
Abstract
Abstract
Background:
There are various methods to place a gastrostomy tube. We report a laparoscopic method to place a standard percutaneous endoscopic gastrostomy (PEG) tube without the use of endoscopy.
Methods:
Laparoscopic magnet-assisted PEG placement was carried out using an orogastric tube attached with a magnet that is used to retrieve the PEG wire that has been percutaneously placed into the stomach.
Results:
Four pediatric patients (mean age 31 months) underwent a PEG tube placement using the laparoscopic magnet-assisted PEG tube insertion technique during 2017. There were no immediate and long-term tube placement complications. Retrieval of the PEG wire using the magnet-tipped orogastric tube was successful in all patients.
Conclusion:
Laparoscopic magnet-assisted PEG tube placement allows precise PEG tube placement without the need for endoscopy.
Introduction
T
One drawback to the laparoscopy-endoscopy techniques is the need for simultaneous endoscopy and laparoscopy. As provider time and operating room availability are limited, hybrid techniques can be cumbersome to coordinate. The endoscopic portion can also be difficult in certain populations such as small children or patients with difficult neck anatomy. We previously reported a novel and safe hybrid technique named “laparoscopically assisted antegrade percutaneous endoscopic gastrostomy.” 6 We have modified the approach to negate the need for endoscopic equipment or an endoscopist. In this report, we describe our early experience with a laparoscopic magnet-assisted PEG placement, which uses an orogastric tube attached with a magnet that is used to retrieve the wire that has been percutaneously placed into the stomach with the aid of a laparoscope.
Materials and Methods
A standard PEG kit is opened in a sterile back table (16 Fr CORFLO-MAX Peg Kit; CORPAK MedSystems, Inc., Buffalo Grove, IL). After general anesthesia and intubation, a 5-mm port is placed through the umbilicus of a supine patient. The abdomen is insufflated to 12 mm Hg pressure with carbon dioxide gas, and a skin incision is made on the abdomen at the chosen PEG site. A Maryland grasper is passed into the abdomen through the skin incision, which is used to grasp the stomach near the greater curvature where the PEG tube is expected to exit. With the stomach pulled toward the abdominal wall, a suture with a large needle is used as a percutaneously placed U-stitch for stomach traction at two places near the Maryland grasper. Once the U-stitches are placed, Maryland grasper is removed, and through the same opening, a 14-gauge angiocath is used to puncture the stomach. The needle within the angiocath is removed, and the PEG wire is passed into the stomach via the angiocath. A sufficient amount of the wire is placed into the stomach such that the wire will coil within the stomach. An orogastric tube fitted with a ¼″ diameter and ½″ long cylindrical neodymium magnet (Product D48-N52; www.kjmagnetics.com) is passed from the mouth into the stomach (Fig. 1). The ferromagnetic PEG wire within the stomach automatically attaches itself to the magnet. The orogastric tube is slowly pulled out through the mouth dragging the wire with it. When the wire attaches to the magnet, there is a subtle sensation that one can feel at the end of the orogastric tube with a slight movement of the wire at the skin level. A portable C-arm fluoroscope can also be used to help visualize and attach the magnet to the wire.
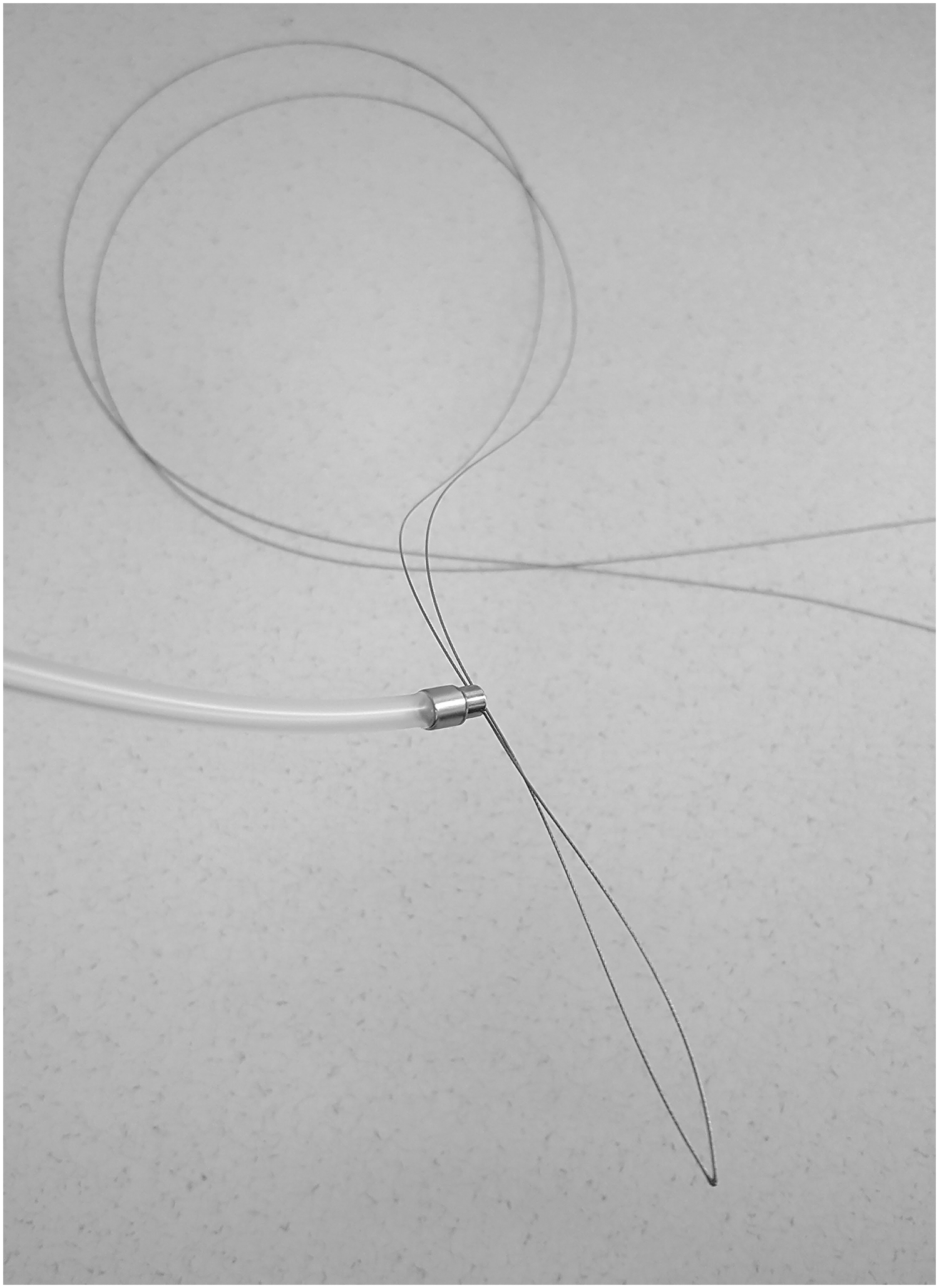
An orogastric tube fitted with a 5-mm-diameter cylindrical neodymium magnet. The PEG wire attaches to the magnet without difficulty. PEG, percutaneous endoscopic gastrostomy.
Once the wire is retrieved at the mouth, the PEG tube is connected to the wire, and the PEG tube is tugged into the stomach by pulling on the wire at the abdominal wall side. Once the PEG tube is placed within the stomach, the U-stitches are removed. The schematic of the technique is shown in Figure 2.

Informed written consent was obtained from the parents of pediatric patients for the laparoscopic magnet-assisted PEG tube placement. Institutional review board approval was obtained for the study.
Results
Four pediatric patients underwent a PEG tube placement using the laparoscopic magnet-assisted PEG tube insertion technique during 2017. The parents of these four patients preferred to have a PEG tube placed rather than a short gastrostomy tube such as Mini One Balloon Button (Applied Medical Technology, Inc., Brecksville, OH). The reasons included perceived sturdiness of the tube and non-necessity to change the tube frequently. The mean age of the patients was 31 months (range 15 months to 5 years). The main reason for gastrostomy placement was feeding difficulties due to each patient's underlying conditions. There were no immediate tube placement complications such as stomach or esophageal injury from the magnet-tipped orogastric tube. No patients needed endoscopy. No long-term gastrostomy tube placement complications such as dislodgement, gastric outlet obstruction, and other viscus injury were observed. The cost of the magnet was $0.99.
Discussion
In this case series, we described our early experience with a new hybrid PEG tube placement technique that eliminates the need for endoscopy. There are many techniques for laparoscopic and endoscopic placement of gastrostomy tubes, and each has its relative risks and benefits. In general, laparoscopic techniques have been shown to be safer as they allow for a direct visualization of intra-abdominal organs, unlike the traditional PEG technique.4,5 When hybridized, as in LAPEG or LEGT techniques, the benefits of each method complement one another to minimize the risks that are inherent in the two approaches when used independently.7–9 These hybrid techniques have been shown to be safer.2,3 Laparoscopic short gastrostomy tube placement technique utilizes stay sutures or T-fasteners and water-filled balloon gastrostomy tube to maintain the stomach in a fixed position and do not need endoscopy for placement purposes.10,11 Similar to the short gastrostomy tube placement, in our technique, a PEG tube can be easily placed into the stomach without endoscopic equipment.
Although safer, one disadvantage of the LAPEG/LEGT technique is the need for endoscopy. When surgeons alone perform LAPEG or LEGT, the endoscopic portion can be difficult, particularly in smaller pediatric patients or those with difficult anatomy. When an endoscopist participates in the procedure with the surgeon, coordination between the two physicians is necessary. In our procedure, the passage of magnet-tipped orogastric tube is still required; this was performed by attending anesthesiologists who are familiar with placing orogastric and nasogastric tubes during surgical procedures.
Further experiences are needed to fully evaluate the risks and benefits of our magnet-tipped orogastric tube. Thus far, we have not encountered any complications or procedural difficulties. Although we have used this technique only on pediatric patients, we believe this technique is safe to use in all age groups and has the potential to reduce operative time and cost without lowering patient safety.
Footnotes
Disclosure Statement
No competing financial interests exist.