
Abstract
Abstract
Introduction:
Studies have shown that Epworth sleepiness scale (ESS) is not a good tool to predict obstructive sleep apnea (OSA). However, data regarding the accuracy of ESS in the prediction of OSA among morbidly obese patients are scarce.
Methods:
The study involved a retrospective review of the charts of the consecutive patients who underwent bariatric surgery at a tertiary care teaching hospital. All the patients underwent polysomnography (PSG) and undertook the ESS questionnaire. The sensitivity and specificity of ESS were calculated based on its correlation with the PSG findings. Furthermore, a new score was devised to improve the utility of ESS to predict OSA.
Results:
A total of 232 consecutive patients from January 2014 to July 2017 were included in the study. The mean age and body mass index (BMI) were 40.5 ± 11.8 years and 47.6 ± 7.3 kg/m2, respectively. Among the 162 patients who had an ESS <10, 57.4% had moderate-to-severe OSA. The sensitivity of ESS to predict moderate-to-severe OSA was found to be 38.8% and the positive predictive value was 84.2% (positive likelihood ratio 2.82, 95% confidence interval = 1.57–5.06). A predictive score was identified as 0.031Age (years) +0.039BMI (kg/m2) + 0.038ESS + Gender (1 for male, 0 for female). The score had a sensitivity of 80% at a cutoff of 3.3.
Conclusions:
Among the morbidly obese, ESS is a poor predictor of OSA. Its utility as a tool for prediction of moderate-to-severe OSA can be improved by use of a new formula incorporating age, gender, and BMI beside ESS.
Introduction
P
Materials and Methods
The study involved the retrospective review of the charts of all the consecutive patients who underwent bariatric surgery at a tertiary care teaching hospital. All the patients underwent PSG as a part of the preoperative evaluation for bariatric surgery and undertook the ESS questionnaire. ESS is a questionnaire to assess the tendency to fall asleep during eight daily activities and the score ranges from 0 to 24. 13 (The ESS score is provided in the Supplementary Data.) An ESS score >10 was taken as an indicator of the presence of excessive daytime reference sleepiness and OSA. Apnea–hypopnea index (AHI) of 5 or less was considered as normal. An AHI of 5–15 was considered as mild, 15–30 as moderate, and >30 as severe sleep apnea. An AHI of >15 (moderate and severe OSA) was taken as clinically significant. 14 The data were analyzed to assess the utility of ESS to predict OSA, considering overnight PSG to be the gold standard for diagnosis of OSA.
For the purpose of assessing the feasibility of a better predictive model for clinically significant OSA in our population, the data set was divided randomly into derivation and validation subgroups in an approximately 2:1 ratio. The derivation subgroup was used to construct a score to predict OSA. This score was then tested in the validation subgroup.
All the analyses were performed using IBM SPSS Statistics Version 20 and Microsoft Excel 2016. The demographic and other clinical details were analyzed for all the patients and compared among those with and without clinically significant OSA. A multivariate regression analysis taking moderate-to-severe OSA as the outcome measure was then conducted on the derivation subgroup, using the logistic regression model. In constructing the model, a step-up approach was followed to include as many variables in the regression equation as possible. The B coefficients of the variables found significant in the logistic regression model were then aggregated to a composite score. To ensure that the efficacy of the predictive model is not restricted to the data on which it was built, comparison with ESS was made on the separate validation cohort. A receiver operator characteristics (ROC) curve was then constructed for the composite score and was compared with ESS to assess its role in OSA prediction.
Results
A total of 232 consecutive patients presenting for bariatric surgery from January 2014 to July 2017 were included. In the study population, the proportion of women was 69.8%. The mean age, weight, and body mass index (BMI) were 40.5 ± 11.8 years, 123.2 ± 23.8 kg, and 47.6 ± 7.3 kg/m2, respectively.
On PSG, 199 (85.7%) patients had OSA (AHI >5) and 152 patients (65.6%) had moderate or severe OSA (AHI >15).
In accordance with the ESS questionnaire, 70 patients (30.1%) had symptoms of EDS (ESS score >10). Among these 70 patients, who had ESS >10, 59 patients (84%) had an AHI >15 and 11 (15.7%) had an AHI <15 as shown in Figure 1. Of the remaining 162 patients who had an ESS <10, a significant majority (93 patients, 57.4%) also had moderate-to-severe OSA (AHI >15) as shown in Figure 2. The sensitivity of ESS to predict moderate-to-severe OSA was found to be 38.8% and the positive predictive value was 84.2% (positive likelihood ratio 2.82, 95% confidence interval = 1.57–5.06). The cross-tabulation of ESS score versus AHI is given in Table 1.
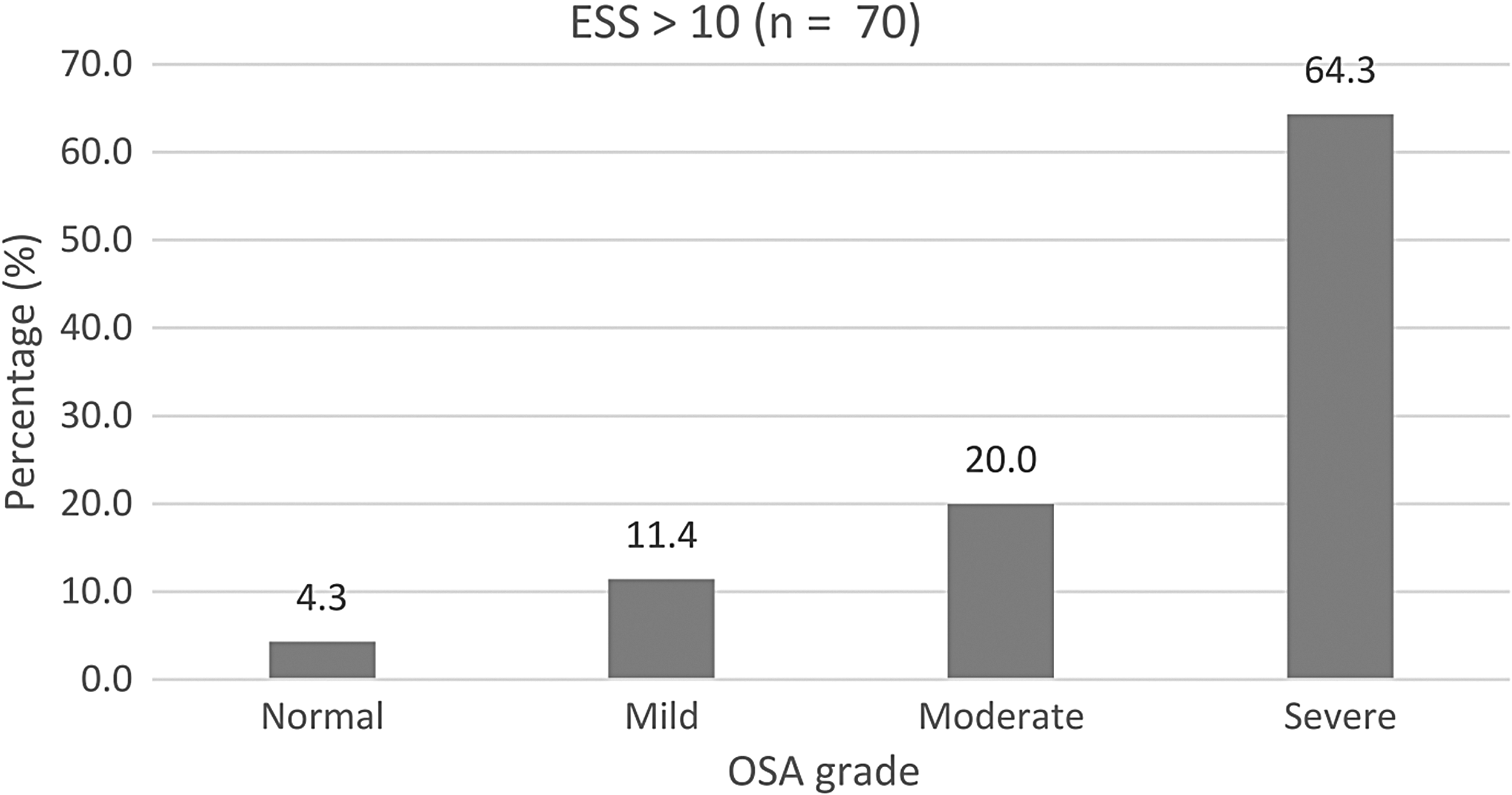
Presence of obstructive sleep apnea in morbidly obese patients with ESS >10. ESS, Epworth sleepiness scale.
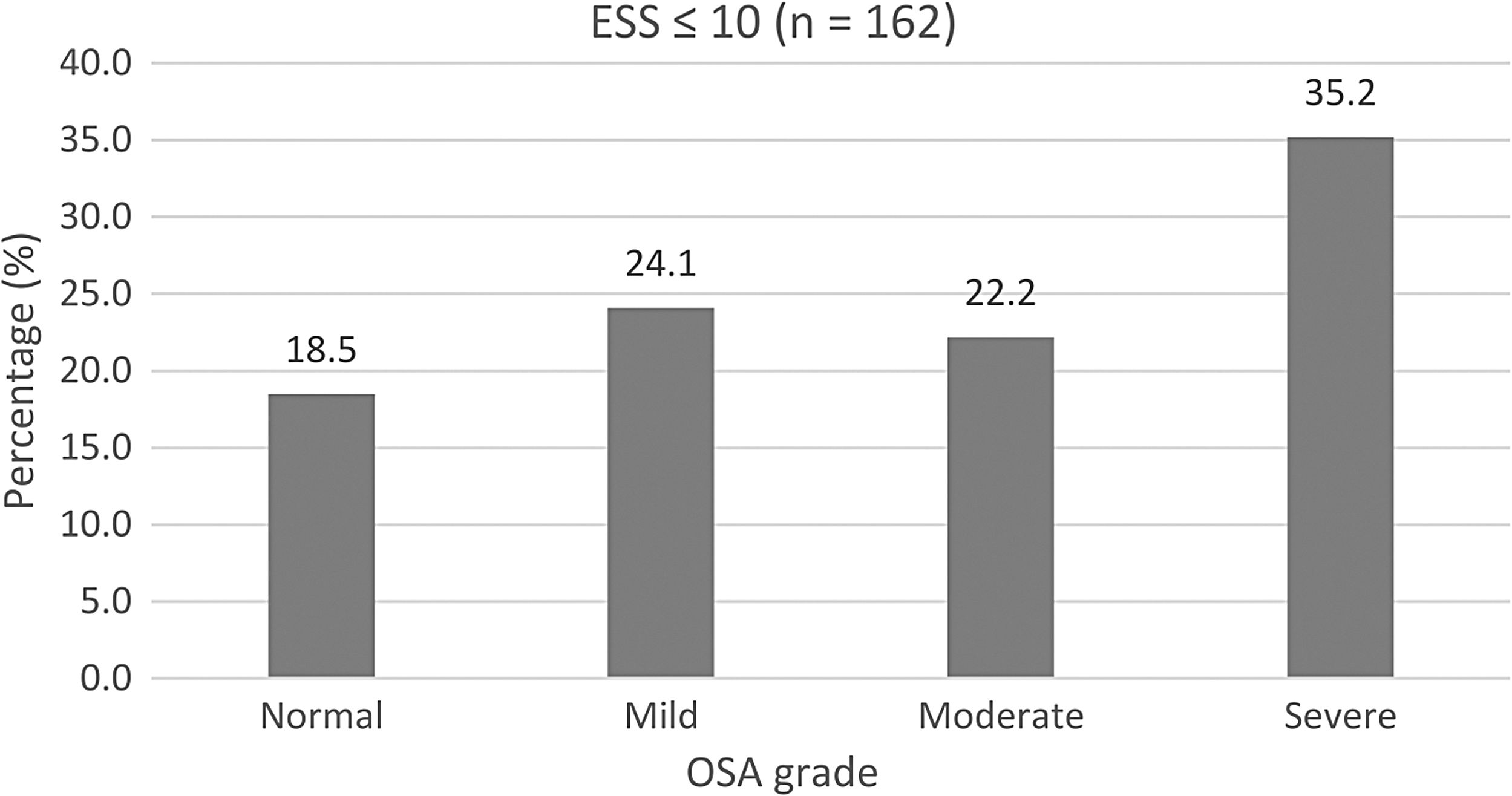
Presence of obstructive sleep apnea in morbidly obese patients with ESS <10.
AHI, apnea–hypopnea index; ESS, Epworth sleepiness scale.
A logistic regression model was thereafter constructed on the derivation cohort (n = 148) using moderate-to-severe OSA as the outcome variable. Four variables were found to have independent predictive value for the outcome: age, gender, BMI, and ESS. Using these four variables, a predictive score was identified as 0.031Age (years) +0.039BMI (kg/m2) + 0.038ESS + Gender (1 for male, 0 for female). A cutoff of 3.3 was identified to have the best predictive value in the derivation cohort.
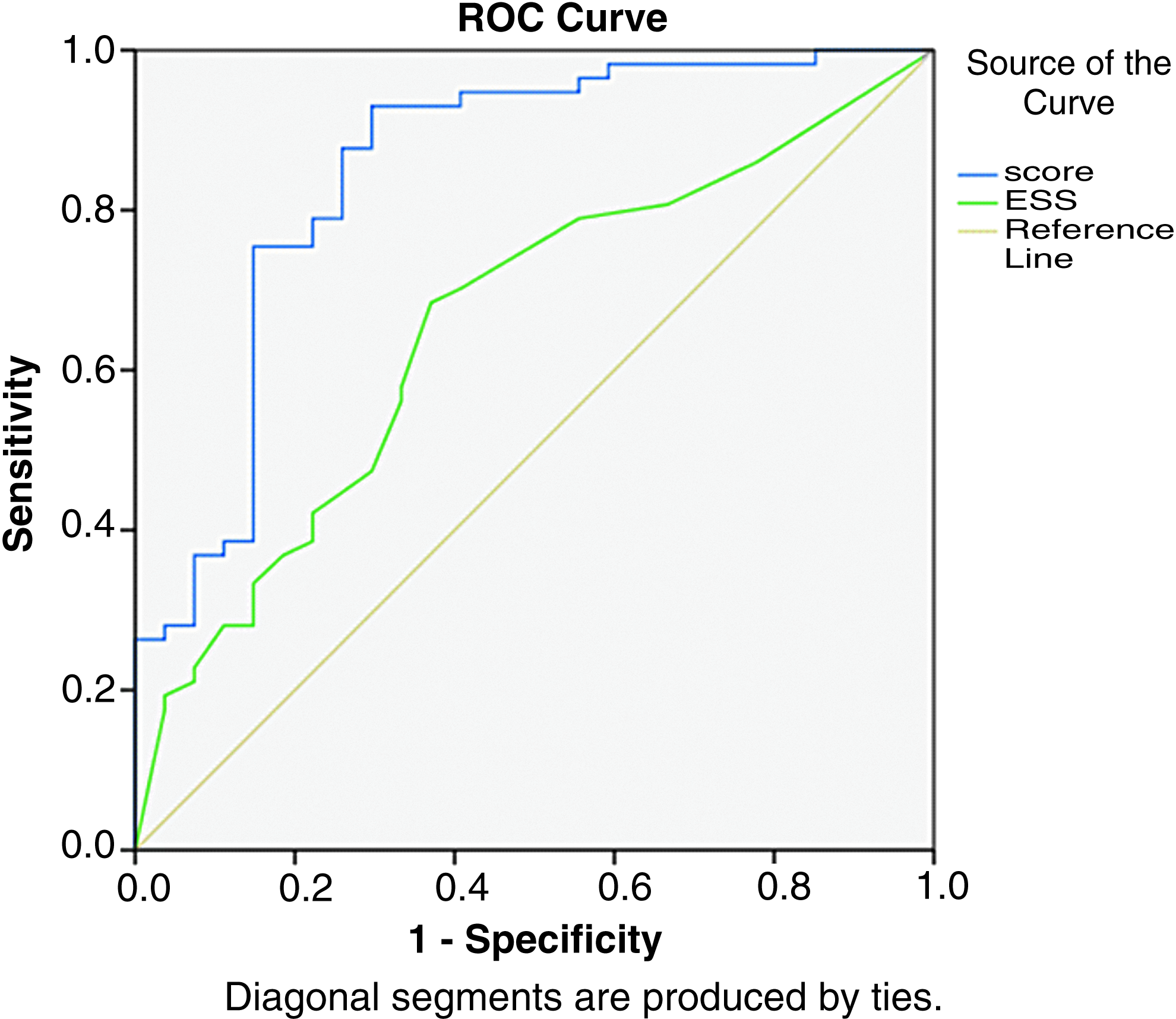
The positive predictive value of this score was found to be 79.6%, with a sensitivity of 80% and a specificity of 62.3% at a cutoff of 3.3 in the derivation cohort. The cross-tabulation of this predicted new score versus AHI is given in Table 2. An ROC curve was calculated for different cutoffs of the predictive score for the derivation cohort (Fig. 3). The area under the ROC curve (AUROC) for the score was 0.807, P < .001, which was better than that for ESS, which was 0.657, P = .002, as given in Table 3.

Receiver operator curve for the derivation cohort.
AHI, apnea–hypopnea index.
ESS, Epworth sleepiness scale.
This predictive score performed better in the validation cohort as well. The AUROC for the score was 0.848, P < .001, which was better than that for ESS, which was 0.657, P = .02, as given in Table 4. Of the 84 patients, 69 (82.1%) were correctly classified to whether or not they have clinically significant OSA. The ROC curve for validation cohort is shown in Figure 4. The AUROC for the predicted score was 0.848, P < .001, which was significantly better than that for ESS (0.657, P = .02). The variables with their B value and significance are given in Table 5.
Receiver operator curve for the validation cohort.
ESS, Epworth sleepiness scale.
BMI, body mass index; ESS, Epworth sleepiness scale.
Discussion
OSA is highly prevalent in obese individuals.1,15 OSA has a prevalence of 70% to 80% in morbidly obese patients who present for bariatric surgery.1,16 It is important to recognize these patients preoperatively as they may require the use of positive airway pressure 17 to avoid postoperative respiratory complications. 4 PSG has been the gold standard for diagnosis of OSA. 18 ESS has been generally used as a predictor of OSA but with unreliable results.6,7 Majority of these studies were carried out in the general population. In our study, we evaluated the reliability of ESS to predict moderate-to-severe OSA in a morbidly obese population, in whom the prevalence of OSA is higher than in the general population.
Our study population had a mean BMI of 47.6 ± 7.3 kg/m2. We found that the sensitivity of ESS to predict moderate-to-severe OSA was 38.8%, and the positive predictive value was 84.2%. The negative predictive value was found to be 42.9%. Ravesloot et al. in their study on 289 morbidly obese patients performed stepwise linear regression taking AHI as the dependent variable. They found that ESS was not a significant predictor of OSA. 9 They showed that BMI to be a more significant predictor of OSA than ESS. Dixon et al. in their study on 99 morbidly obese patients found that ESS is not a significant predictor of the presence of OSA. 12 In another study by them, it was seen that ESS was a significant predictor of OSA. However, in this study, PSG was performed only in patients with ESS >10. 11 Sareli et al. found that 42% (88/209) of the patients (planned for bariatric surgery) with an ESS score <10 suffered from moderate-to-severe OSA. 10 In the general population, the sensitivity of the ESS score to predict OSA ranged from 50% to 65%.8,19,20 The low sensitivity of ESS in our study (38%) could be because of a higher prevalence of OSA in morbidly obese patients, which was 85.7% in our study and 65.6% for moderate-to-severe OSA.
In the logistic regression model on the data of our study population, age, gender, and BMI besides ESS were found to be significant predictors of OSA. Prevalence of OSA increases with age because of increased fat deposition around parapharyngeal areas, dysfunction of pharyngeal muscles, and lengthening of soft palate.21,22 It is estimated that ∼60% of moderate-to-severe OSA can be attributed to obesity with both having a similar genetic basis. Up to 35% to 40% of genetic variance for OSA has been found to match with that of obesity. 23 Male gender is an independent risk factor for the presence of OSA. It may be due to the effect of hormones on the upper airway muscles in women and higher neck circumference in men. The difference, however, persists even after eliminating these factors. 24 Basoglu et al. in their study concluded that sleep apnea is underdiagnosed in women, as they do not report classical symptoms of sleep apnea. They generally tend to present with insomnia rather than the typical symptoms of loud snoring, witnessed apneas, or sleepiness. 25
In a study carried out by Christina et al., it was seen that BMI, American Society of Anesthesiologists (ASA) score, age, and comorbidities including hypertension and diabetes were significant predictors of OSA. They developed a score using these parameters with a sensitivity and specificity of 72% and 76%, respectively. 26 Other parameters such as neck circumference, snoring, and reports of nocturnal gasping can also be used to predict OSA as shown in their studies by Flemons et al. and Deflandre et al.27,28 Deflandre et al. developed the * DES-OSA score based on BMI, the distance between chin and thyroid, Mallampati score, and neck circumference with a sensitivity of 77%.
Our study addresses an important clinical question—namely how to identify obese subjects with OSA before bariatric surgery. ESS is a subjective tool devised to predict EDS. EDS is an important marker of OSA, although other factors such as age, gender, BMI, and neck circumference also play a role. This might result in a poor sensitivity of ESS to predict OSA. We have attempted to improve the predictive power of ESS by building a population-specific predictive equation in morbidly obese patients. PSG should be a part of routine preoperative workup for bariatric surgery as advocated in other studies as well. 29
However, there are certain limitations to our study. Our study is retrospective in nature. It was carried out in a single center. Moreover, external validation of the predicted score (using the derivation subgroup) has not been performed.
Conclusion
PSG should be performed routinely in patients planned for bariatric surgery as advocated in other studies as well. Among the morbidly obese, ESS is a poor predictor of OSA. Its utility as a tool for prediction of moderate-to-severe OSA can be improved by use of the predicted score incorporating age, gender, and BMI besides ESS.
Footnotes
Acknowledgments
The authors thank Rachna Chaudhary, Secretary to Professor Sandeep Aggarwal, Department of Surgical Disciplines, AIIMS, New Delhi.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.