
Abstract
Aim:
This study aimed to compare the surgical outcomes of patients with the intermediate-type imperforate anus who underwent laparoscopically assisted anorectoplasty (LAARP; L group) with those of patients who underwent sacroperineal anorectoplasty (S group).
Materials and Methods:
The medical records of patients with intermediate-type imperforate anus at a single institution between April 1983 and April 2017 were retrospectively reviewed. Fecal continence was evaluated using the clinical assessment score for fecal continence developed by the Japanese Study Group of Anorectal Anomalies (maximum score, 8).
Results:
Twelve cases (rectobulbar urethral fistula, 7; anal agenesis without fistula, 4; and rectovaginal fistula, 1) were included in the L group versus 14 cases (rectobulbar urethral fistula, 11, and anal agenesis without fistula, 3) in the S group. Age and body weight at the time of surgery and rate of associated anomalies did not differ significantly between the two groups. The total scores for fecal continence 3, 5, and 7 years after anorectoplasty were 4, 5, and 4 points in the L group and 4, 5, and 6 points in the S group, respectively, showing no significant intergroup differences. Mucosal prolapse occurred in 50% of the L group and 29% of the S group (P = .42), but failed rectocutaneous anastomosis and anal stenosis were not identified in either group.
Conclusions:
Postoperative fecal continence and the incidence of complications after LAARP were comparable with those after sacroperineal anorectoplasty in patients with intermediate-type imperforate anus.
Introduction
Laparoscopically assisted anorectoplasty (LAARP) was introduced in 2000. 1 Several studies have compared the results of LAARP with those of the conventional approach, and laparoscopic approach has been shown to be beneficial in cases of rectobladder neck fistula. 2 For intermediate-type imperforate anus, application of the laparoscopic approach is controversial because manipulation in the deep and small pelvic cavity is technically demanding and creates concern of residual urethral fistula.3–6 Recent articles showed that LAARP in cases of rectobulbar urethral fistula is technically feasible without residual urethral diverticulum7–9 and functionally superior to posterior sagittal anorectoplasty. 10 However, evidence that fecal continence after laparoscopic repair is superior to that after the conventional approach is still lacking.
The aim of this study was to compare postoperative complications and fecal continence of patients with intermediate-type imperforate anus who underwent LAARP or sacroperineal anorectoplasty.
Materials and Methods
The medical records of patients with intermediate-type imperforate anus who underwent anorectoplasty at Saitama Children's Medical Center between April 1983 and April 2017 were retrospectively reviewed. Our hospital was founded in April 1983 and standard sacroperineal anorectoplasty was routinely performed. LAARP was introduced as the standard procedure in 2000. The procedure used in this study was subjected to minor modifications such as introducing a method to measure the residual rectourethral fistula8,11 based on the original procedure, 12 and a muscle stimulator has been used to detect the center of the puborectalis muscle from the beginning. 12
Data on patient characteristics (gender, anorectal malformation type, associated anomalies including sacral deformity or spinal pathology, age and weight at anorectoplasty, procedure time, and bleeding amount), postoperative complications (mucosal prolapse, failed rectocutaneous anastomosis, anal stenosis, and residual urethral fistula), and fecal continence were collected. Intermediate-type imperforate anus includes rectobulbar fistula, anal agenesis without fistula, anorectal stenosis, rectovaginal fistula (low), and rectovestibular fistula according to the International Classification of Anorectal Anomalies proposed in 1971. 13 Fecal continence was evaluated using the clinical assessment score for fecal continence developed by the Japanese Study Group of Anorectal Anomalies in 1982 and is commonly used in Japan. The scoring system is composed of four items: urge to defecate (0–2 points), constipation (1–4), incontinence (0–4), and soiling (0–2). The total score (maximum, 8) is calculated as the sum of urge to defecate, constipation or incontinence (whichever is smaller), and soiling, with higher scores indicating better fecal continence (Table 1).14,15 This study extracted the scores at 3, 5, and 7 years postanorectoplasty.
The total score is 1–8, which is the sum of urge to defecate, constipation or incontinence (smaller one), and soiling.
Statistical analysis was performed by the Steel–Dwass method for nonparametric multiple comparisons and Fisher's exact test for contingency tables using a commercially available software (JMP® Pro 11.0.0; SAS Institute Japan Ltd., Tokyo, Japan). P values <.05 were considered statistically significant. All data are shown as median (range).
This retrospective observational study was approved by the ethics committee of Saitama Children's Medical Center.
Results
LAARP was performed in 12 patients (rectobulbar urethral fistula, 7; anal agenesis without fistula, 4; and rectovaginal fistula, 1: L group) and sacroperineal anorectoplasty was performed in 14 patients (rectobulbar urethral fistula, 11, and anal agenesis without fistula, 3; S group). Patient characteristics are given in Table 2. There were no statistically significant differences in imperforate anus type, gender ratio, rate of patients with associated anomalies, or age and weight at anorectoplasty between the L and S groups. The procedure time was longer (P < .001) and bleeding amount was smaller (P = .03) in the L group than in the S group.
Patient Characteristics
Spinal lipoma.
Trisomy 21, 4; 22q11.2 deletion syndrome, 1; unknown etiology, 1.
Trisomy 21, 3; Opitz syndrome, 1; Pfeiffer syndrome, 1.
LAARP, laparoscopically assisted anorectoplasty.
Mucosal prolapse occurred in 50% of the L group and 29% of the S group, but the intergroup difference was insignificant (P = .42). Failed rectocutaneous anastomosis and anal stenosis were not identified in either group. Postoperative magnetic resonance imaging (MRI) was performed in 9 patients of the L group versus 2 patients of the S group. Residual urethral fistula was detected in 5 patients (56%) of the L group versus 0 patients of the S group (Table 3).
Postoperative Complications
LAARP, laparoscopically assisted anorectoplasty.
Patients with intellectual disability (6 in the L group and 5 in the S group) were excluded from the evaluation of postoperative fecal continence. Some data were missing in this retrospective review. The total score for fecal continence 3, 5, and 7 years after the surgery were 4, 5, and 4 points in the L group and 4, 5, and 6 points in the S group, respectively, showing no significant intergroup differences (Fig. 1). Scores at any time point in each item also showed no significant intergroup differences (Fig. 2).
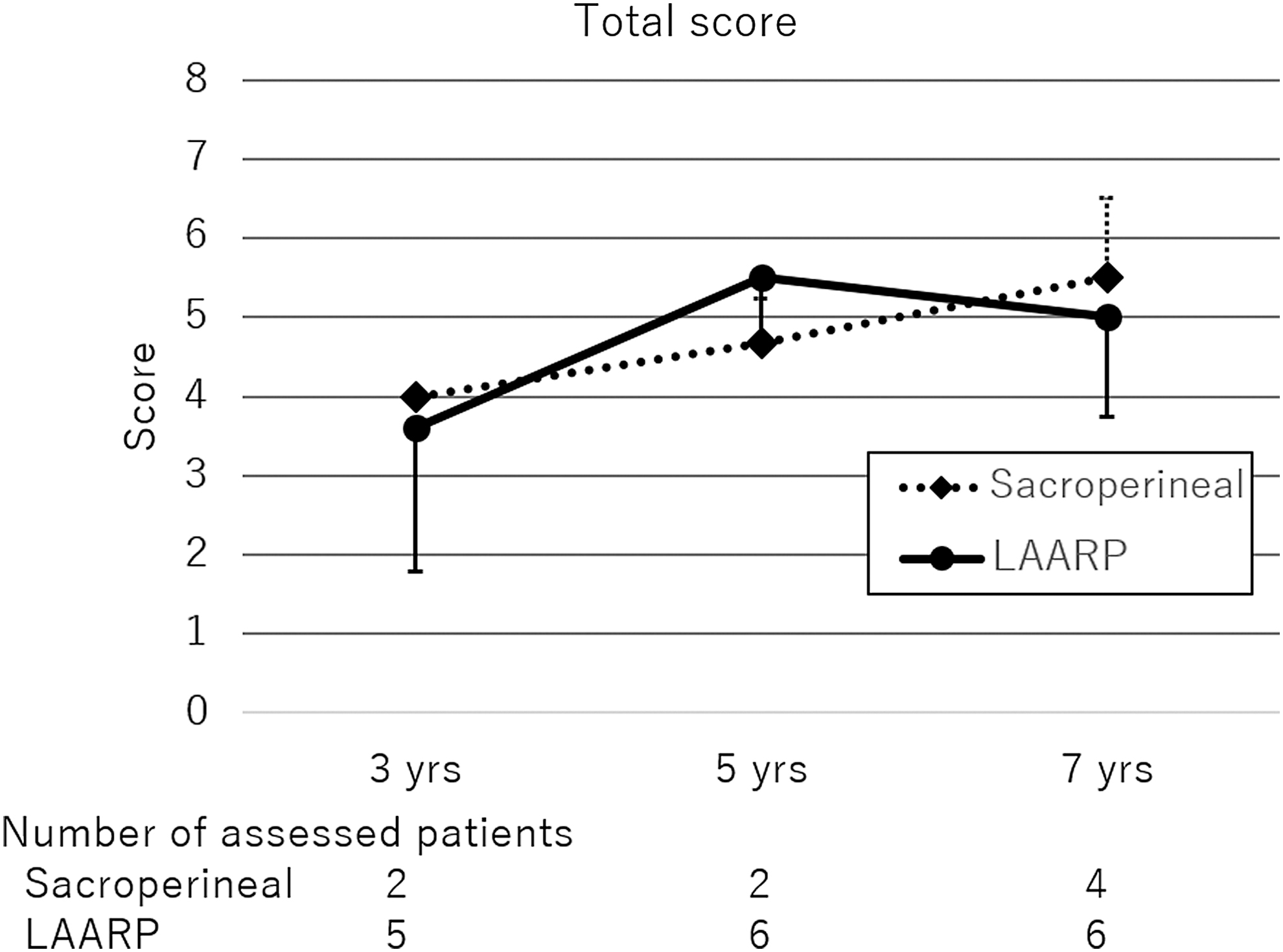
Total score of the clinical assessment for fecal continence. LAARP, laparoscopically assisted anorectoplasty.
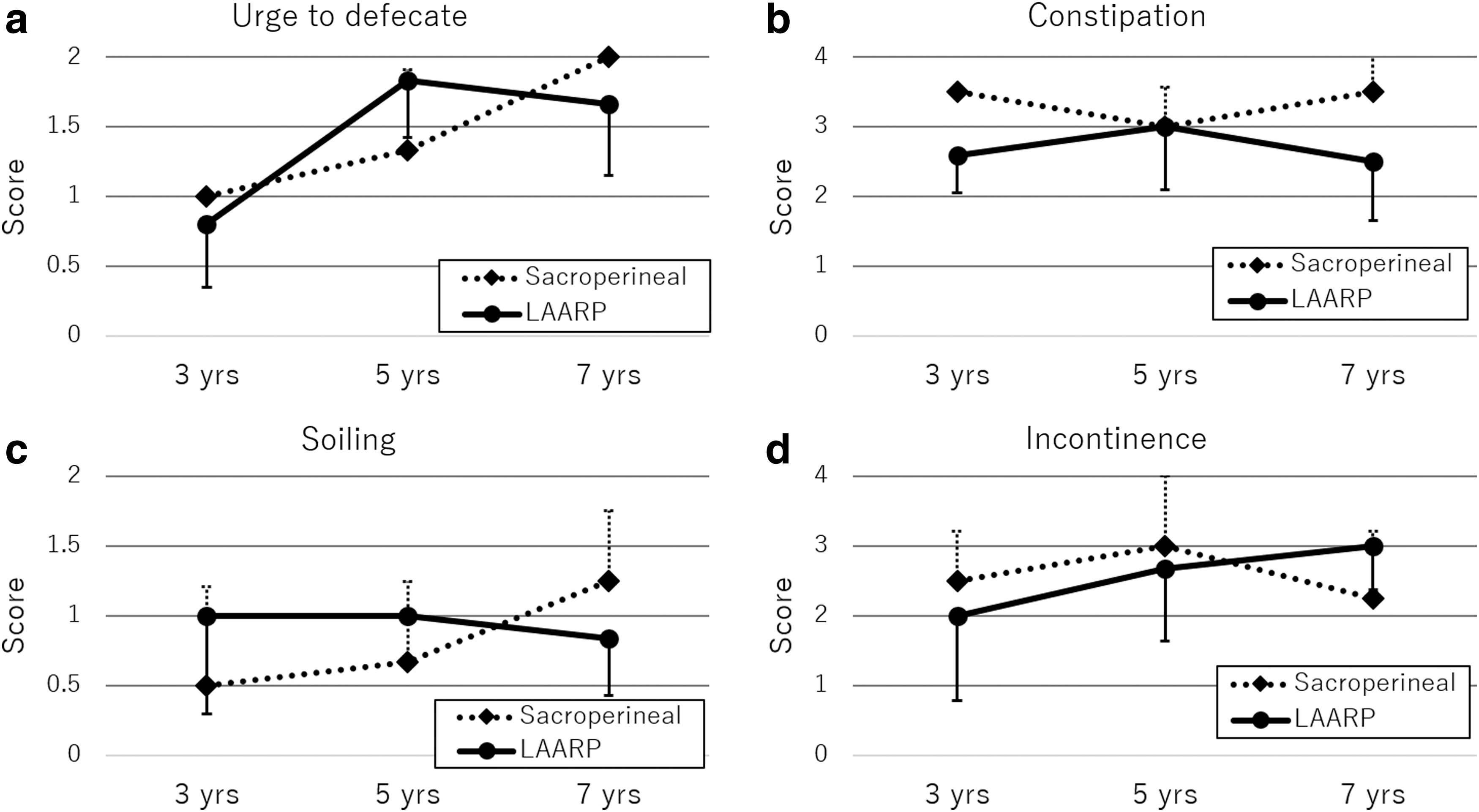
Each item of the clinical assessment for fecal continence.
Discussion
This study showed that postoperative fecal continence of patients with intermediate-type imperforate anus who were treated laparoscopically was comparable with that of those treated with conventional sacroperineal approach. The noninferiority of LAARP to the sacroperineal approach in terms of fecal functionality was seen not only in the total score but also in each item at any time point, that is, urge to defecate, constipation, incontinence, and soiling after 3, 5, and 7 years postanorectoplasty. Fecal continence is expected to improve as patients grow, 10 but the total score of the L group at 7 years postanorectoplasty decreased from the previous time point (5 years after the procedure). As for each item, only the score of incontinence at 7 years postsurgery increased from the previous time point, whereas those of the other three items decreased. This scoring system is subjective based on caregiver reports at the outpatient clinic visits and primary doctors changing for some patients during the study period. Caregivers might assess fecal continence more strictly as their child matured because they expected their child to regain continence once of school age. These factors may have affected the score of incontinence and resulted in lower scores than it really was. The number of patients was small, especially in the S group, due to the exclusion of patients with intellectual disability to strictly evaluate postoperative fecal continence and the missing data for some patients. Patients in the S group were treated with anorectoplasty in the 1980s or 1990s and had been classified as the intermediate type using the International Classification of Anorectal Anomalies proposed in 1971. This old classification was then applied to the cases in the L group. Yazaki et al. showed that functional outcomes appear to favor LAARP over posterior sagittal anorectoplasty for rectobulbar fistula. 10 Our results did not show superiority of fecal continence after LAARP but at least showed noninferiority of LAARP to the sacroperineal approach.
The incidence of mucosal prolapse was higher in LAARP patients.10,16 A similar tendency was found in this study. In LAARP patients, the dissection must be started from peritoneal reflection, whereas in the S group, the dissection was performed within the lesser pelvic cavity. The dissection lengths of the colon and the rectum in the L group were longer than those in the S group. We anchored the rectum wall to the pull-through route using four stitches, but these did not provide reasonable efficacy for rectopexy. This extensive dissection might have affected the higher incidence of mucosal prolapse, which seemed to occur in a certain number of patients regardless of approach, because the muscle complex that circumferentially supports the rectum is naturally immature in patients with high- or intermediate-type imperforate anus. Nonetheless, the definitive reason for this is unknown, and some technical modifications are needed to improve this complication.
Regarding technical aspects, the application of laparoscopy to intermediate-type imperforate anus has been controversial because of difficulties in dissection and ligature of the fistula and the higher incidence of posterior urethral diverticulum,2,17 but recent reports insisted that patients with rectobulbar fistula can be treated laparoscopically without the formation of a postoperative residual urethral fistula of the same quality as those with rectoprostatic fistula.7,8 One of the coauthors reported residual fistula after LAARP in 2008. 6 Since then, we perform MRI in all patients after LAARP. In addition, patients who underwent anorectoplasty before 2008 also underwent MRI, but some patients had lost outpatient visit. Therefore, unfortunately, this study did not examine residual fistula in all the cases, especially in the S group, and identified residual fistula in 5 out of 9 (56%) patients in the L group. However, for all complicated cases, patients were treated with anorectoplasty before intraoperative residual rectourethral fistula measurement 11 was introduced into our procedure in 2008. The procedure time was significantly longer in the L group than in the S group. Technical difficulties in manipulating the laparoscopic forceps in the deep and small pelvic cavity may have impacted this time difference, but the difference was partly due to the introduction of the mentioned technique. In fact, the operative times of LAARP before and after the introduction of the technique were 224 (173–241) and 243 (188–316) minutes, respectively. The extended time was not long, and use of this technique has decreased the incidence of residual fistula, suggesting that it effectively prevents this complication.
This study has a few limitations that merit consideration. The sample size was not large and the data were collected retrospectively. In addition, various surgeons performed the procedures, although they were always supervised by an expert. These issues could result in a bias in our data and findings.
Despite these limitations, this study's findings suggest that postoperative fecal continence and the incidence of complications after LAARP were comparable with those after sacroperineal anorectoplasty in patients with intermediate-type imperforate anus. Mucosal prolapse tends to occur more often in patients after LAARP, and an investigation into its cause and preventive measures is needed. LAARP carries the potential risk of postoperative urethral diverticulum when used in cases of rectobulbar fistula, but it can be overcome by technical refinement using intraoperative measurement of the urethral fistula. A multicenter prospective study is needed to confirm superiority of LAARP to the sacroperineal approach.