
Abstract
Abstract
Background:
We aimed to report surgical and oncological outcomes of renal cell carcinoma (RCC) patients with level I and II thrombus treated with laparoscopic transperitoneal radical nephrectomy.
Patients and Methods:
Medical records of 13 patients were reviewed retrospectively in a single center between 2005 and 2017. Hem-o-lok® clips were used to secure renal artery and renal vein, excluding 2 patients with an attached thrombus on the right side.
Results:
Seven male and 6 female patients were treated laparoscopically, and conversion to open surgery was not required in any case. The mean age was 61.6 ± 7.8 years (range 45 to 75 years) and the mean body mass index was 27 ± 4.6 kg/m2 (range 18.8 to 34.5 kg/m2). Median tumor size was 9.5 × 7.3 cm (range 5 to 14 cm) and 5 patients who had preoperative metastases underwent cytoreductive nephrectomy. The mean operative time was 137.6 ± 45.8 minutes (range 60 to 200 minutes) and blood loss was 105 ± 34.9 mL (range 50 to 150 mL). The mean hospital stay was 4.4 ± 3.9 days (range 1 to 15 days). Splenic capsular injury occurred in 1 patient and the vena cava was injured in another. Three patients needed blood transfusions. The mean follow-up period was 25 months (range 12 to 86 months).
Conclusion:
Laparoscopic transperitoneal radical nephrectomy can be reliable option for surgical management of RCC with level I and II thrombus in experienced centers.
Introduction
S
The incidence of the tumor thrombus extending into the RV, inferior vena cava (IVC), or atrium varies from 4% to 10% of all renal cell carcinomas (RCCs). 6 Presence of a thrombus in the RV or vena cava has a limited impact on prognosis in patients without lymph node involvement or visceral metastasis.7,8 Thus, proper surgical intervention is substantially important.
Laparoscopic or hand-assisted laparoscopic surgery for kidney tumors with RV thrombus has been reported as an oncologically reliable and effective technique in several case series.9–18 In this study, we aimed to report our surgical experience and the oncological results of kidney tumors with level I and II thrombosis treated with transperitoneal LRN.
Methods and Patients
After obtaining the approval of the ethics committee of Bulent Ecevit University, we reviewed database of LRN retrospectively at a single tertiary referral center. Between 2005 and 2017, 13 of the 755 patients had level I and II thrombus with kidney tumor. The Novick staging system was used in this study to describe the level of IVC tumor thrombus. Tumor thrombus extending <2 cm above the RV is staged as a level I, infrahepatic thrombus is staged as a level II, an intrahepatic IVC thrombus above the hepatic veins but below the diaphragm is staged as level III, and an IVC tumor thrombus extending above the diaphragm is staged as level IV.
Information regarding preoperative imaging, perioperative findings, postoperative complications, and oncological outcomes were recorded. Abdominopelvic and thoracic computerized tomography (CT) was routinely performed. Magnetic resonance imaging was performed only for particular patients with RV or IVC thrombosis on CT.
Surgical Technique
All patients underwent a standard transperitoneal laparoscopic approach with early control of renal artery. The patient was placed in the lateral decubitus position, pneumoperitoneum was created with carbon dioxide insufflation until 12 mm Hg intraperitoneal pressure was reached, and five-port configuration was used in all cases (three 10-mm and two 5-mm trocars). The ureter and gonadal vein were identified, and RV and renal artery were reached. Renal artery and vein were dissected and clipped using Hem-o-lok® clips. An interaortocaval dissection and early control of renal artery was employed for right-sided tumors with level II thrombus.
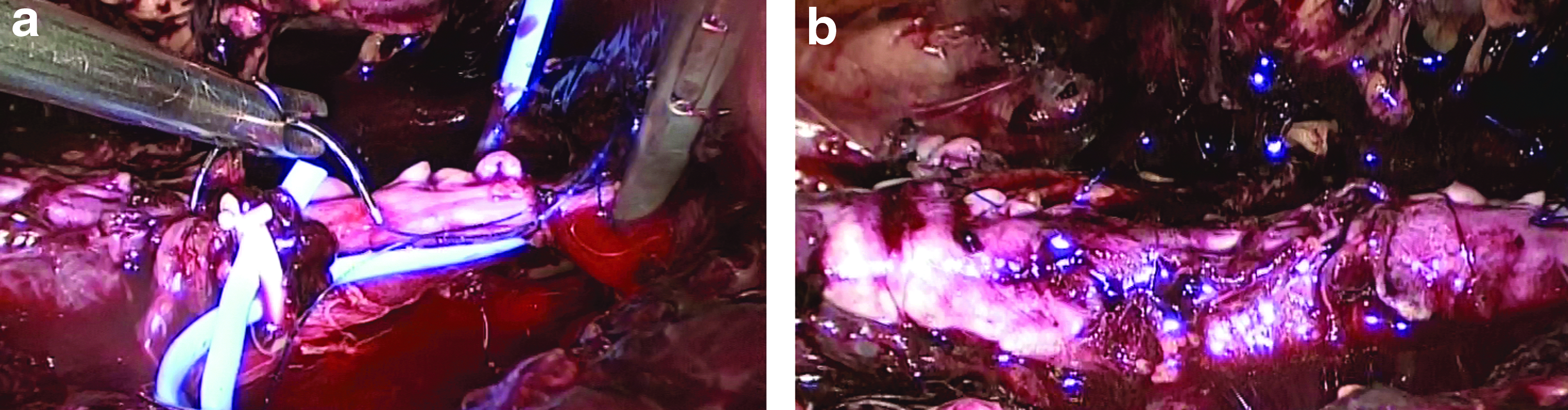
Interaortocaval space was dissected to secure renal artery as soon as possible in these 2 cases to provide oncological safety during the manipulation of renal mass. The infrarenal IVC, left RV, and suprarenal IVC were clamped using bulldog clamps in the right-sided tumors (Fig. 1). For the management of the thrombus, the RV was dissected individually and the tumor thrombus was clearly identified in the RV. The thrombus in the RV was managed using two different techniques. First, a floating thrombus was milked back with the help of suction irrigation cannula and secured with two Hem-o-lok clips after early control of the renal artery. Second, we used Endo GIA (U.S. Surgical Corp., Norwalk, CT) for patients with an attached thrombus on the right side. The IVC incision was sutured gently using a 3/0 Prolene (Ethicon, Somerville, NJ) suture to restore venous blood flow (Fig. 2). The surgical specimens were retrieved with a 15 mm Endo Catch™ (Covidien, Mansfield, MA) bag and pulled through the modified Gibson incision. Perihilar lymph node dissection was only performed in cases that were diagnosed preoperatively.

Vascular control of the vena cava was achieved by placing a laparoscopic Satinsky clamp just below the liver
Results
The mean age of the patients was 61.6 ± 7.8 years (range 45 to 75 years), and the mean body mass index was 27.0 ± 4.6 kg/m2 (range 18.8 to 34.5 kg/m2). Renal thrombus was identified preoperatively in 8 and intraoperatively in 5 patients. The mean tumor size was 9.5 × 7.3 cm (range 5 to 14 cm). The procedure was completed laparoscopically, and conversion to open surgery was not required in any case. The renal thrombus floating into the lumen of the RV was identified in 7 patients. Level II thrombus was detected in 2 patients in the IVC. Preoperatively identified lymph node dissection was carried out in 2 patients.
The mean operative time was 137.9 ± 45.8 minutes (range 60 to 200 minutes). The mean hospital stay was 4.46 ± 3.9 days (range 1 to 15 days). The mean blood loss was 105 ± 34.9 mL (range 50 to 150 mL).
Splenic capsular injury in 1 patient was repaired laparoscopically using surgicel absorbable hemostat. Vena cava injury was recorded in a patient due to close relationship between the renal mass and vena cava. A suction-irrigation cannula was used to occlude the caudal portion of the vena cava and laceration was sutured with 3/0 running Prolene sutures in that case.
Three patients required blood transfusions: 1 patient due to caval injury, another patient had a larger tumor, 14 cm diameter, and the third patient had preoperative deep anemia (Hb = 7.9 mg/dL).
Pathological examination revealed clear cell carcinoma in 11 and papillary renal carcinoma in 2 patients. The number of the patients with grade 2, 3, and 4 were 2, 9 and 2, respectively. All patients had T3b stage according to tumor node metastasis (TNM) classification. No positive surgical margins were identified and no local recurrence was observed during the follow-up period.
A total of 8 patients received adjuvant interferon treatment during the follow-up period. One patient who had undergone nephrectomy for cytoreductive purposes refused the adjuvant therapy. Four patients without any adjuvant treatment were free of tumor recurrence or metastasis. Pulmonary metastasis developed in one of the patients at the 13 months, and liver metastasis developed at the ten months postoperatively. Eight patients received interferon: 4 for preoperative metastasis, 1 for the liver metastasis at the 10th month, 1 patient for the lung metastasis at the 13th month post surgery, and 2 patients received interferon and radiotherapy treatment for bone metastasis. Six patients received targeted therapy due to progression after interferon treatment. Although the follow-up was relatively short, no cases of local recurrence developed. Four patients without metastatic disease at nephrectomy were disease free. Characteristics of the patients and surgical outcomes are presented in Tables 1 and 2, respectively.
Patient Characteristics (n = 13)
BMI, body mass index; CT, computerized tomography; MRI, magnetic resonance imaging.
Perioperative and Postoperative Parameters
IVC, inferior vena cava; RCC, renal cell carcinoma; TNM, tumor node metastasis.
Discussion
Extension of the thrombus in the RV is not rare and can be challenging during laparoscopy. 6 Although increased experience in laparoscopic surgery has encouraged the urologists to perform more complex operations, there is still no standard approach for thrombus in the RV.1,4
In 2003 Desai et al. reported the first case series of laparoscopic management of RV thrombus in 8 patients and defined their technique as early control of the renal artery and milking back of the thrombus with jaws of the Endo GIA stapler and securing the RV. 9 They also reported conversion to open surgery in 1 patient due to uncontrollable bleeding.
Following these series, Kapoor et al. reported a case series of 12 patients with no intraoperative complication using the same technique in 6 patients and hand-assisted laparoscopy in the others. They also reported two open surgery conversions. 10
Similar outcomes with laparoscopic and hand-assisted approaches were reported using either vascular clips or endoscopic stapling devices. 19 In a recently published study, different techniques were described to secure RV, including Hem-o-lok clip, vicryl ligature, prolene suture, and hand assistance. 20 Henderson et al. reported conversion to open surgery in 2 patients due to vena cava laceration and excessive bleeding. 19 In cases of serious bleeding or incomplete removal of the thrombus, conversion to open surgery should be kept in mind. Therefore, the surgeon must have both laparoscopic and open surgical experience. Conversion to open surgery was not required in our series. We also did not use any hand assistance.
In the present study, we used two different techniques for management of the RV: A suction irrigation cannula was used for milking back off the floating thrombus with the assistance of two Hem-o-lok clips placed to secure the vein, and an interaortocaval dissection and early control of the renal artery was employed for right-sided tumors with level II thrombus to secure the renal artery as quickly as possible, providing oncological safety and reducing collateral vein bleeding. A stapler device was used for the right-sided tumors with an attached thrombus.
In addition to advanced laparoscopy experience of the surgeon, we believe that limited RV dissection, minimal kidney mobilization, and early ligation of the renal artery are the important maneuvers to prevent or minimize the migration of the tumor thrombus. It is harder to manage the RV thrombus on the right side because of shorter length of the right renal artery. Prevention of collateral venous bleeding can be provided using early interaortocaval dissection of right the renal artery. The left renal artery can be controlled by finding the aorta directly.
Renal thrombus was identified preoperatively in 8 and intraoperatively in 5 patients. Desai et al. reported that preoperative CT did not show evidence of a RV thrombus, while there was doubtful involvement in 7 cases. 9 Surgical planning is dependent on preoperative imaging, so it should be noted that segmental RV involvement may be difficult to identify with current radiological imaging techniques.
Use of perioperative ultrasonography (US) was reported, especially in the first case series.10,11 US can be useful when the thrombus is not visualized or for determining the proximal extension of the tumor thrombus intraoperatively. In the present study, the use of US was not necessary.
Mean blood loss in the present study was comparable with other reports. Median blood loss up to 275 mL has been reported in the literature during LRN with level II IVC thrombus.17,21
Cytoreductive surgery contributes to survival in metastatic disease. 22 Eight patients received adjuvant interferon treatment in follow-up period, but only 1 patient denied the therapy who undergone cytoreductive surgery.
LRN in patients with venous thrombus is not always free of complications, and surgeons should have advanced laparoscopic skills to bear any complication including an injury to vena cava. In our series, we faced vena cava laceration in 1 patient, which was repaired with a Prolene suture laparoscopically. The tumor diameter was 11 cm in this patient and the tumor was adjacent to IVC.
Tumor-free surgical margins is another important aspect of a successful surgery. Basic oncological principles have been applied in our series, and all of the patients had negative surgical margins while performing LRN. Safety and the short-term oncological efficacy of LRN and thrombectomy have been demonstrated in our study for RCC patients with level I and II thrombus.
Conclusions
Renal masses with level I and II thrombus can be laparoscopically managed with comparable oncological outcomes in experienced centers. Conversion to open surgery should be kept in mind; therefore, the surgeon must have both advanced laparoscopic and open surgical experience. Limitation of the present study was the short-term oncological outcomes for this approach. Long-term follow-up reports and randomized studies are needed with a larger number of patients to evaluate the oncologic outcomes of LRN for RCC with level I and II thrombus.
Footnotes
Disclosure Statement
No competing financial interests exist.