
Abstract
Abstract
Introduction:
Laparoscopic complete mesocolic excision (CME) for transverse colon cancer is technically challenging. Robotic technology has been developed to reduce technical limitations of laparoscopy. Yet, no data are available on the role of robotic approach for CME of transverse colon cancer. The aim of this study is to evaluate the feasibility and short-term outcomes of robotic CME in this subset of colon cancer.
Methods:
A retrospective review of a prospectively maintained database of 29 consecutive patients undergoing robotic CME for transverse colon adenocarcinoma between December 2014 and December 2017 was performed. Data on demographics, tumor characteristics, postoperative 30-day complications, and oncologic outcomes were analyzed.
Results:
There were 21 (72%) men and 8 women with a mean age of 62.9 ± 15.6 years and a body mass index of 26.4 ± 4.8 kg/m2. Of the 29 robotic CME procedures, 12 patients underwent extended right colectomy, 10 extended left colectomy, 6 subtotal colectomy, and 1 total colectomy. The mean operative time was 321.7 ± 111.3 minutes and estimated blood loss was 106.9 ± 110.9 mL (median, 50; range, 10–400 mL). The intra- and postoperative complication rates were 7% and 24%, respectively. There were no conversions. The mean time to first bowel movement was 3.5 ± 1.3 and length of hospital stay was 7.1 ± 3.0 days. All the resections were R0. The mean number of harvested lymph nodes in extended and subtotal/total colectomy procedures was 36.6 ± 13.1 and 71.0 ± 30.3, respectively. The rate of mesocolic plane surgery was 79%. There were no statistically significant differences between the mesocolic and the intramesocolic/muscularis propria plane resections with respect to clinical characteristics, operative outcomes, and pathology results (P > .05).
Conclusions:
Robotic CME for transverse colon cancer is feasible and can be a procedure of choice to achieve a good surgical quality.
Introduction
There is a growing interest in complete mesocolic excision (CME) for the oncologic resection of colon cancer following its introduction by Hohenberger et al. in 2009. 1 The CME technique in which the root of colonic arteries are tied centrally and the mesocolon with its lymph nodes is radically excised as a package in the embryological plane has been shown to produce a higher degree of lymphadenectomy, fewer local recurrences, and better long-term survival compared with standard non-mesocolic excisions.1–3 Initially, CME was purely an open procedure, and eventually, the feasibility of laparoscopic approach has been reported with the advantages of minimally invasive surgery, including faster postoperative recovery and shorter hospital stay.4,5
Noticeably, transverse colon cancers have often been excluded from many studies carried out on the laparoscopic approach, including the COST, COLOR, and CLASICC trials.6–8 The most commonly stated reasons for this exclusion are, in addition to low incidence of transverse colon tumors, technical difficulties associated with ligation of the middle colic vessels and performing lymphadenectomy around the middle colic artery (MCA) by laparoscopy.9–12 Although few studies reported the feasibility of laparoscopic CME for transverse colon cancer,10–14 the evidence remains limited.
In the last two decades, robotic surgery has gained increasing acceptance in colorectal procedures due to its inherent advantages overcoming the technical limitations of laparoscopy. However, no report exists regarding the role of robotic approach in CME of transverse colon cancer. Regarding the lack of data, this study was conducted to report the feasibility of this procedure, and present details of our operative technique and oncologic outcomes.
Methods
Patients
After obtaining approval from the Institutional Ethics Committee, we evaluated prospectively collected data of 29 consecutive patients undergoing robotic CME for transverse colon adenocarcinoma between December 2014 and December 2017. Research electronic data capture (REDCap) 15 was used for data collection. Transverse colon cancer was defined as a tumor located between the hepatic and splenic flexures, including the flexures. Patients with a transverse colon and a synchronous colonic tumor requiring ligation of the MCA at its origin were included. In this series, the tumor was localized to the hepatic flexure in 6 patients, proximal transverse colon in 2, mid transverse colon in 3, distal transverse colon in 3, and splenic flexure in 10 patients. Each of the 5 remaining patients had a synchronous colonic tumor elsewhere in addition to transverse colon cancer.
Preoperatively, a computed tomography scan of the abdomen and thorax was performed to determine the clinical tumor stage. Bowel preparation protocol included a fiber-free diet for 2 days and sodium phosphate soda and enema 1 day before surgery. All the patients received venous thrombosis and antibiotic prophylaxes. Postoperative pain control was provided by intravenous narcotics as needed. Discharge criteria were sufficient oral intake, full ambulation and adequate pain control with oral analgesics.
Data collected were patient demographics, operative and histopathological results, and postoperative 30-day and oncologic outcomes. Docking time was defined as the time from moving the robot in the surgical field to setting the robotic arms into the port sites. The overall operative time was defined as the time from the first skin incision to the end of skin closure. Conversion was defined as the completion of any part of the procedure with an open or standard laparoscopic technique, excluding the delivery of the specimen, and placement of the stapler anvil for stapled ileocolic/ileorectal anastomosis in subtotal/total colectomy procedures. The quality of the mesocolic dissection was graded as mesocolic (smooth intact mesocolic excision with high vascular ties), intramesocolic (disruption of the mesocolon, but the incisions do not reach down to the muscularis propria), or intramuscularis propria plane (exposed muscularis propria). 16
Operative technique
In all the patients, the operations were carried out with a full robotic technique using the da Vinci Xi® Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA). CME with central vascular ligation was performed using the medial-to-lateral approach and bowel anastomosis was created intracorporeally. Resections were performed to achieve at least 10-cm proximal and distal tumor-free margins.
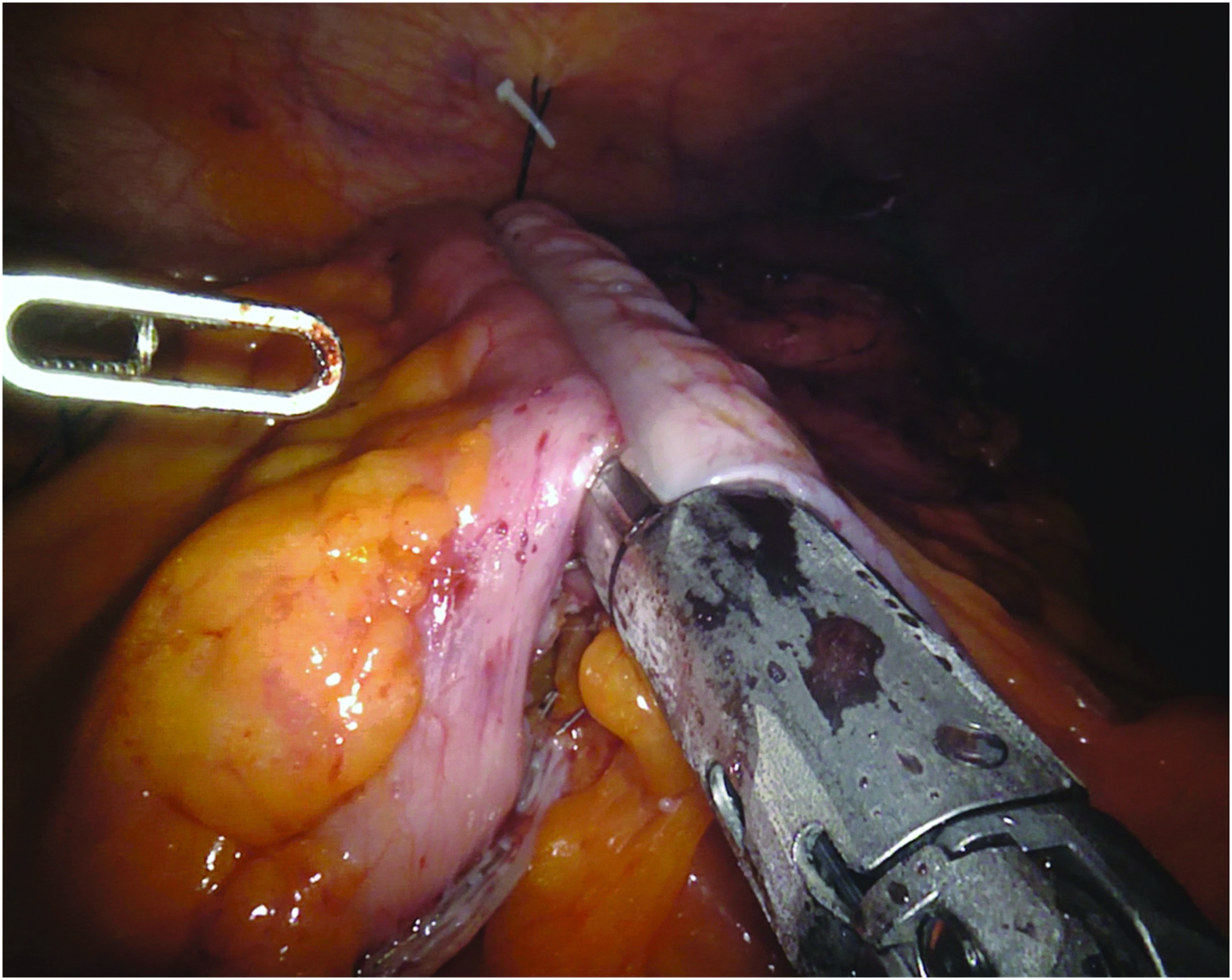
For tumors localized to the hepatic flexure, proximal, or mid transverse colon, an extended right CME hemicolectomy was performed. In this procedure, we initially performed a caudal-to-cranial dissection technique in our early experience and then adopted a cranial-to-caudal (top-to-down) technique, as described below. Figure 1 shows trocar placement. In the caudal-to-cranial technique, the patient was placed in a modified lithotomy with a 15-degree Trendelenburg and a 30-degree left tilt position. The robot was docked from the right side of the patient. Dissection was initiated by retracting the ascending mesocolon near the ileocecal junction anteriorly and laterally with the tip-up grasper. The peritoneum overlying the ileocolic vascular pedicle was lifted up with bipolar forceps and incised with monopolar scissors. First, the ileocolic vein, and then, the ileocolic artery were isolated individually, clipped with 5-mm clips near its origin from the superior mesenteric vein (SMV) and superior mesenteric artery (SMA) and divided. Dissection was continued superiorly along the ventral side of the SMV, dissecting out the entire mesocolic tissues until the second portion of the duodenum and head of the pancreas were reached. During this dissection process, the right colic artery, if present, was divided near its origin in the same fashion. Careful dissection onto the duodenum and the inferior border of the neck of the pancreas was performed. In this study, the middle colic vein (MCV), anterior superior pancreaticoduodenal vein, and superior right colic vein were isolated, clipped, and divided (Fig. 2). The MCA was identified arising from the SMA and divided at its root. This was followed by radical lymph node dissection along the anterior and lateral side of the SMV. Then, the embryological tissue plane between the pancreas and the transverse mesocolon was separated. During this dissection, the lymph nodes in the subpyloric region and over the pancreatic head were removed. With caudal traction of the transverse colon, the lesser sac was entered and the gastrocolic ligament was divided from left to the right along the greater curvature of the stomach. The right half of greater omentum at a length of 10–15 cm from the tumor was dissected off to include it with the final specimen. The medial-to-lateral mesenteric dissection was completed staying between the embryological planes just over the Toldt's fascia. Following completion of CME, the terminal ileum and the transverse colon were transected sequentially using robotic EndoWrist® staplers (Intuitive Surgical, Inc.) and a side-to-side stapled ileocolic anastomosis was created (Fig. 3).
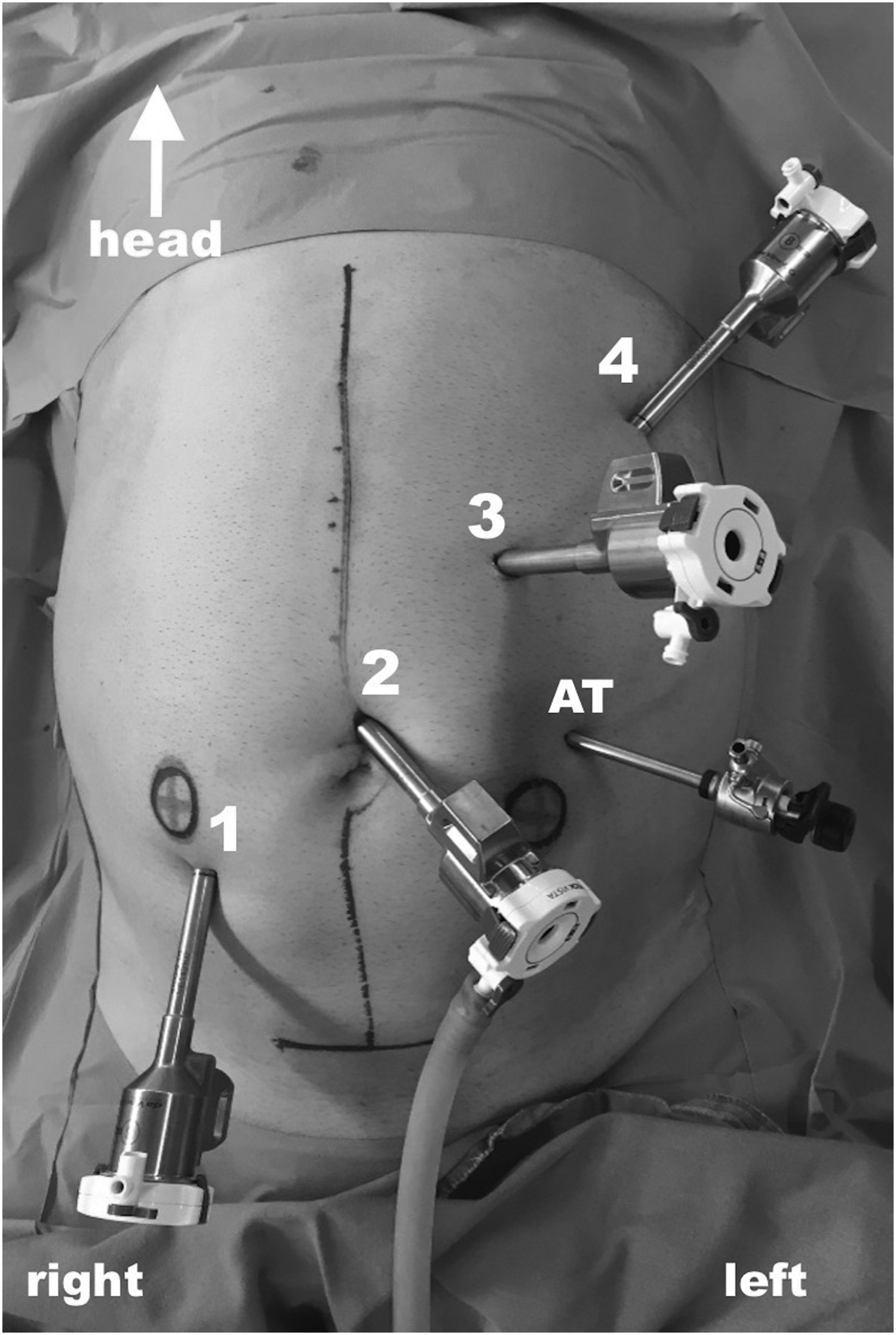
Trocar placement for robotic right extended CME hemicolectomy. Camera was introduced at trocar #2 (8 mm), double fenestrated bipolar forceps at trocar #1 (8 mm), monopolar curved scissors at trocar #3 (8 mm), and double fenestrated tip-up grasper at trocar #4 (8 mm). Later in the operation, the trocar #4 was changed to a 12-mm trocar to introduce the stapler for bowel transection and anastomosis. AT, assistant trocar; CME, complete mesocolic excision.

Dissection of the root of the middle colic vein.
Intracorporeal stapled side-to-side ileocolic anastomosis.
In the cranial-to-caudal technique, all the operative steps were the same as those described above with the exception that dissection was initiated superiorly to allow easy access to and early vascular control of the gastrocolic trunk of Henle and middle colic vessels. 17 For this, the patient was first placed in a 15-degree reverse Trendelenburg and a 30-degree left tilt position. First, the omental bursa was opened and the right gastroepiploic vein was identified. Using this vein as a landmark, dissection was continued caudally to expose the gastrocolic trunk. The right gastroepiploic vessels, branches of the gastrocolic trunk, and the main pedicles of the MCV and MCA were divided in a similar fashion. After this step, the robotic arms were demounted and the patient was placed in a Trendelenburg position to expose the ascending mesocolon. The transverse colon was raised ventrally and dissection was continued in an inferior-to-superior fashion along the SMV, dividing the ileocolic and right colic vessels (if present). Finally, the ascending and transverse mesocolon was separated from the retroperitoneal tissues, completing CME.
For tumors localized to the splenic flexure, an extended left colectomy was performed, as described previously. 18 Figure 4 shows trocar placement. The patient was placed in a 30-degree Trendelenburg position with a 30-degree right tilt. The robot was docked from the left side of the patient. First, the descending mesocolon was raised with a tip-up grasper and the retroperitoneal plane was entered over the inferior mesenteric vein (IMV). The IMV was isolated and divided at the inferior edge of the pancreas. Dissection was carried out in a cranial-to-caudal manner using bipolar forceps and monopolar scissors. The inferior mesenteric artery (IMA) was skeletonized until the left colic artery appeared. The left colic artery was then clipped and divided at its origin. Next, the mesentery of the descending colon was mobilized from the ligament of Treitz. Dissection was carried out along the embryological tissue plane between the anterior surface of the pancreas and the mesocolon, which enabled entry into the lesser sac (Fig. 5). This was followed by radical lymph node dissection in the lateral left gastroepiploic vascular curvature. Dissection was continued down to the inferior border of the neck of the pancreas where the root of the MCA was isolated, clipped, and divided. Similarly, the MCV was divided before its confluence with the gastrocolic trunk or SMV. The medial-to-lateral mesenteric dissection was performed to the lateral peritoneal reflection, staying in the embryological plane just over the Toldt's fascia. The lateral peritoneal reflection of the colon was incised from bottom to top, joining the medial dissection of the mesocolon. The splenocolic ligament was divided, completing splenic flexure mobilization. Then, the gastrocolic ligament was divided all the way to the major curvature of the stomach, releasing the distal half of the transverse colon. The left part of the omentum was removed en bloc with the final specimen. Finally, the transverse colon and descending colon were transected sequentially and a stapled colocolic anastomosis was created.
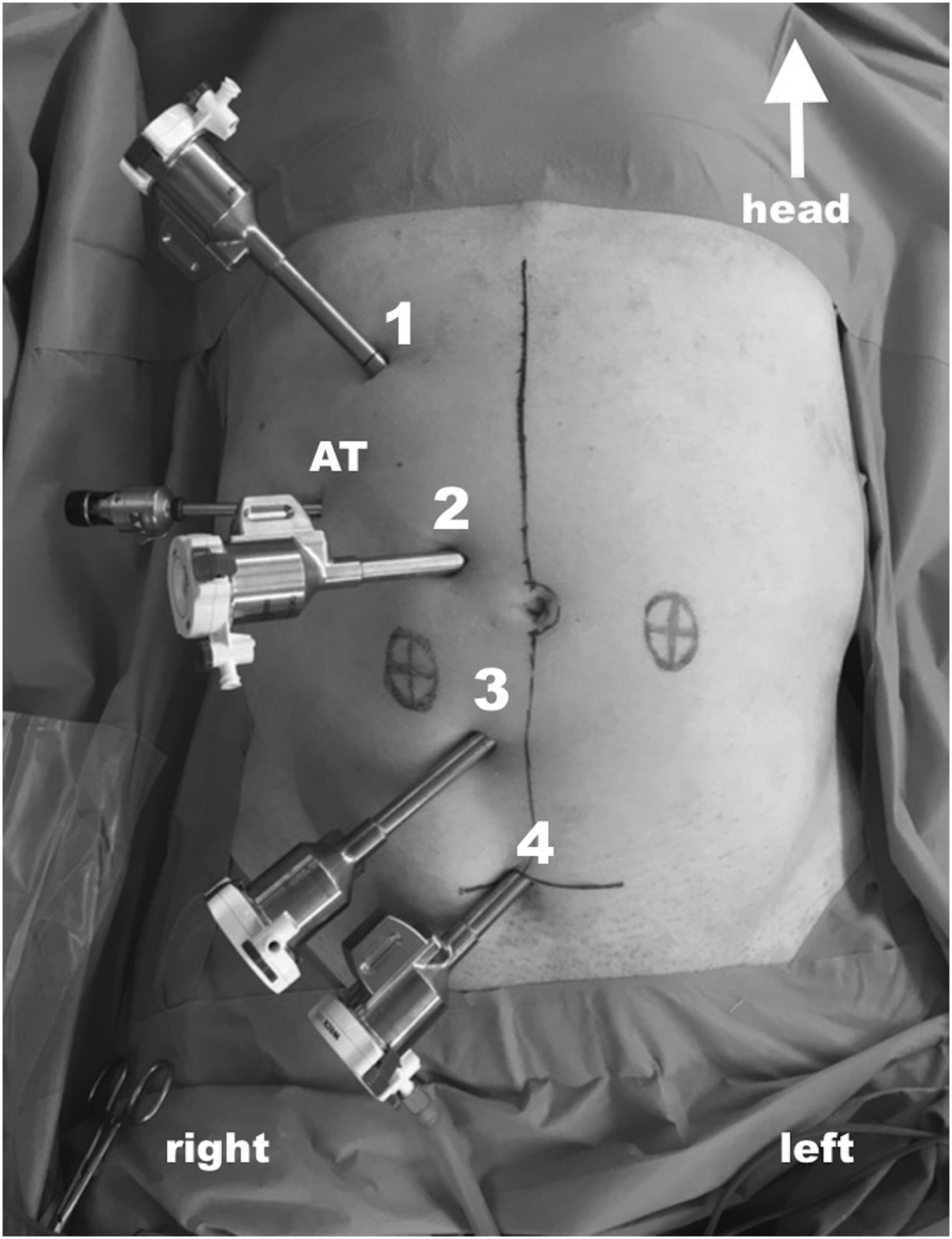
Trocar placement for robotic left extended CME hemicolectomy. Camera was introduced at trocar #2 (8 mm), double fenestrated bipolar forceps at trocar #1 (8 mm), monopolar curved scissors at trocar #3 (8 mm), and double fenestrated tip-up grasper at trocar #4 (8 mm), later in the operation, the trocar #3 was changed to a 12-mm trocar to introduce the stapler for bowel transection and anastomosis. AT, assistant trocar; CME, complete mesocolic excision.

Separation of the mesocolon from the pancreas.
A subtotal colectomy was performed for tumors localized to the distal transverse colon. In patients with synchronous colonic tumors, an extended right, extended left, subtotal, or total CME colectomy was performed depending on the location of the second lesion. For a subtotal or total colectomy, the robot was first docked from the right side of the patient to perform the right side of colectomy as in the aforementioned extended right CME hemicolectomy procedure and then, without moving the robot, the boom of the robotic cart was rotated to the left side to complete the operation as in the extended left CME hemicolectomy procedure. The subtotal and total colectomy procedures included ligation of the root of the ileocolic, right colic (if present), MCA, and IMA. In these procedures, the bowel anastomosis was performed using a transanally inserted circular stapler.
In all the operations, the specimen was extracted through a suprapubic transverse incision with wound protection or within an endobag through a 15-mm laparoscopic trocar introduced at the suprapubic incision. No abdominal drain was routinely placed.
Statistical analysis
Categorical measures were summarized using frequencies and continuous measures were described as mean and standard deviations. The outcome measures were compared between the mesocolic and the intramesocolic/muscularis propria plane resections using the Mann–Whitney U test or Fisher's exact test. SPSS Statistics Version 23.0 (IBM Corp., Armonk, NY) was used for this analysis. P < .05 was considered statistically significant.
Results
Patient demographics, clinical characteristics, and operative procedures are provided in Table 1. Of the 29 patients, there were 21 (72%) men and 8 women with a mean age of 62.9 ± 15.6 years and a mean body mass index of 26.4 ± 4.8 kg/m2. One patient with a splenic flexure tumor had a clinical presentation of complete bowel obstruction, thus a subtotal CME colectomy was performed. Among the 5 patients with synchronous tumors, an extended right colectomy was performed in 1 patient with hepatic flexure and ascending colon tumors; an extended left colectomy in 1 patient with mid transverse colon and splenic flexure tumors; a subtotal colectomy in 1 patient with splenic flexure and cecal tumors, and in the other patient with splenic flexure and appendiceal tumors. A total colectomy was performed in 1 patient with splenic flexure tumor, cecal tumor, and a high-grade dysplastic lesion in the ascending colon.
Demographics, Clinical Characteristics, and Operative Procedures
BMI, body mass index; ASA, American Society of Anesthesiologists; SD, standard deviation.
Perioperative outcomes are provided in Table 2. The mean operative time and estimated blood loss were 321.7 ± 111.3 minutes and 106.9 ± 110.9 mL, respectively. There were no conversions to laparoscopy or open surgery. Overall, an intraoperative complication occurred in 2 patients (7%) and this was a vascular injury in a right extended colectomy procedure in each patient. Both of these injuries involved a small branch of the right colic vein and were repaired uneventfully with intracorporeal 5/0 Prolene sutures. Postoperatively, the mean time to first bowel movement was 3.5 ± 1.3 and length of hospital stay was 7.1 ± 3.0 days.
Operative Findings and Postoperative Outcomes of Robotic Complete Mesocolic Excision for Transverse Colon Cancer
SD, standard deviation.
The postoperative complication rate was 24%, and included pulmonary embolism in 1 patient, nosocomial pneumonia in 1, atelectasis in 1, adynamic ileus in 2, and wound infection in 2 patients. Pulmonary embolism was treated with heparin therapy. The patient with pneumonia and the other with atelectasis were successfully managed with medical therapy. The 2 patients with ileus were effectively managed with nasogastric tube decompression. For wound infections, local drainage of the incision site was required. There was no anastomotic leak.
Histopathological findings are presented in Table 3. All resections were defined as R0. The mean number of harvested lymph nodes in extended and subtotal/total colectomy procedures was 36.6 ± 13.1 and 71.0 ± 30.3, respectively. The mean length between the vascular tie and the tumor was 14.1 ± 4.9 cm. Twenty-three cases (79%) belonged to the mesocolic plane, with a complete and integrated excision of mesocolon and root ligation of supply vessels. Comparison of the outcomes between the mesocolic and the intramesocolic/muscularis propria plane resections revealed no statistically significant differences with respect to clinical characteristics, operative outcomes, and pathology results (P > .05) (Table 4). At a mean follow-up time of 19 ± 9.7 months, there were no recurrences or disease-related mortality.
Pathology Results
CME, complete mesocolic excision; LN, lymph node; SD, standard deviation.
Comparison of Clinical Characteristics, Operative Outcomes, and Pathology Results Between the Mesocolic and Intramesocolic/Muscularis Propria Plane Surgery
BMI, body mass index; LN, lymph node; SD, standard deviation.
Discussion
The present study shows that robotic CME can achieve a complete oncologic resection with good short-term postoperative results. The technical advantages of the robotic system with stable three-dimensional magnified visualization and a high degree of articulating instruments are very useful for clarifying the embryological planes, precisely dissecting the root of the mesocolic vessels, performing a radical lymphadenectomy, mobilizing both colonic flexures, and creating an intracorporeal anastomosis.
In the field of robotic colon surgery, similar to laparoscopy, the predominant use of robotic approach has been for right- or left-sided colectomies and this approach for transverse colectomy has rarely been described. Recently, only two studies specifically indicating the safety and feasibility of robotic surgery for transverse colon cancer have been reported, and in both studies, resections were performed using a standard non-CME colectomy procedure.19,20 In the first study, 19 the authors report three consecutive cases of a premalignant tumor. In this small series, the total operative time ranged from 297 to 408 minutes with no intraoperative complications and no conversions. The maximum number of harvested lymph nodes was 8. All the patients were discharged within 9 days, and after a median follow-up of 72 months, no local or systemic recurrences were noted. In the second study, 20 22 consecutive patients undergoing robotic transverse colectomy were compared with 22 matched patients undergoing laparoscopic colectomy. No differences were noted between the two groups regarding intraoperative complications, median blood loss, postoperative pain, mean time to regular diet, and length of hospital stay. The robotic group had significantly longer operative times (260 minutes versus 225 minutes). There were no conversions in the robotic group, whereas two laparoscopic cases were converted due to uncontrolled bleeding and technical difficulty in middle colic pedicle dissection. Postoperative complications were similar and the mean number of lymph nodes harvested did not differ between the groups (17.5 ± 5.4 versus 19.1 ± 3.4).
In minimally invasive surgery for transverse colon tumor, the technical challenges are obviously higher in the CME procedure than in the standard colectomy because of the need for a more extensive dissection in the presence of complex vascular anatomy. Because of this high technical demand, the advantages of robotic surgery can be maximized when performing the CME procedure for a radical oncologic resection.
In the presented series, the key concepts of CME were successfully applied in every case, including central vascular ligation; lymph node dissection in the subpyloric region, over the pancreas, in the infrapancreatic region, and along the gastroepiploic arcade; bowel transection within a distance of 10 cm from the tumor; and resection of the omentum in relation to the location of the tumor, as suggested by Hohenberger et al. 1 Of note, misrecognition of the vascular anatomical variations, especially at the gastrocolic trunk of Henle may lead to troublesome hemorrhaging and controlling can be difficult. 21 Therefore, in our later experience with extended right colectomy procedure, we adopted the so-called “top-to-down” dissection technique 17 and this technique provided early identification of the gastrocolic trunk and a well-controlled access to the vascular pedicles in these patients.
The number of harvested lymph nodes is regarded as an important surrogate marker for surgical quality1,2 and crucial for prognosis, as suggested by studies indicating that enhanced lymph node harvesting significantly improves survival in stage I–III colon cancers.22,23 There are some concerns regarding adequate lymphadenectomy by laparoscopic transverse colectomy since dissection of the regional lymph nodes around the MCA can be challenging.9–11,20 Additionally, the integrity of the visceral mesocolic layer should be preserved along the entire specimen as incidental tears may lead to tumor spread into the peritoneal cavity. 1 Similar to the total mesorectal excision grading, which has been demonstrated to be an accurate surrogate marker for disease recurrence in rectal cancer, 24 this notion has also been supported by studies showing a better oncologic outcome for mesocolic plane of resection in respect to both intramesocolic and muscularis propria planes of surgery.25,26 The present study supports that these two important aspects of the CME are technically feasible with the robotic approach. Excluding the subtotal and total colectomies in this series, the mean number of 36.6 harvested lymph nodes is higher than that of the majority of laparoscopic or open transverse colon CME series, ranging between 16.2 and 40.10–13,27 Regarding mesocolic integrity, CME completeness was graded as the mesocolic plane in 79% of the patients. This parameter for transverse colon cancer surgery has been assessed in only one laparoscopic CME study, in which the mesocolic plane was achieved in 21 of 24 patients (88%). 10
Nowadays, extracorporeal anastomosis is commonly performed in laparoscopic colectomies. This is because the intracorporeal anastomosis is considered one of the most technically challenging maneuvers in laparoscopy. 28 On the other hand, the intracorporeal technique is suggested to provide important advantages, such as less dissection of the colon for a tension-free anastomosis, less tissue stretching, and reduction of incision length for specimen extraction. 29 In every case, we carried out an intracorporeal anastomosis and we can state that the EndoWrist feature and improved dexterity of the robotic arms simplify this demanding step of the operation.
As can be noted, all the operations in this series require dissection in different quadrants of the abdominal cavity. In fact, working volume limitations of the robot may be one of the reasons why robotic approach has not been widely applied for multiple-quadrant surgery, including transverse colectomy. The multiquadrant access feature of the latest generation of da Vinci robotic system, the Xi model, with its wider range of motion and thinner arms was designed to overcome this limitation perceived in its previous model. 30 This study demonstrated that a single docking of the robot is feasible for both extended right and left colectomies. Even in subtotal and total colectomy procedures, the rotational function of the robotic boom obviates the need for time-consuming intraoperative moving of the robot and redocking from the opposite side of the patient. Nevertheless, the mean operative time of 321.7 minutes is higher than that of the laparoscopic CME series, ranging from 119 to 274 minutes.10,12–14
We note that this study has several limitations due to its noncomparative nature and retrospective design despite the use of prospectively collected data. Our interpretation of the results was also limited by the short follow-up period.
Based on our initial experience, robotic surgery for CME of transverse colon cancer is feasible, safe, and can be a procedure of choice to achieve a good oncologic quality of the resected specimens. Well-designed comparative studies are required to further explore the role of robotic surgery in this procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.