
Abstract
Abstract
Background:
Total-laparoscopic intragastric surgery (T-LIGS) has gradually been accepted for the treatment of endogenous gastric submucosal tumors. However, it is difficult to perform T-LIGS when the tumor is located at the esophagogastric junction (cardia endogenous gastric submucosal tumor [CEGSMT]) without special laparoscopic instruments that are not available in most developing countries. We have successfully treated 12 cases of CEGSMTs using conventional laparoscopic instruments and achieved acceptable outcomes. This study was conducted to evaluate the surgical techniques for CEGSMT management.
Methods:
A retrospective analysis was conducted involving all the CEGSMT patients who were treated with T-LIGS in the General Surgery Department of Guangdong General Hospital from August 2014 to June 2016.
Results:
There were 12 patients successfully treated with T-LIGS. The surgical time ranged from 56 to 108 minutes, and the blood loss was 5–70 mL. The distance to the tumor from the dentate line was 12–24 mm, and the tumor diameter was 17–28 mm. The tumor margins were 9–15 mm, and the eating time was 2–4 days. The drainage tube indwelling time was 2–4 days, and the discharge time was 4–6 days. The follow-up exams revealed no recurrences, dysphagia, acid reflux, or other digestive symptoms.
Conclusions:
It is safe and feasible to perform T-LIGS using conventional laparoscopic instruments to treat CEGSMTs. We suggest that T-LIGS can be performed for endogenous mucosal tumors within 3 cm from the cardiac dentate line and less than 3 cm in size.
Introduction
G
Materials and Methods
The technology has been identified as the “new technology project of Guangdong General Hospital,” and all patients provided informed consent before treatment.
Patients
From August 2015 to June 2017, all 12 patients (4 males and 8 females; range: 30–54 years) received endoscopic ultrasound endoscopy and CT scans. The preoperative evaluation detected tumors within 2.5 cm from the cardia dentate line. There were six tumors located in the lesser curvature of the stomach, five were on the posterior gastric wall, and 1 was in the anterior wall of the fundus.
Surgical procedures
Position and trocar insertion
The surgical procedure was performed with each patient in the herringbone position under endotracheal general anesthesia. Antibiotic prophylaxis (2 g of ceftriaxone intravenously) was given 30 minutes before the operation. The umbilical trocar (10 mm) was placed as the abdominal video-laparoscope and the 5 mm abdominal assisted trocar was placed in the upper right abdomen. The other trocar (10 mm) was used as the gastric video-laparoscope and was placed in the upper left abdomen. The remaining two gastric assisted trocars (5 mm and 12 mm) were placed in the upper two sides (Fig. 1). The surgeon was located on the left side of the patient.

The abdominal pressure was maintained at 12 mmHg after all the trocars were placed. A coagulation hook was then used to cut open the seromuscular layer at three corresponding positions in the anterior wall of the stomach. The mucosa layer was retained and the obvious submucosal vessels were coagulated to reduce bleeding. There were two gastric trocars placed in the gastric wall from the left side, one by one using the abdominal video-laparoscope. The air valve of the abdominal video-laparoscope trocar was opened to preserve the gastric cavity pressure of 8–10 mmHg.
The laparoscopic instruments were placed (Fig. 1) and a coagulation hook was used to indicate the circumferential margin (Fig. 2). The cardia submucosal tumor was resected by coagulation hook (Fig. 2) to protect the integrity of the cardia (Fig. 3). The resected tumor was removed using a disposable Endo-Pouch by the left 10-12 mm trocar (Fig. 4). Then, 3-0 V-Loc™ 90 barbed sutures (Covidien, Mansfield, MA) were used to continuously suture the defect of the gastric mucosa and gastric wall and assure complete hemostasis.

The close relationship between the GSMTs and cardia
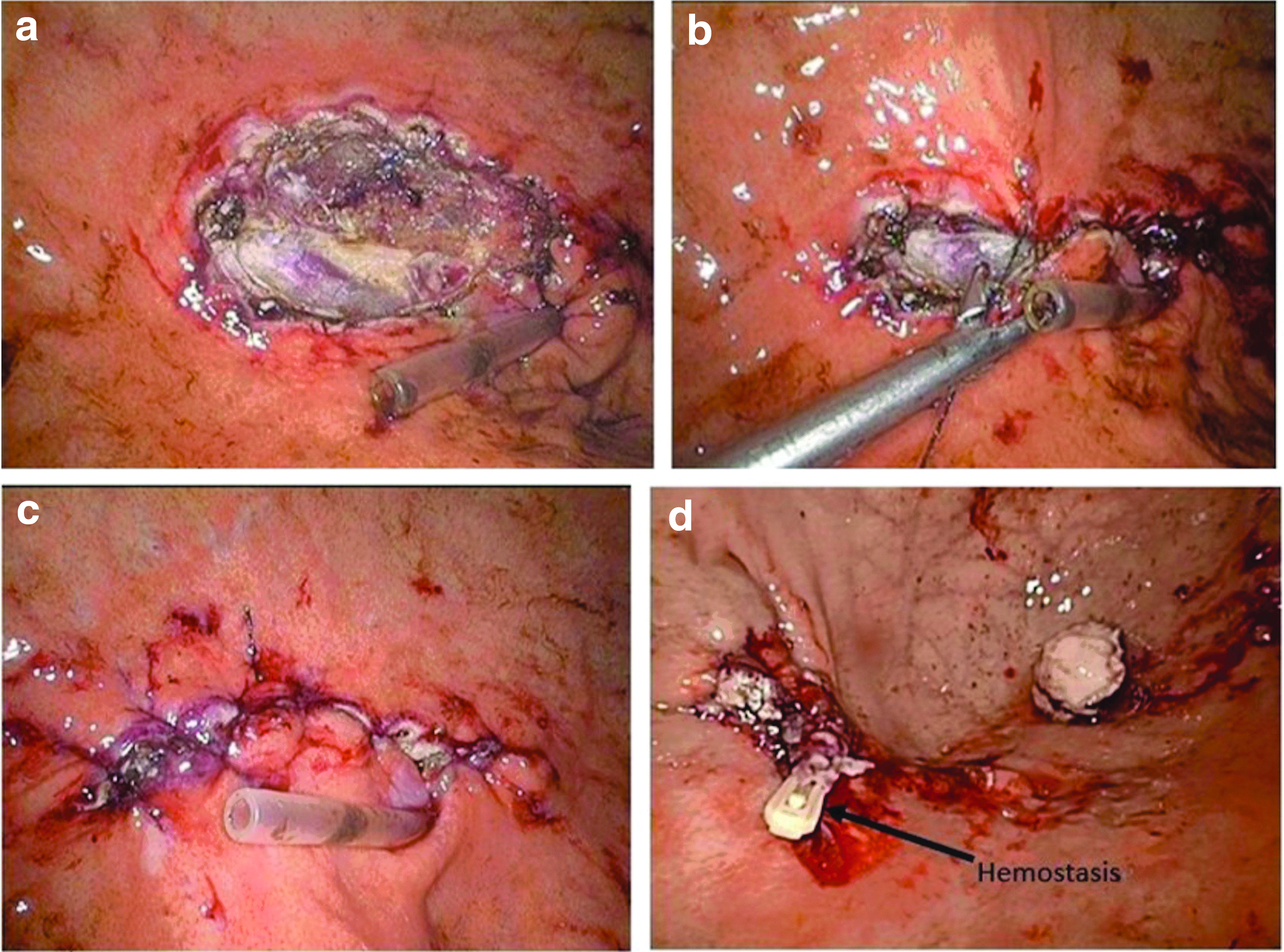
After the tumor was resected, the surgical wound showed complete resection
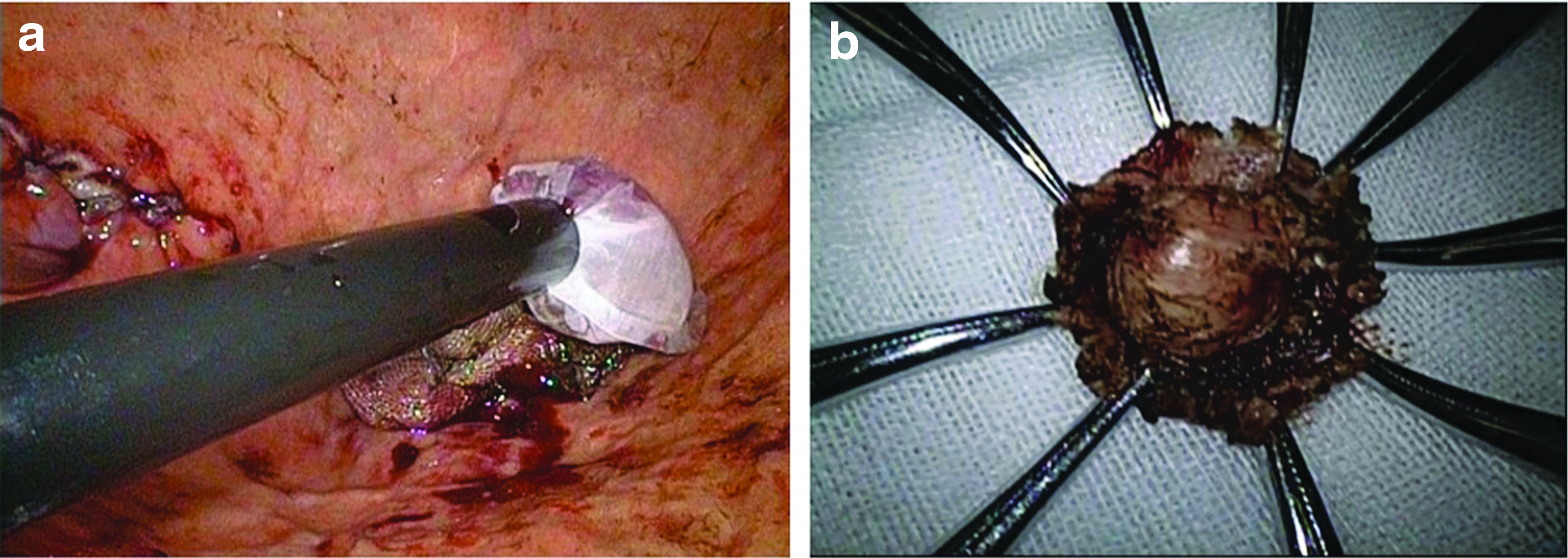
The specimen was removed using a disposable specimen bag
Outcomes
From August 2014 to June 2016, all 12 patients with CEGSMTs were successfully treated with T-LIGS and no patient was converted to open surgery. The specimens were completed and encapsulated. The following pathologic diagnoses were observed (Tables 1 and 2): gastric intestinal stromal tumors (n = 8), leiomyomas (n = 3), and G1 neuroendocrine tumor (n = 1). The operative times ranged from 56 to 108 minutes and the blood loss was 5–70 mL. The tumor distance from the cardia dentate line was 12–24 mm. The tumor diameters ranged from 17 to 28 mm, and the tumor margin was 9–15 mm. The patient fasting time was 2–4 days, and the drainage tube indwelling time was 0–3 days. The patient discharge time was 3–6 days. During the perioperative period, 1 patient experienced infection of the trocar port. The follow-up examinations revealed no recurrences, dysphagia, acid reflux, or other digestive symptoms.
GIST, gastrointestinal stromal tumor.
Discussion
Surgical resection is the gold standard for CEGSMTs and techniques for GSMT resections have shifted from open surgery to laparoscopic and endoscopic approaches and from gastrectomy to local resection. Recent advances in laparoscopic techniques and optimization of endoscopic systems have improved the safety and feasibility of laparoscopic surgery and endoscopic resections.2,3,9–11 However, due to the special location of these tumors, only a limited number of physicians have mastered the highly difficult techniques required to resect CEGSMTs by endoscope. In addition, this surgical strategy is limited in most developed countries and only a few major hospitals offer the surgery in developing countries. Thus, a new easy and feasible exploration of LIGS for local resection is needed to avoid proximal partial gastrectomy. In 1995, Ohashi 8 reported the first LIGS to treat early gastric cancer and achieved satisfactory results. Simultaneously, other clinical procedures similar to LIGS have also been reported12–17 with good clinical results. The majority of these reports show tumors located in the body of the stomach. Therefore, we summarized our experience in treating CEGSMTs with T-LIGS.
Designing the puncture positions is the first crucial step in the procedure. A proper design can prevent the instruments from interfering with each other and should provide a full view of the gastric cavity. When locating the puncture hole in the stomach, the gastric body should be pulled down. The left gastric trocar should be close to the greater curvature and the right trocar should be located close to the lesser curvature. The position of the gastric video-laparoscope trocar is slightly lower than the operating trocars. It is also important to coagulate the vessels of the lesser and greater curvature corresponding to the gastric holes. Only the seromuscular layer is cut, and the obvious submucosal vessels are coagulated before placing the trocar into the stomach directly. This avoids making the hole oversized. The gastric trocars should be placed from the left side one by one. The abdominal assisted trocar can grasp the gastric wall and aid in placing the gastric trocars, which will avoid damaging the mucosa of the posterior gastric wall. The 3-0 V-Loc 90 barbed suture is very useful to suture the defect of the gastric mucosa and gastric wall continuously. This approach is reliable and time-saving. It is not necessary to block the duodenum 8 because when the air valve of the abdominal video-laparoscopic trocar is opened, any overgassing of the gastric cavity will flow into the abdominal cavity and out of the body. The gap between the gastric wall and the trocars is small so the pressure of the gastric cavity can be maintained at 8–10 mmHg. It is important to completely exhaust the excess CO2 to reduce any harm. Preoperative endoscopic ultrasonography and CT scans are both necessary and cannot be substituted for each other. These tests help identify tumors embedded in the submucosa or muscular layer such as leiomyoma.
In our study, the lack of experience in the early phase led to increased operation time and intraoperative blood loss. However, the accumulation of experience led to satisfactory control of blood loss and surgical time. Our overall results were similar to the results of prior studies.8,11,14 In addition, the complication rate was lower in all patients compared to other studies.13,16 All the cases were confirmed by postoperative pathology and were completely resected. Thus, from the surgeon's point of view, the procedure is safe and feasible for CEGSMTs.
In contrast to the study by Li et al., 18 we did not need to open the gastric wall to expose the tumors and avoided the spread of the malignant tumor. Furthermore, compared to the study by Ojima et al., 19 we did not need the help of an endoscope and this decreased operating techniques. This difference is especially valuable in county hospitals. Previous research published 20 used cuffed trocars, and we did not require these instruments. This is useful because it is difficult to obtain these instruments in most developing countries and county hospitals. We used a coagulation hook to indicate the circumferential margin. The hook may more accurately confirm the margin relative to using the linear stapler to resect the tumors. 21 In our center, we also explored the single-point procedure. However, this required a 3 cm incision in the abdomen and was difficult in obese patients.
The limitations of our study include the single-center design, small sample size, single arm test, and retrospective nature. However, there is currently no clinical long-term evaluation of the procedure. Our research is only an analysis of short-term results. Therefore, we hope that there will be a multicenter, large sample, and prospective study to support our findings. Future studies should also evaluate the long-term efficacy.
Conclusion
Our data indicate the T-LIGS surgical approach is safe and feasible for the treatment of CEGSMTs and only requires conventional laparoscopic instruments in developing countries and county hospitals. Future advances in surgical instruments and techniques and the promotion of endoscopic technology may replace this surgery, but our findings show that it is currently a safe and effective option.
Footnotes
Acknowledgment
This research was supported by Guangdong General Hospital, Guangzhou, China.
Disclosure Statement
All authors have no conflicts of interest or financial ties to disclose.