
Abstract
Abstract
Background:
Pectus excavatum is a common chest wall anomaly. Achieving optimal pain control is a priority for adolescents undergoing surgical correction of this condition. Options for pain control include the use of subcutaneous catheters (On-Q® pumps) and epidurals. The objective of this study is to demonstrate the feasibility of using subcutaneous catheters for pain control and to compare them with the use of epidurals during surgical correction of pectus excavatum.
Materials and Methods:
We identified patients who underwent pectus excavatum repair at our institution between January 2010 and August 2016. Patients were divided into two cohorts (epidural or On-Q pump). Patient charts were reviewed for length of stay, pain scores, pain medications, and complications.
Results:
A total of 124 patients were included. Forty percent of patients used an epidural (n = 50), and 60% had the On-Q pump (n = 74). The average patient age was 15.6 years. The average Haller index was 4.3. The On-Q pump population had a significant decrease in postoperative length of stay (mean [M] = 4.86, standard deviation [SD] = 0.85) compared with the epidural population (M = 5.60, SD = 0.97); P ≤ .001. There was a significant difference observed in pain scores for patients on the epidural (M = 2.91, SD = 1.13) and On-Q pump (M = 3.81, SD = 1.19; P ≤ .001). There was n = 1 wound infection in each group.
Conclusion:
The use of bilateral subcutaneous infusion catheters is a safe and effective method for pain control in patients undergoing surgical correction of pectus excavatum. Even though the degree of pain control is not necessarily superior to epidurals, in this study, the catheters were associated with a shorter postoperative length of stay in this patient population and did not increase the incidence of complications.
Introduction
P
Patient-controlled analgesia (PCA) has been one alternate method of pain control in patients who undergo chest wall reconstruction. In 2008, St. Peter et al. 8 published their retrospective review of patients who underwent pectus repair at their institution. They compared the outcomes of patients who used epidurals versus those who used PCAs. They found that patients with PCA had significantly shorter OR times. The length of hospital stay was not significantly different. 8 However, in 2012, there was a follow-up prospective randomized trial comparing epidurals to PCAs. The advantage of PCA over the epidural included fewer calls to anesthesiologists and fewer hours to Foley removal. The length of stay was similar between the two groups—just over 4 days. 9 Another randomized trial performed by Butkovic et al. 10 in 2007 showed similar pain scores, vital signs, and hemodynamic indicators in patients who used PCAs compared with those who used epidurals.
Tunneled, anesthetic-infiltrating subcutaneous catheters are another modality of pain control that has been investigated for pectus excavatum repair. The most well-known subcutaneous catheter is the On-Q pump® (Halyard Health, Alpharetta, GA). In 2013, Pontarelli et al. 12 published a study comparing the use of On-Q® pain pumps to epidurals in children who underwent midline abdominal procedures, transverse abdominal procedures, Pfannenstiel incisions, thoracostomies, and bone and soft tissue procedures. They found that children who used the On-Q® pumps had effective pain control and a similar pain profile compared with children who used epidurals.11,12 More recently, adult studies have demonstrated the effectiveness of subcutaneous pain catheters in patients who undergo the Nuss procedure or minimally invasive repair of pectus excavatum (MIRPE). One randomized trial comparing subcutaneous catheters to epidurals revealed that the two groups had no significant difference in daily pain scores, morphine-equivalent opioid usage, or hospital stay. 13 Retrospective reviews have been performed in the pediatric population with similar findings.14,15
In the last 5 years, our center has started to use bilateral subcutaneous infusion catheters (On-Q® pump) to help assist in pain management for our pectus excavatum patients. The catheters have been used as an adjunct to PCAs. Before our adoption of these catheters, epidurals with PCAs were routinely placed to manage pain in this population. The purpose of this study is to demonstrate the feasibility of using On-Q® pumps for adolescent patients undergoing repair of pectus excavatum. Furthermore, we compare the experience of patients who used the On-Q® pumps with those who used epidurals in terms of length of stay, pain scores, and complications.
Materials and Methods
Institutional Review Board approval was obtained to conduct a retrospective chart review on patients who had undergone MIRPE or modified Nuss procedure. The time of review spanned from January 2010 to August 2016. Patients were divided into two cohorts based on the pain control treatment they were administered—epidural and On-Q. Data were obtained from electronic medical records and paper charts. Primary outcomes were length of stay, pain scores, and complications.
Thoracic epidurals were used from 2010 to 2012 (n = 50). Subcutaneous catheters were used from 2012 to 2016 (n = 74). All patients in both groups received the same adjunct medications. The same induction medications were used for both patient populations. These included propofol infusion 2–5 mg/kg, fentanyl injection 1–3 mcg/kg, and rocuronium 0.6–1 mg/kg. The patients then followed a pain protocol that is described in detail in Table 1. For the hydromorphone PCA, patients were started at a concentration of 0.2 mg/mL with 6-minute lockouts. The loading dose given was 0.01–0.02 mg/kg (up to 1 mg). The PCA dose itself was 0.004 mg/kg (up to 0.2 mg). One hour maximum was 0.01–0.02 mg/kg (up to 1 mg).
PCA, patient-controlled analgesia.
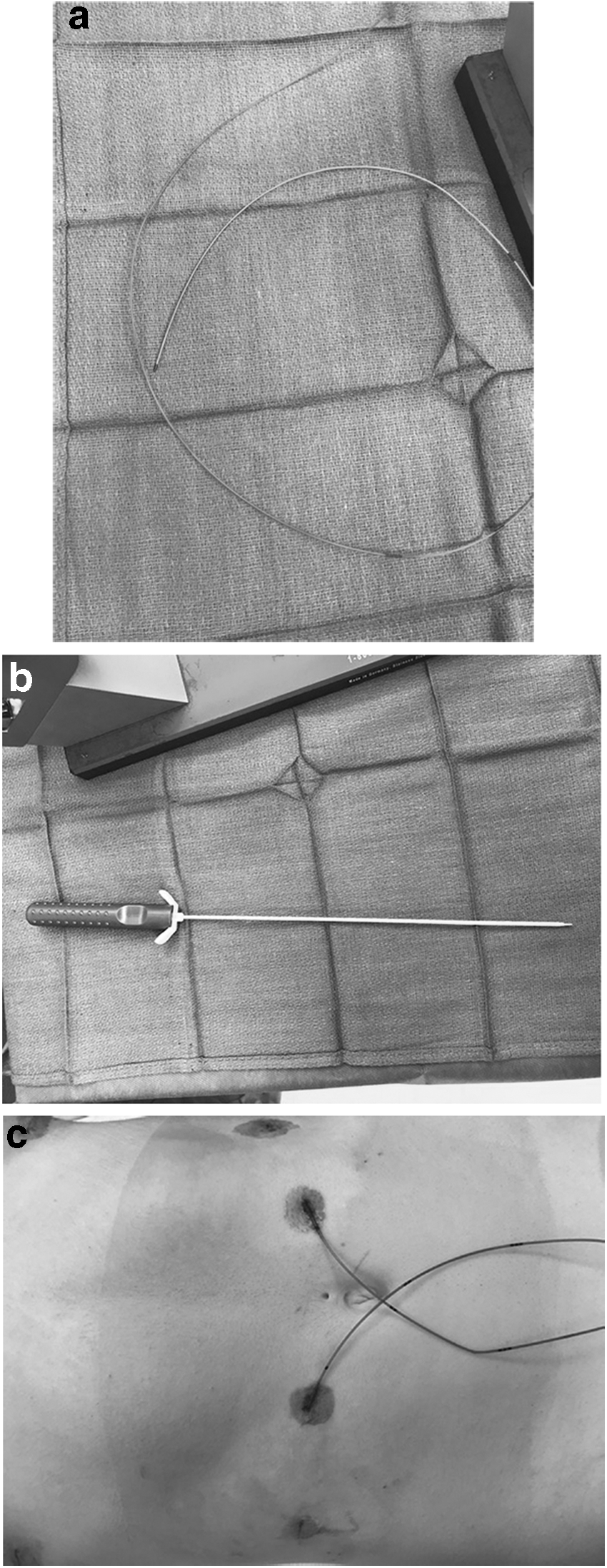
The On-Q group was administered ropivacaine 0.2% continuously. The maximum infusion rate per hour was 0.4 mg/kg/hour. The medication infused through the epidurals was bupivacaine 0.1%. A picture of On-Q pump placement is in Figures 1 and 2a–c. The On-Q pumps were multiholed 7.5-inch or 10-inch wound catheters inserted bilaterally by the pediatric surgeons at the beginning of the case. The catheters were placed subcutaneously with assistance of tunnelers. The tip of the catheter was superior to the main chest incisions used for the Nuss procedure. Patients had epidurals placed at T5–T6/T6–T7 level. All epidurals were placed by the anesthesiology team while the patient was asleep. The epidurals were placed in midline. The test dose was 1.5% lidocaine with epinephrine (1:200,000). The epidurals typically stayed in place until the patient could start oral pain medications—this ranged from postoperative day 2 to postoperative day 4. All patients underwent the Nuss procedure. All patients received perioperative IV cefazolin. General endotracheal intubation was performed for the case. All patients in this series received only 1 bar for correction of their pectus. The bar was secured to the chest wall with either a stabilizer/foot plate on the left side of the chest and FiberWire, or with 19-gauge sternal wires that were tied around two different ribs on the right side of the chest. The patients typically remained on bed rest on postoperative day 0, and they would ambulate on postoperative day 1. Discharge criteria included patient's being able to ambulate without assistance, tolerate medications by mouth and food intake without antiemetics, and have pain well-controlled with oral medications only.

The On-Q® pump catheter and tunneler laid on top of the patient during a Nuss procedure.
Analyses were performed using SPSS 16.0 (IBM Corporation, Armonk, NY). The relationship between variables was evaluated using Fisher's exact test or independent sample t-tests. All tests were two tailed, with a P-value of .05 or less considered significant.
Results
Study population
Charts of 124 patients who underwent the Nuss procedure for the correction of pectus excavatum between January 2010 and August 2016 were reviewed for this study; all were included in the analysis. The majority of subjects were male (86%), non-Hispanic (84%), and Caucasian (82%). Average age at time of Nuss procedure was 15.6 years (standard deviation [SD] = 2.2; Table 2).
Data are presented as (n) with percentages or (n) with SD.
Pearson's chi-square.
Fisher's exact.
SD, standard deviation.
The length of stay was significantly shorter in the On-Q pump group (mean [M] = 4.89, SD = 0.854) compared with the epidural group (M = 5.60, SD = 1.0; P ≤ .001). However, the average pain scores during the hospital stay were better in the epidural cohort (M = 2.91, SD = 1.13) compared with the On-Q pump cohort (M = 3.81, SD = 1.19; P ≤ .001). A total of 65 patients received a preoperative consult with the hospital's pain specialists. Of these 65 patients, 13 (26%) were in the epidural cohort and 52 (70%) were in the On-Q pump cohort. The frequency of patients who received a postoperative consult from the inpatient pain management team was greater in the On-Q pump cohort (83%) versus the epidural cohort (53%). A significant correlation was not identified when comparing the frequency of pain consultations with average pain score.
Medication use
All 124 patients of this study were administered postoperative narcotics. Ninety-three percentage (n = 115) of patients received adjunct acetaminophen, and 90% (n = 111) of patients received adjunct anti-inflammatory medications. A total of 119 (96%) patients were prescribed narcotics on discharge. The different discharge narcotic regimens are found in Table 3. There was no significant difference in discharge narcotic use in patients who received epidural versus On-Q pumps. Methocarbamol was also prescribed to 62% (n = 77) of patients on discharge. Of these, n = 36 were in the epidural group and n = 41 were in the On-Q pump cohort. There was no significance in methocarbamol administration between the two cohorts.
Data are presented as (n) with percentages.
Fisher's exact.
The average time for patients to stop all medication postoperative was 18.05 days (SD = 10.20). Postoperative narcotic use for study patients averaged 13.6 days (SD = 7.8). No significance was observed for time to stop postoperative narcotics between the Epidural and On-Q pump cohorts.
Daily pain medication intake was documented for the duration of the patient's stay. Pain medications administered included: anti-inflammatory medications, acetaminophen, and narcotics. The daily pain medications administered for both cohorts are found in Figures 3–7.
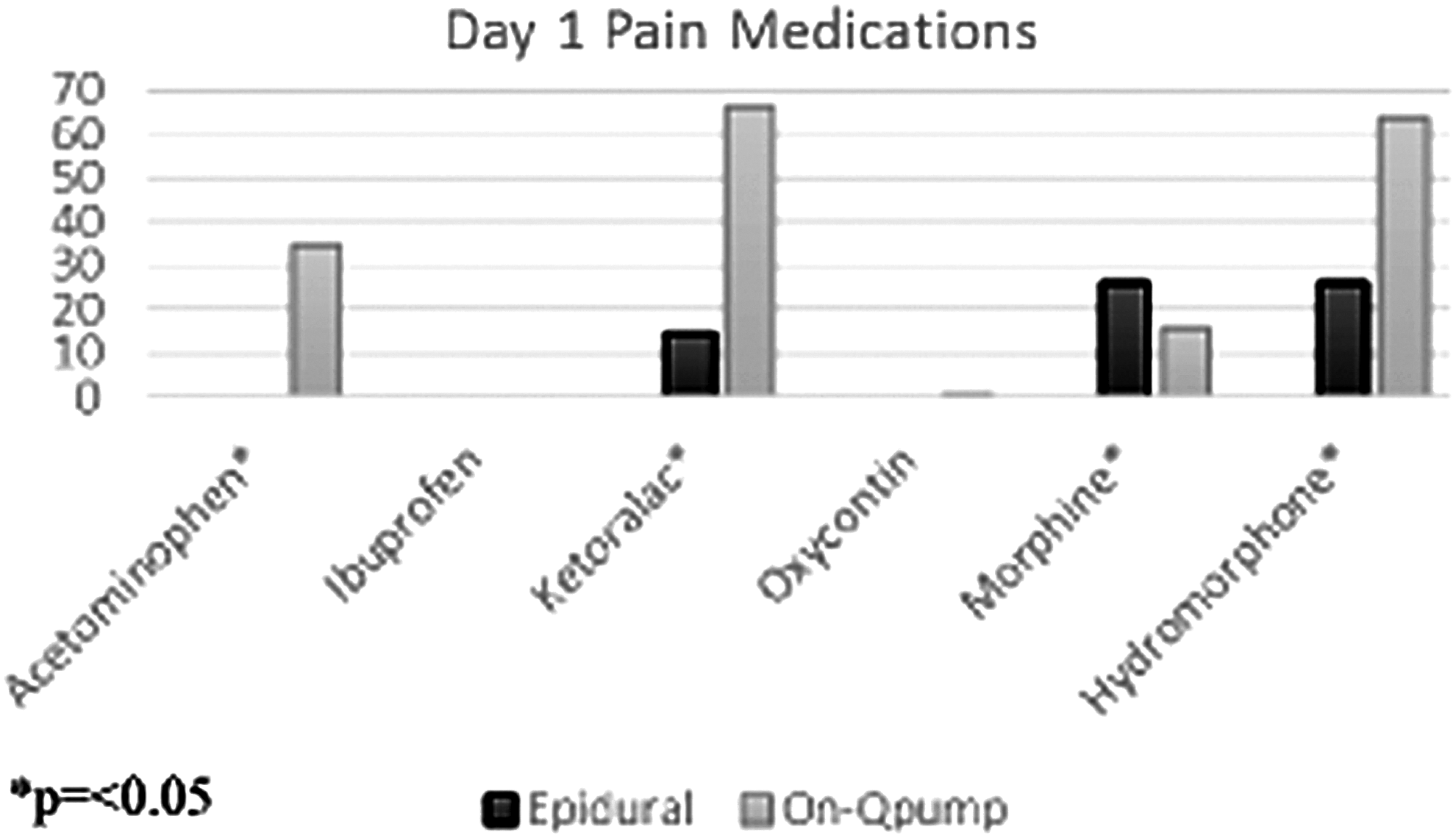
Medication administration for both cohorts day 1.
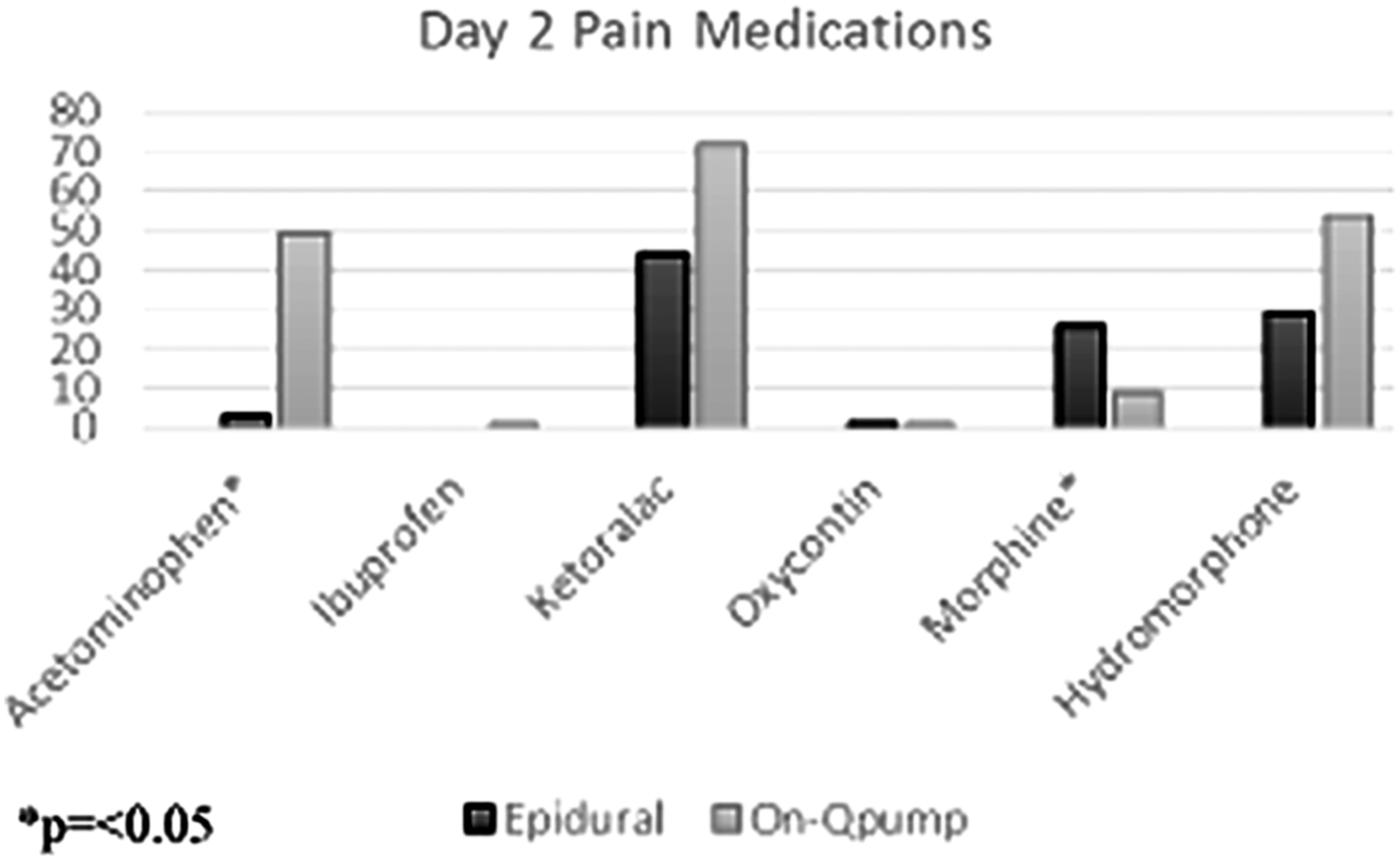
Medication administration for both cohorts day 2.
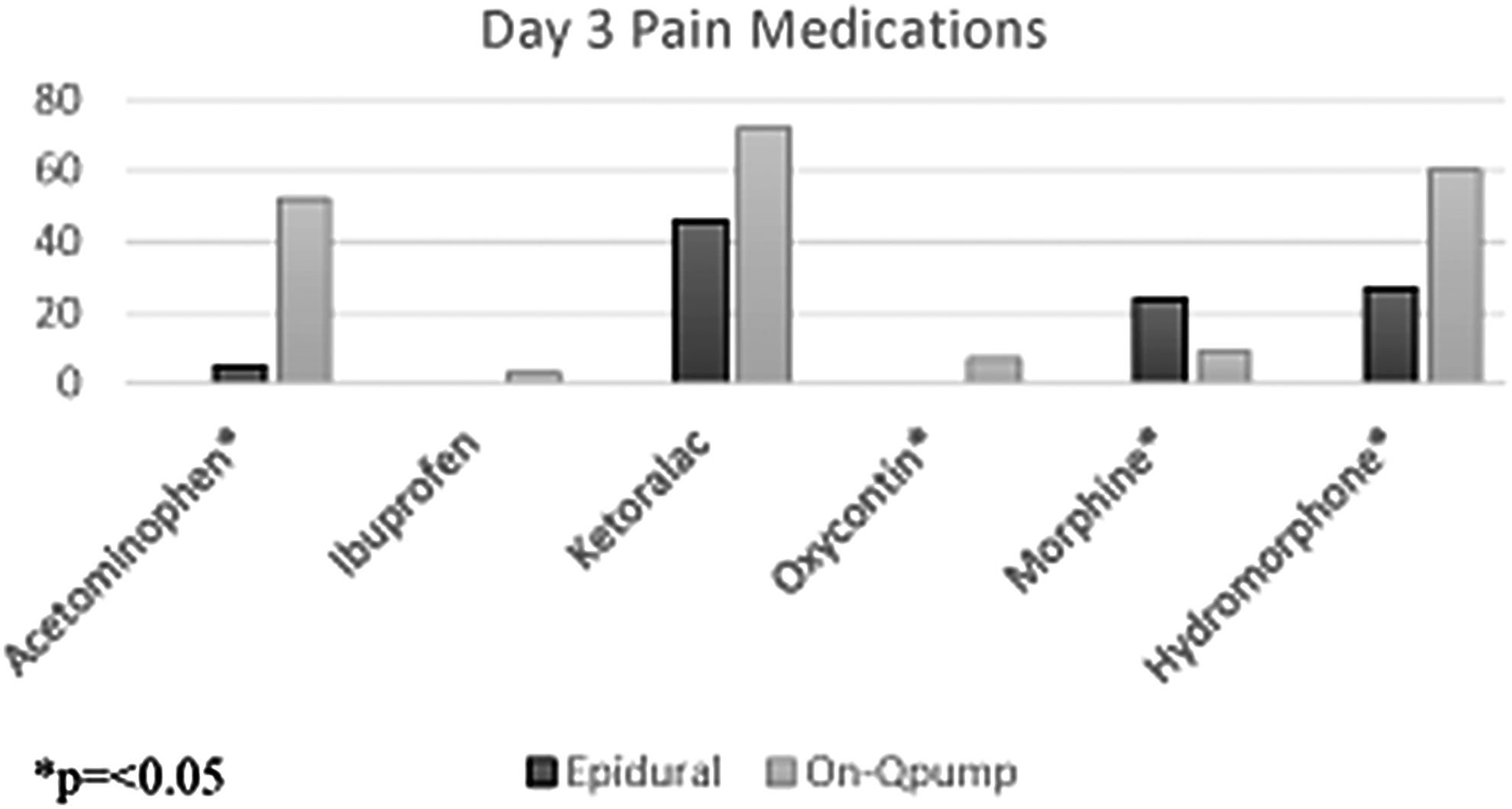
Medication administration for both cohorts day 3.
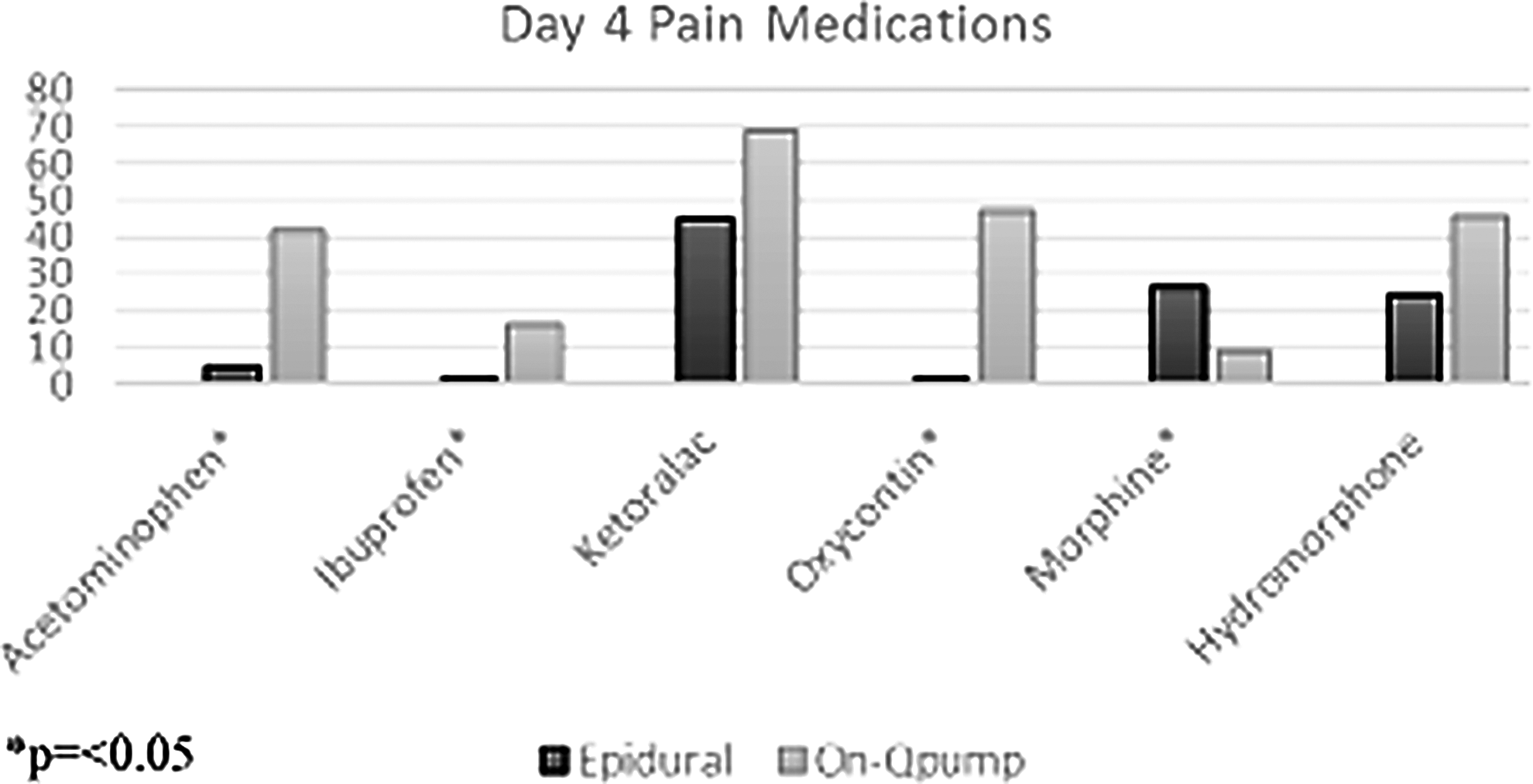
Medication administration for both cohorts day 4.
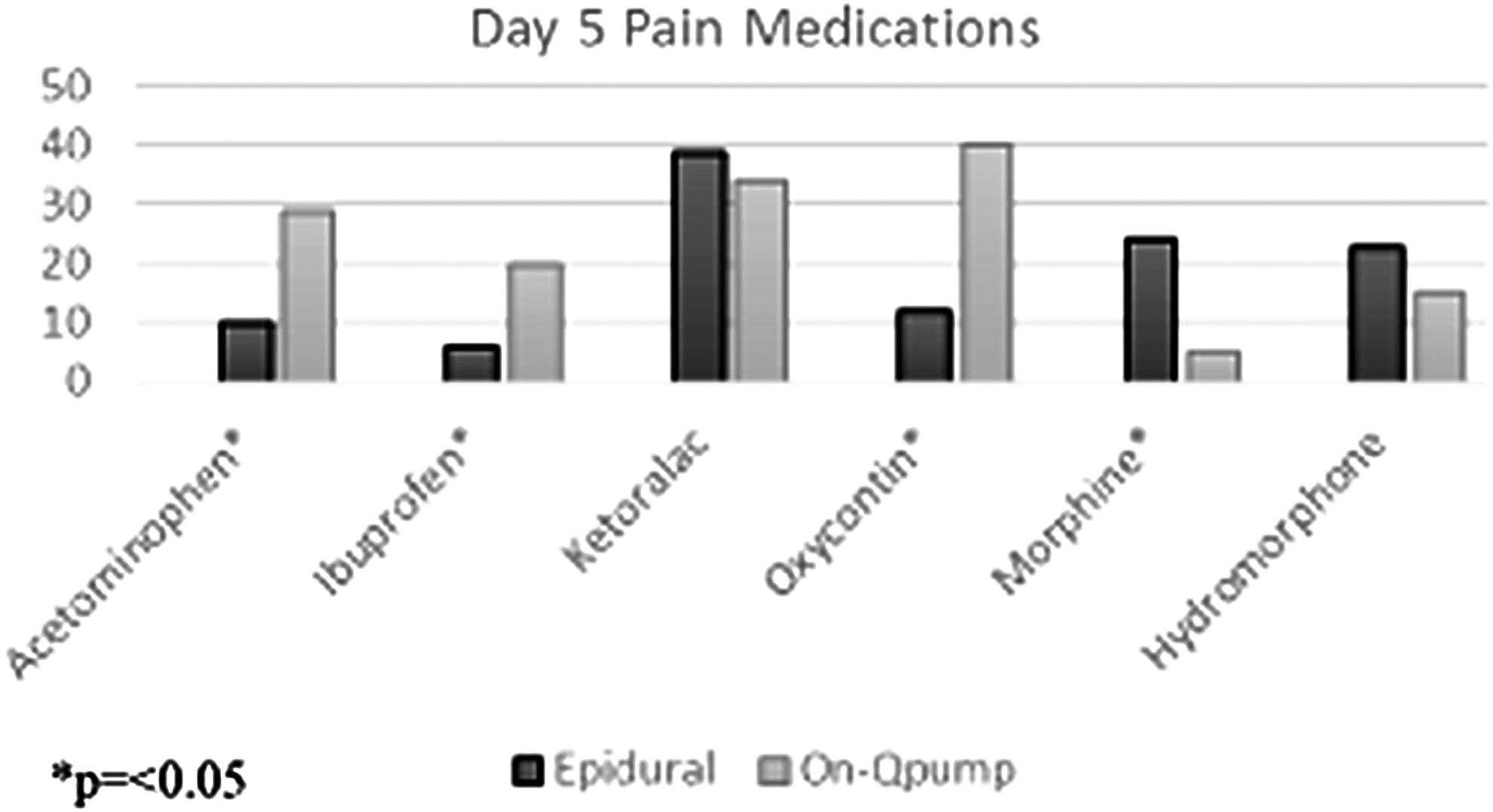
Medication administration for both cohorts day 5.
Comorbidities
The overall incidence of comorbidities in the study cohort was 32.3% (n = 40). A total of 11.3% (n = 14) had asthma, 9% (n = 11) had scoliosis, and 1 had a diagnosis of Marfan's syndrome. Other comorbidities included Asperger's, anxiety and congenital heart defects.
Complications
Two surgical-site infections were documented in groups, one in the epidural cohort and one in the On-Q pump cohort. This was not a statistically significant difference.
Discussion
The use of bilateral subcutaneous infusion catheters is a safe and effective method for pain control in patients undergoing surgical correction of pectus excavatum. These catheters can function similarly to epidurals in this patient population. In this study, the catheters were associated with a shorter postoperative length of stay and did not increase the incidence of infection and other complications. However, the degree of pain control, as measured by pain score during hospitalization, was still better in the epidural population.
We perform 35–40 Nuss procedures a year at our center. We have been using On-Q® pumps over epidural catheters exclusively since 2013. As described in Table 1, we have developed a postoperative pain protocol that all pectus excavatum patients undergo. Even though there was no statistically significant difference in time to wean off narcotic use in our On-Q population compared with our epidural population, in the last 2 years in particular, it seems that most patients are weaning off narcotics faster than the 2 weeks average indicated in the Results section. Patients undergo the Nuss procedure follow-up in clinic at 1, 2, and 4 weeks postoperative, in addition to more long-term postoperative visits. In the last 2 years, the majority of patients indicate to us that they have stopped all narcotic use by 1 week postoperative. This pattern may be following a national trend to try and minimize opioid use. However, it also may have to do with the fact that most patients go home on the On-Q® pump for 2 to 3 days before their pumps run out.
One additional variable that we also planned to compare while conducting this study was the operating room times between the epidural group and the On-Q group. In 2013, the medical center underwent a transition from paper to electronic medical records, and due to this changeover, some of the data from the epidural group, who underwent surgeries before 2013, were limited. In our medical centers, epidurals are placed in the operating room and therefore are factored into the operating room time. We have timed the duration of time for our On-Q® pump placements, and it ranges from 5 to 10 minutes. The epidural placements for recent other thoracic cases (nonpectus cases) range from 5 to 20 minutes. Therefore, although we cannot demonstrate the potential decrease in total OR time, another advantage to On-Q pumps may be time saved in the OR.
There are several limitations present in this study. One limitation is that it is a retrospectively conducted study. More reliable data would be obtained from a prospective randomized trial. However, that study is unlikely to be performed at our center as the surgeons have universally adopted On-Q® pump placement for the Nuss procedures instead of epidurals. The main reasons behind this include an avoidance of neurologic sequelae with the On-Q® pump and the subjective patient satisfaction with the pumps.
In addition, the institution transitioned from paper charts to electronic health records between 2012 and 2013, and this limited our ability to abstract variables that would have provided more data supporting the advantage of On-Q® pumps. The study also recognizes that patient pain scores are a subjective measurement. Although all patients indicated their pain levels using the FACES pain scale, there is likely variance in interpretation of the FACES scale from patient to patient. Documentation in charts, primarily at postoperative follow-up visits, was also a limitation of this study. Four surgeons in our group performed the Nuss procedure, and documentation of patient's pain medication use at postoperative visits varied from provider to provider.
We can attribute the shorter length of stay in the On-Q group to several reasons. The first notable reason is we have changed the patient expectations with respect to discharge criteria, and the probability of going home pain free. We have altered our discharge criteria to recognize that although pain will be present, this can be managed by the On-Q® pump and pain medications provided at discharge. As a group, we have implemented this change and this has resulted in a decrease in the length of stay. In addition, the comfort level of the surgeons performing the Nuss procedure using the On-Q® pump, the primary pain management technique, has increased, and as a group are more agreeable to send a patient home earlier, with the proper pain management schedule. The other major factor of the shorter length of stay in the On-Q® group is the historical cohort. The time period of this study spanned 7 years. The length of stay for most surgical conditions would be expected to decrease over this time period, as surgeons gain comfort with an operation. It is not possible to quantify what percent of the decreased length of stay was due to the infusion catheters alone compared with other factors that would cause a reduction in length of stay over time (surgeon comfort, patient expectations, insurance companies regulating length of stay, etc.).
The study suggests that subcutaneous pain catheters are an effective method of pain relief when combined with opiates, nonsteroidal inflammatory medications, and other nonopiate medications during the surgical correction of chest wall deformities. We foresee the continuation of this practice at our medical center over the next several years.
Footnotes
Disclosure Statement
No competing financial interests exist.