
Abstract
Abstract
Background:
Our objective was to investigate the clinical characteristics of laparoscopic repair for groin hernias in female patients.
Study Design:
The clinical data of 316 female patients (341 hernias) who underwent laparoscopic inguinal hernia repair at Shanghai Minimally Invasive Surgery Center between January 2001 and December 2015 was analyzed retrospectively. The operation-related data were to provide an overview of female groin hernias, preferred surgical approach, and the management of round ligament of uterus.
Results:
There were 274 transabdominal preperitoneal patch plastic repairs and 67 total extraperitoneal repairs performed on 257 and 59 patients, respectively. The median follow-up period was 48 months. Fifty-eight femoral hernias were noted in 52 patients, of which 18 femoral hernias were incarcerated. Cysts on the round ligament of uterus were found in 39 patients, and most of them underwent laparoscopic resection. Round ligaments of uterus were preserved in 152 patients and transected in 162 patients. The preservation group requires longer operation time and trickier surgical technique. None of the cases was converted to laparotomy. All patients returned to normal activity soon and no recurrence was noted during follow-up.
Conclusions:
Laparoscopic inguinal hernia repair is well adopted around the world. Meanwhile, there still remain questions to be discussed in female patients. Based on this study, the round ligament cyst could be resected while the operation. Either “open and suture” or keyhole technique will be available to preserve the round ligament of uterus.
Introduction
R
The prospective data registered of treatment and outcome of female patients with groin hernias performed in Minimally Invasive Surgery Center (MISC) of Shanghai Ruijin Hospital enables the description and further study into this comparatively rare topic. 1 A total of 341 hernias were operated on in 316 females from January 2001 to December 2015. The aim of this study is to discuss the characteristics of female groin hernias, the technique of operation preferred, and especially the management of round ligament of uterus in the procedure.
Methods
Patients
Four thousand four hundred forty-five cases (5330 hernias) of laparoscopic inguinal hernia repair were performed in Shanghai MISC of Ruijin Hospital from January 2001 to December 2015, among which 316 patients were female (7.1%) with 341 hernias (6.4%). Average age of female patients was 53.3 ± 18.2 (16–89) years of age and body mass index was 21.3 ± 3.0 kg/m 2 . There were 177 right-sided hernias (56.0%), 114 left-sided hernias (36.1%), and 25 bilateral hernias (7.9%) out of all the female patients. Among them, there were 241 indirect hernias (70.7%), 18 direct hernias (5.3%), 58 femoral hernias (17.0%), 16 recurrent hernias (4.7%), and 8 combined hernias (2.3%). According to the classification criteria of Chinese Hernia Association, 8 19 hernias (5.6%) were classified into Type I, 244 (71.6%) were Type II, 62 (18.2%) were Type III, and 16 (4.7%) were Type IV. All the patients were followed every 3 months, and median time of follow-up was 48 months (4–60 months).
Operation methods
TAPP was performed on 257 patients (274 hernias) and 59 patients (67 hernias) underwent TEP. All the procedures were performed by the same surgical team after evaluation. TAPP and TEP were performed with the technique reported by Dion and Morin 9 and McKernan and Laws, 10 respectively. The round ligament of uterus was either transected or preserved based on the anatomical characteristic of patients. Two major techniques were implemented to preserve the round ligament: open and suture of peritoneum, and keyhole technique. The meshes were selected from one of the following: 10 × 15 cm Prolene (Ethicon), Vipro II (Ethicon), ULTRAPRO (Ethicon), or 3DMax (Bard).
Statistical method
Statistical analysis was carried out using SPSS version 18.0 for Windows (SPSS, Inc.). Measurement data were presented as mean ± standard deviation and analyzed by t-test and variance analysis. Enumeration data were calculated by χ2 test. A P-value <.05 was considered statistically significant.
Results
Femoral hernia
In the study, 58 femoral hernias were found in 52 patients (17%, 58/341), of which 18 incarcerations with greater omentum in 4 cases, preperitoneal fat in 11 cases and 3 patients had both. All the incarcerated femoral hernias were dealt with by TAPP.
Cyst on the round ligament of uterus
Cysts on the round ligament of uterus were found in 39 patients (12.3%, 39/316) (Fig. 1). Laparoscopic resection was performed in 38 cases, which includes 35 TAPPs (90.3%) and 4 TEPs (9.7%). The remaining one was removed with a small incision in the inguinal area.
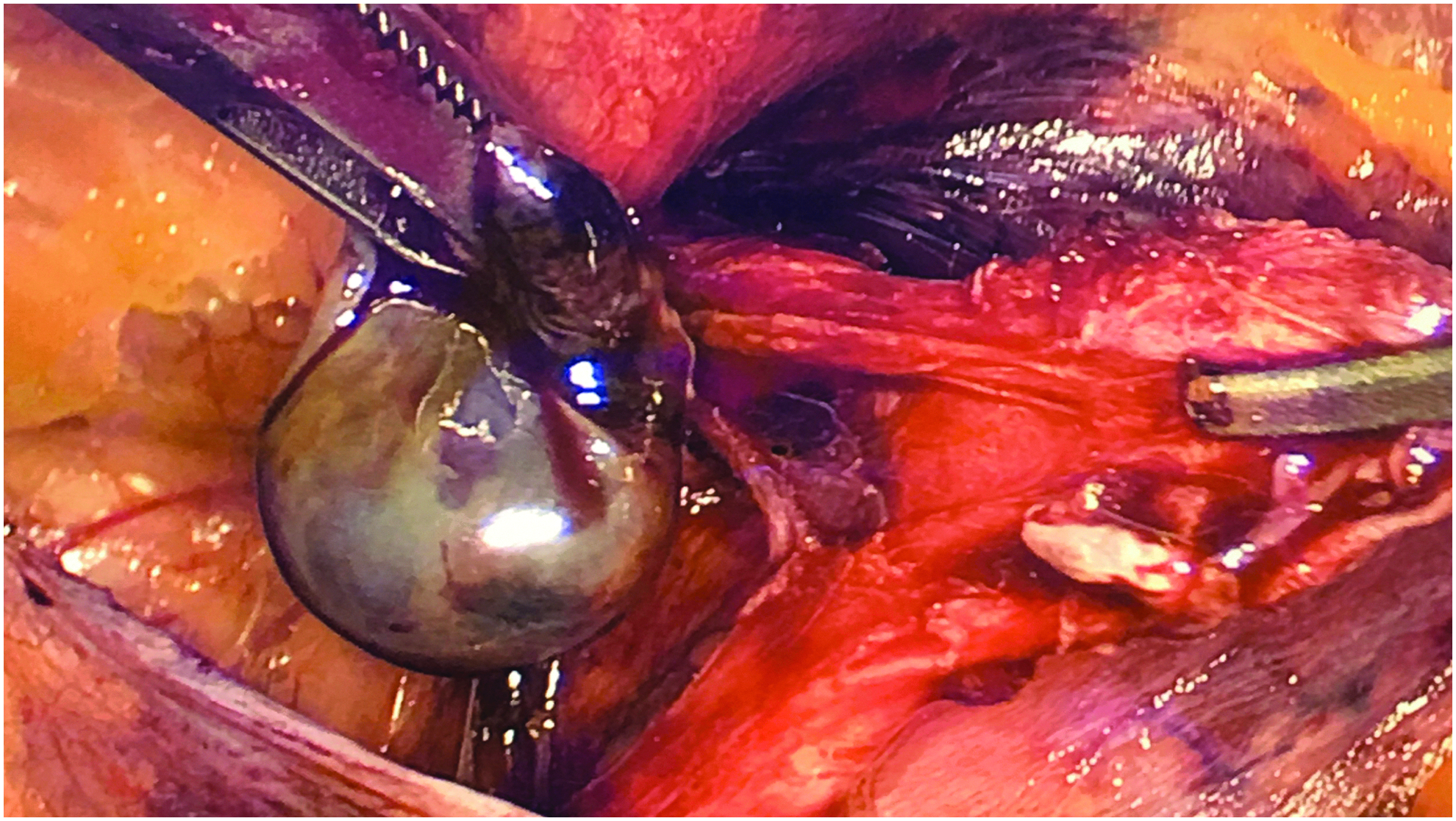
Round ligament cyst.
Round ligament of uterus
One hundred sixty-two round ligaments of uterus were preserved in 152 patients, whereas the other 179 ligaments in 164 patients were transected. In the preservation group, 28 round ligaments of uterus were completely peritalized without any damage on the peritoneum. In the 14 cases, the round ligaments of uterus were dissected with open and suture of the peritoneum and meshes were placed in front of the ligaments. For the remaining 120 cases, the meshes were placed behind the ligaments by using the Keyhole technique. There were 146 TAPP (90.1%) and 16 TEP (9.9%) performed in the preservation group, and 128 TAPP (71.5%) and 51 TEP (28.5%) in the transection group (P < .01). The average age in the 2 groups were 43.2 ± 16.2 and 62.6 ± 13.9 years of age (P < .01), respectively. Operation time in the preservation group (30.6 ± 11.1 minutes) was significantly longer than that in the transection group (24.9 ± 8.2 minutes) (P < .01) (Table 1).
TAPP, transabdominal preperitoneal patch plastic repair; TEP, total extraperitoneal repair.
Operation-related data
None of the cases was converted to laparotomy. The average postoperative hospitalization was 1.5 ± 0.2 days. There were 14 cases of seroma (4.5%) and 3 cases of urinary retention (1.0%) observed. All patients returned to normal activity within 2 weeks. No recurrence was noted in the follow-up.
Discussion
Female patients have a higher incidence of femoral hernia, so preperitoneal approach is widely adopted. According to European Association for Endoscopic Surgery (EAES), laparoscopic repair should be considered to treat femoral hernia in female patients. 5 Femoral hernia is more likely to be incarcerated, as result, it is recommended to perform surgery in a short time.11,12 Incarcerated hernial contents are different between female and male patients. In male patients, intra-abdominal organs or tissues (intestine, omentum, etc.) are mostly found, whereas in female patients, incarceration of preperitoneal lipoma also shares a high incidence rate (Fig. 2). Incarcerated lipoma will be easily dealt with by mobilizing the iliopubic tract under laparoscopy. TAPP is preferred in female patients as it gives a clear overlook on the incarcerated hernial contents.
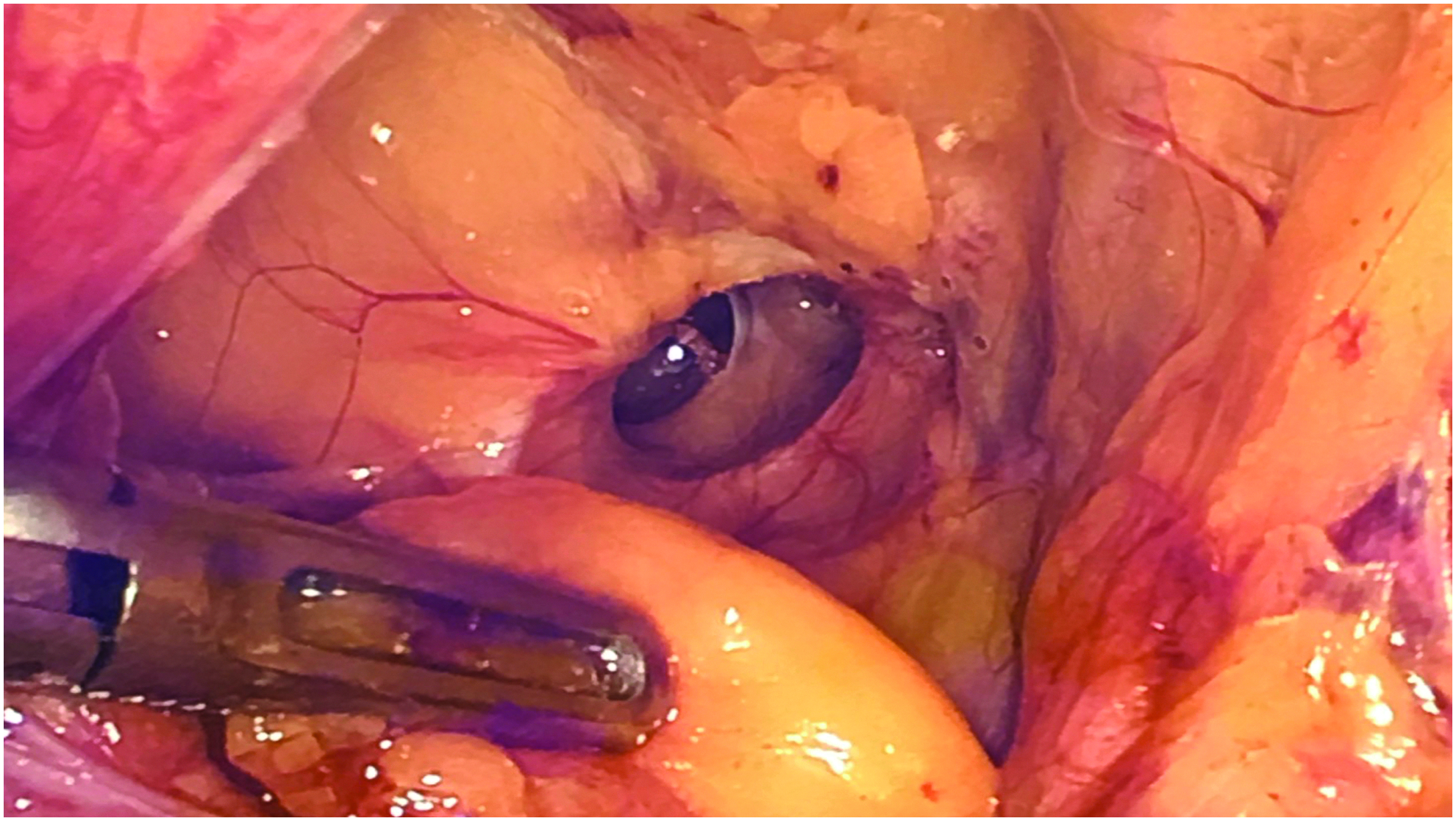
Incarceration of preperitoneal lipoma.
Laparoscopic repair is recommended for the female patients with round ligament cysts as it provides a precise diagnosis and possibility to remove the cyst during the hernioplasty. For the immobile round ligament cysts under laparoscopy, a mini laparotomy at the inguinal area is recommended. It is easy to detect a cyst proximal to the round ligament, while for distal ones, maneuvers like traction of round ligament, careful palpation, or both should be carried out in case of misdiagnosis. In some cases, round ligament cysts are misdiagnosed as inguinal hernia. To prevent the vulnerability of internal ring and posterior wall of inguinal canal caused by the dissection of the cysts under laparoscopy, a prophylactic repair is considered feasible. So TAPP is recommended as a better exploration method for the female patients suspecting preoperatively for round ligament cyst.
The contents of round ligament in female patients are different from those of the spermatic cord in male patients, as the round ligament is considered as interperitoneal, whereas extraperitoneal for the spermatic cord. As result, it is extremely difficult to achieve a complete peritalization for female patients (especially in a preperitoneal approach). Sun has classified the relationship between round ligament and peritoneum into 3 groups: loose, small-gap, and no-gap. 13 In this study, only 8.5% of cases (29/341) fit in the loose group and round ligaments are easily preserved. For the remaining patients, round ligaments are closely attached to the peritoneum. It is difficult to preserve them, and also requires special approaches.
The feasibility to transect the round ligament of uterus is controversial. As it originates at the uterine horns in the parametrium, the round ligament leaves the pelvis through the deep inguinal ring passing through the inguinal canal and continues on to the labia majora to maintain the anteflexion of the uterus during pregnancy, to prevent prolapsus of uterus and potential blood supply possibility during pregnancy.14,15 It is uncommon to transect the round ligament during conventional hernioplasty in female patients. However, female patients normally have a higher postoperational recurrence rate than male patients. Especially when performing a preperitoneal repair, including the laparoscopic repair without transecting the round ligament, will make placement of meshes trickier, prolong the operation time, and increase the recurrence rate.16–18 In this study, although transecting the round ligament was shown to shorten the operation time by 6 minutes in average, further stratified analysis will be needed to eliminate other underlying factors. It is optimal to transect the round ligament with a complete preperitoneal mesh placement, especially for the purpose to reduce surgical and anesthetic risk for the elder patients with no fertility requirement or with increased intra-abdominal pressure and large hernia defect area. The round ligament of uterus is recommended to be preserved in the younger female patients with fertility requirement.19,20
There are two major approaches recommended to preserve the round ligament of uterus:
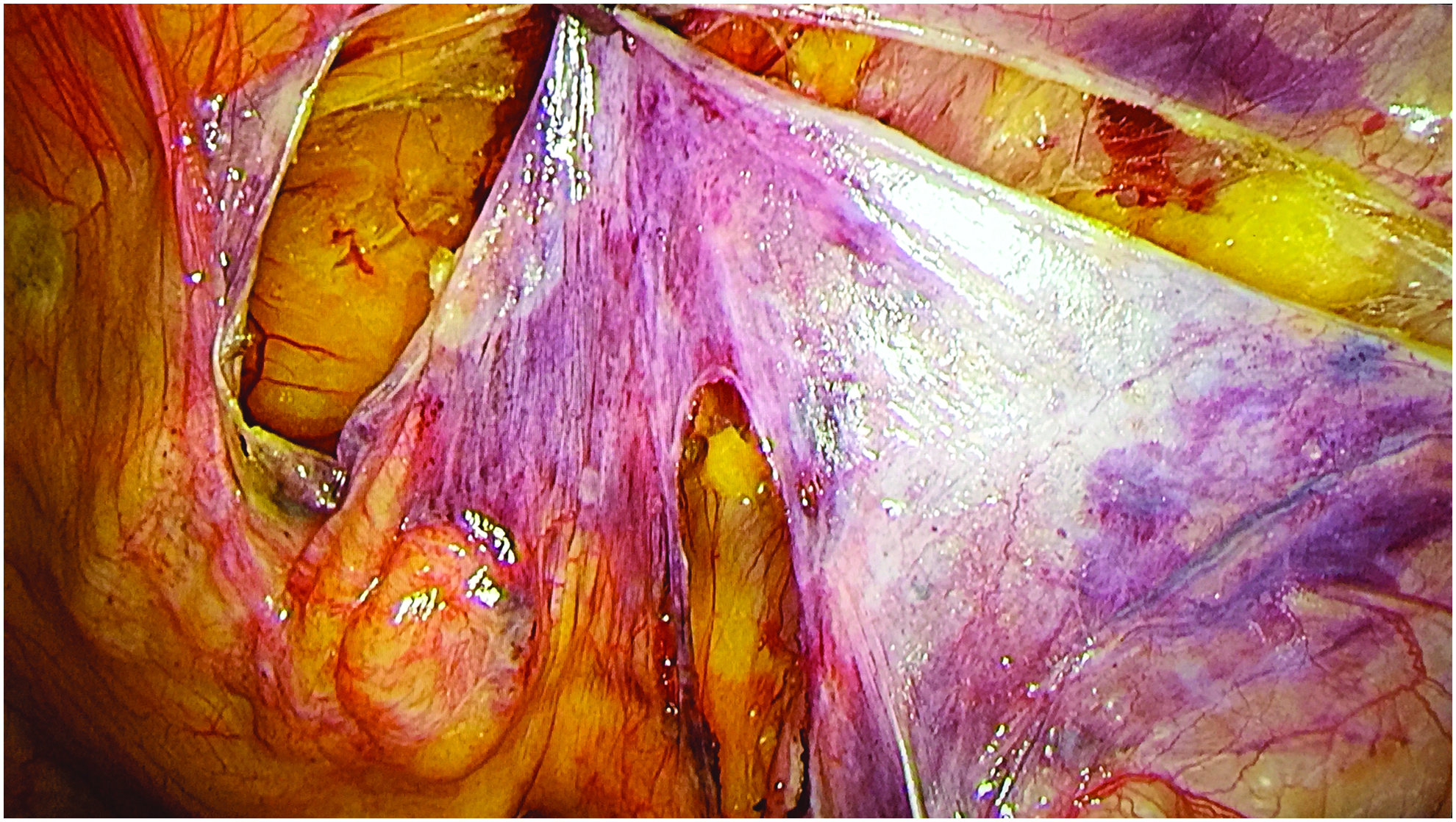
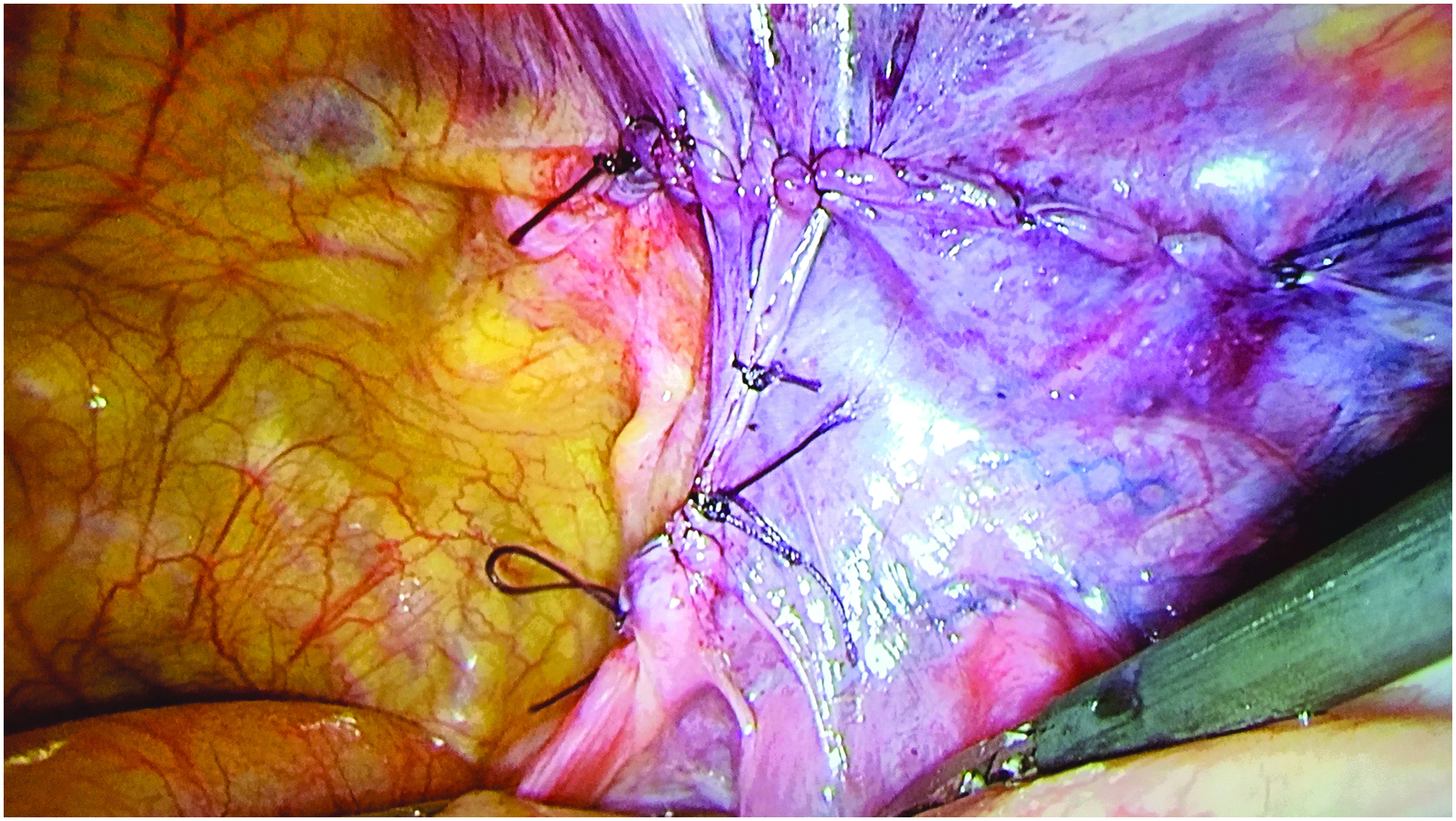
Open and suture of peritoneum: Figures 3–6 show the procedure of this technique. To simulate a complete peritalization, peritoneum is opened bilaterally along the round ligament to the level of 6 cm under the internal ring. Place a flat mesh anterior to the round ligament before closing the peritoneum by suture. This method was carried out in five early cases in our study. In fact, the tight attachment between the round ligament and peritoneum was not aware of then. Inappropriate peritalization of the round ligament of uterus will lead to tearing and defect of peritoneum, which requires repair by suture after the placement of mesh. Lately, some surgeons are preserving the round ligament of uterus by using the technique of open and suture of peritoneum, which comes up with good results. In terms of the surgical approach, TAPP is considered easier as it provides more spatial surgical area without any concern of the “air leak.” However, if the surgeon is well trained, TEP has the same outcome as TAPP.
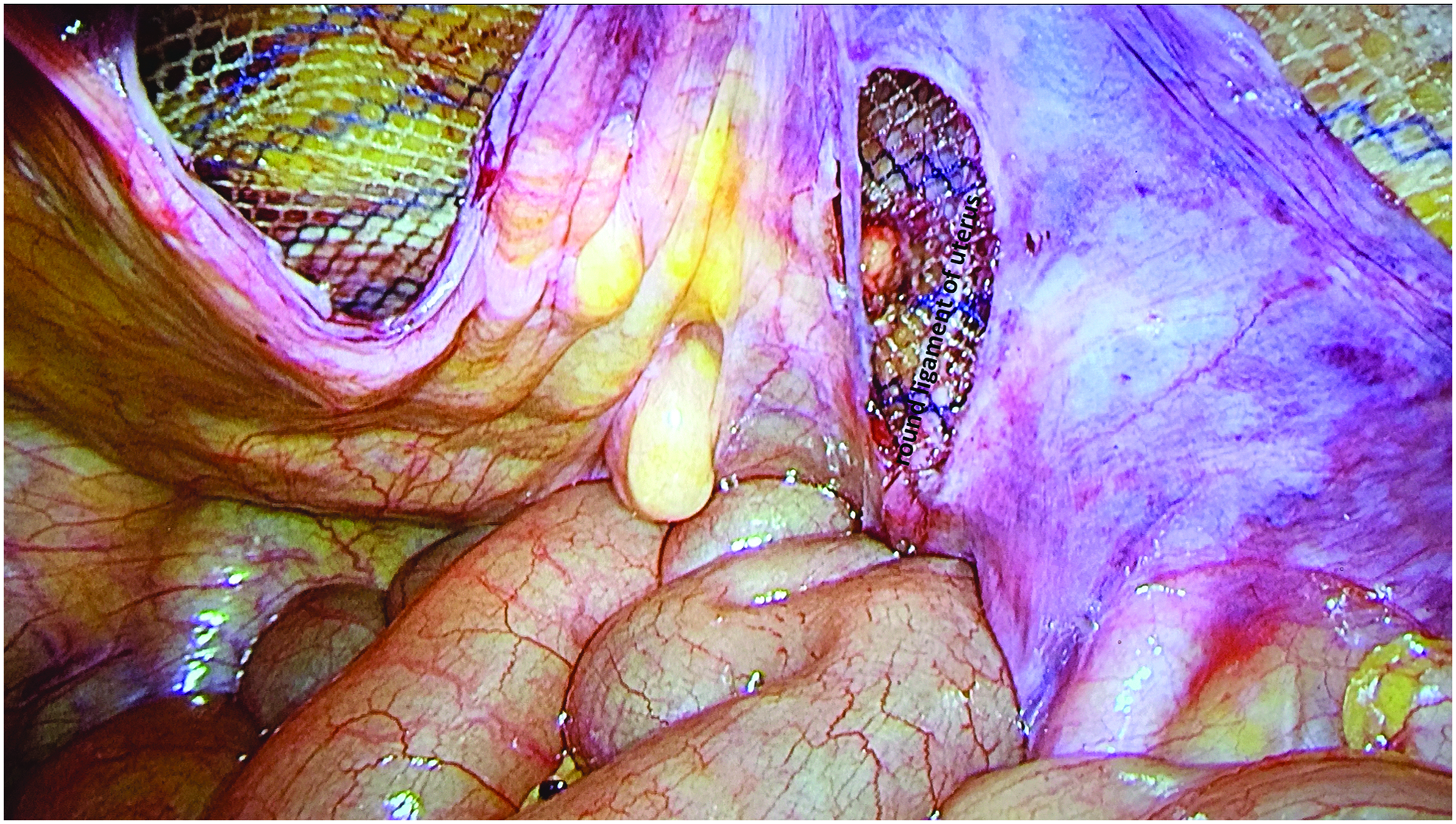
Peritoneum is opened horizontally first, then vertically along the two sides of the round ligament. Anatomy of peritalization of the round ligament. Preperitoneal placement of mesh. Sutures of the peritoneum. Keyhole technique: Figures 7–10 indicate how to carry out this procedure. Make a breach on the mesh, wrap it around the round ligament and place it behind (different from the way in male patients). Close the breach by using fibrin glue or suture. The procedure simulates the mesh placement behind transversalis fascia by reconstructing the transversalis fascia and internal ring.
7
There were 125 cases in the study performed this way as our major method to preserve the round ligament. This approach is easier and simpler as peritalization as well as open and suture of preritoneum are not necessary. It also provides enough space to place a mesh behind the round ligament. However, whether making a breach on the mesh would lead to an increased recurrence rate is still unknown. Although no recurrent case is noticed in the follow-up, further observation is obligated to discuss the safety of the method.


Anatomy of the preperitoneal space.

Closure of the breach on the mesh by fibrin glue.

Wrap the mesh around the round ligament.

Closure of the peritoneum.
To preserve the integrity of mesh, some suggest transecting the round ligament, passing it through the small hole cut on the mesh and then suturing the round ligament. This method of internal ring reconstruction is worth further study. It is feasible to choose between TAPP and TEP based on the surgeon's experience.
Conclusions
Laparoscopic inguinal hernia repair is already well developed. Meanwhile, there still remain questions to be discussed in female patients with groin hernias. In this study, it shows that the cysts on the round ligament could be resected during the procedure. Before transecting the round ligament, surgeons should comprehensively evaluate multiple factors of the patient. Either “open and suture” technique or “keyhole” technique is available to preserve the round ligament.
Footnotes
Disclosure Statement
No competing financial interests exist.