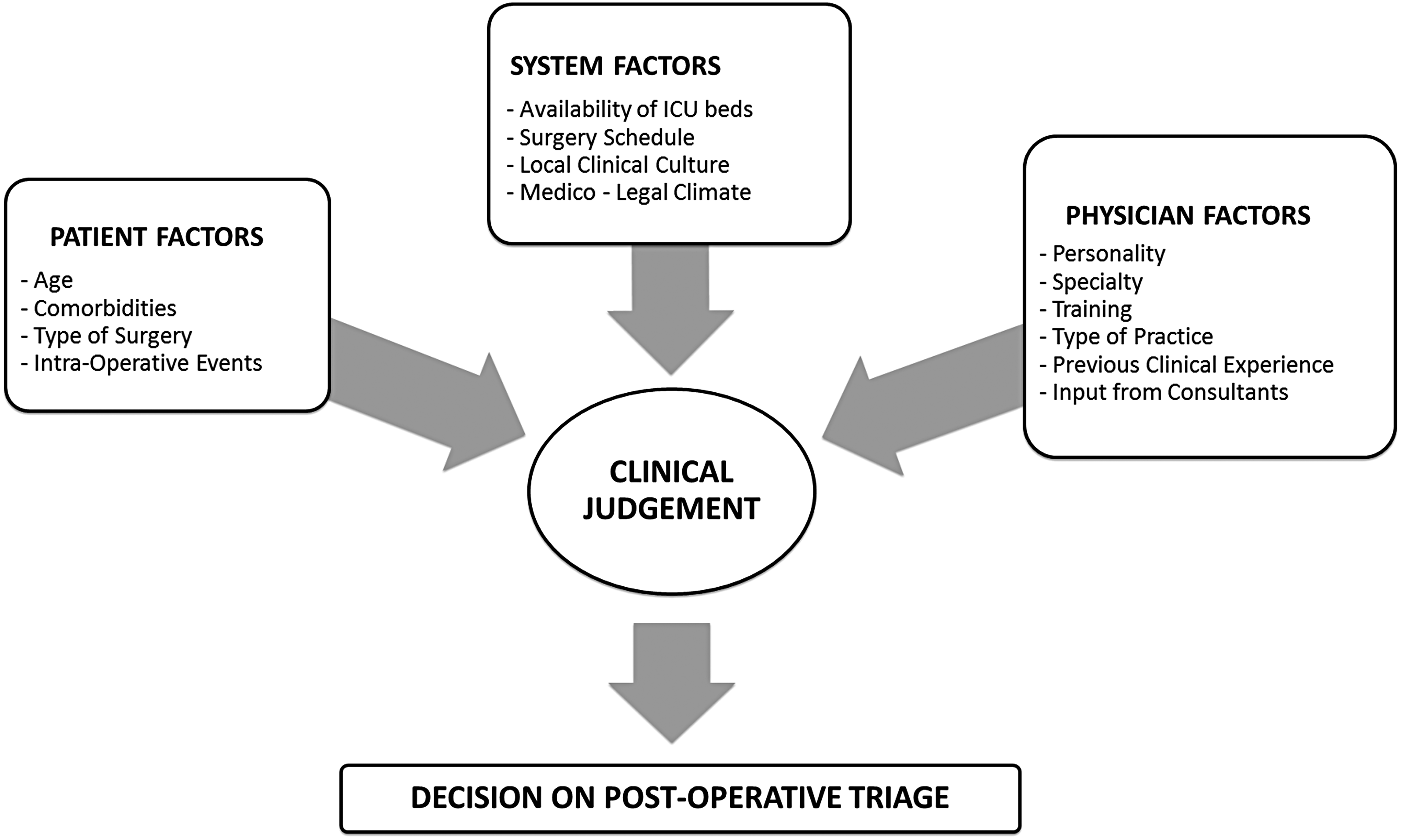
Conceptual model.
Current available guidelines and recommendations for ICU triage from the Society of Critical Care Medicine, from the Council of the World Federation of Societies of Intensive and Critical Care Medicine,5,6 and from different national societies including the European Society of Intensive Care Medicine, 8 the American College of Critical Care Medicine, 6 the Italian Intensivist Group, 9 are used for the triage process in general but are not specific for the surgical nor for the postoperative triage of the hemodynamically stable patient. 10 Several models have also been proposed to aid in the prediction of postoperative outcomes: the Veterans Affairs Surgical Quality Improvement Program, National Surgical Quality Improvement Program, Charlson comorbidity index (CCI), revised cardiac risk index (RCRI), and surgical Apgar score (SAS) are just some among the many.
Since the risk of postoperative complications is directly related to both preoperative conditions, magnitude of surgery, and intraoperative events, our study aimed at investigating the role of commonly used surgical risk scores in identifying patients who would benefit from postoperative admission to the ICU. Of the new risk scores, we decided to include the SAS, since we previously validated it in a similar population. 11
Materials and Methods
Currently, no objective criteria for appropriate ICU admission have been codified in the literature, thus we developed a list of “index events” (Table 1) that would usually grant admission to the ICU independently of the hospital system. We analyzed correlation between occurrence of at least one of those “index events,” commonly used clinical risk scores (e.g., CCI, RCRI, and SAS), objective patient data (age, blood losses, heart rate, etc.), and semiqualitative patient data (e.g., presence or absence of a certain condition). More than 200 quantitative and semiquantitative variables have been collected for each patient and a decision tree modeling (DTM) technique was used to investigate any correlation between clinical variables and the need for ICU.
ICU, Intensive care unit.
Results
Using DTM techniques on preliminary data on 368 patients, we found that although SAS and the other surgical risk scores were factors highly correlating with the need of ICU, they were not the top predictors identified by the DTM. In testing the model, patients were triaged to an appropriate level of care with an accuracy of 86% compared with the 37% of our current practice. In addition, we validated the DTM against explanatory models, such as multiple logistic regression and least absolute shrinkage and selection operator, and found it to be superior in accuracy by 2.6% and 4.5%, respectively.
Discussion
DTM is a form of predictive modeling that results in a classification system that can be used to predict future observations using a set of decision rules.12,13 The resulting tree diagrams are easy to interpret and offer a highly streamlined process for complex decision-making. Predictive modeling has several advantages over explanatory modeling (e.g., bivariate analysis and multiple logistic regression). For example, it can deal with numerous variables types, account for missing data using surrogate variables, and, most importantly, provide variable rank, which measures the importance of each predictive factor. For this reason, predictive modeling does not require an a priori hypothesis as to which variables are most important. Instead, it is able to consider every single variable of interest and then sort them by importance based on the model. Conversely, explanatory modeling requires variable selection and can only assess a restricted set of variables at once as it is limited by the large p/small n problem, where the number of predictors exceeds the number of subjects. Consequently, the selection of variables to be included in explanatory modeling would introduce a concerning source of bias. Furthermore, relevant variables can be missed if they are not selected for inclusion in the analysis. For all these reasons, we found DTM to be the ideal technique to develop an objective clinical model for postoperative triage.
There are many additional considerations to be addressed for postoperative triage optimization after major surgery. For instance, the accuracy of clinical judgment (the accepted standard of care) in determining the appropriate level of postoperative care is unknown.
As a second part of our study, we planned a prospective pilot observational study to investigate whether objective clinical parameters may outperform subjective clinical judgment in triaging patients to the most appropriate level of care. The main challenge with this type of study, however, is to identify which patients would benefit from an ICU admission. For instance, an ICU patient may receive a timelier resuscitation compared with a patient in the regular ward. Whether that timely intervention would result in the avoidance of a complication remains impossible to determine, despite prospective data collection. To partially overcome this limitation, for such pilot study we decided to focus solely on those patients for whom ICU admission was clearly clinically indicated. The downside of this approach is the loss of sensitivity in identifying who benefits from ICU admission, along with a corresponding increase in specificity.
This study has the potential to be very significant for several reasons. First of all, the study provides measurable parameters that define an objectively appropriate ICU admission. It assesses the accuracy of both measurable data and subjective clinical judgment for postoperative triage. This type of study also provides the background data for future research on the efficacy of implementing objective decision-making tools to improve postoperative triage of patients undergoing major surgery. Ultimately, this research provides substantial contribution to enhance patient care, cut hospital costs, and improve measurement of performance quality while clarifying the clinical decision-making process of postoperative patients.
Footnotes
Disclosure Statement
No competing financial interests exist.