
Abstract
Abstract
Purpose:
Laparoscopic Kasai portoenterostomy (LKP) remains controversial in the management of infants with biliary atresia (BA). There are no data reporting the 10-year native liver survival rate after LKP. The study aims to present the 10-year native liver survival rate after LKP and complications in native liver survivors after Kasai portoenterostomy (KP).
Methods:
A retrospective review was conducted for 31 consecutive infants with BA who underwent KP by day 75 of life in our institute from January 1993 to December 2007. The demographics and outcomes of patients after LKP and open KP (OKP) were compared.
Results:
Eleven patients underwent LKP and 20 patients underwent OKP. No statistical difference was observed in the age at operation and the preoperative bilirubin level. The operative time for LKP was significantly longer than that for OKP (mean 314.5 minutes versus 271.5 minutes, P = .03). The 10-year native liver survival rate was 45% (5/11) after LKP and was 85% (17/20) after OKP (P = .03). Forty percent (2/5) of the native liver survivors in the LKP and 71% (12/17) in the OKP developed complications within 10 years after KP (P = .23).
Conclusions:
The 10-year native liver survival rate in patients who underwent LKP by 75 days of life was 45%. With superior 10-year liver survival rate and comparable complication rate after OKP, OKP is still the treatment of choice for BA in our institute.
Introduction
K
Regardless of the approach to KP, native liver survivors developed complications as a result of the progressive liver disease. 7 Complications including cholangitis, gastrointestinal bleeding, and portal hypertension developed in 60%–100% of long-term native liver survivors. 7
The 10-year native liver survival and long-term complications in native liver survivors after LKP are never reported in the literature. This study designed to evaluate the 10-year native survival rate after KP and to compare the 10-year complication rates in native liver survivors between LKP and OKP in our center.
Materials and Methods
From January 1993 to December 2007, 36 infants with BA underwent KP. This review only studied patients who underwent KP by 75 days of life. All patients were operated by laparoscopic approach from 2002 to 2006 according to our department policy. OKP was performed before 2002 and after 2006.8,9 The age and the sex of the patients, the bilirubin levels before the operation, and operative time were reviewed. The clearance of jaundice was defined as the total bilirubin <20 μmol/L. The clearance rate of jaundice at 6 months after KP, the native liver survival rate at 5 and 10 years, and the jaundice-free 10-year native liver survival after KP were reviewed.
Complications including cholangitis, variceal bleeding, hypersplenism, and intestinal obstruction developed within 10 years after KP in native liver survivors were studied. Hypersplenism was defined as splenomegaly with thrombocytopenia (platelet <100 × 10 9 /L). The outcome of patients who underwent LKP and OKP was compared. Ethical approval was obtained from our institutional review board.
The techniques of LKP and OKP were previously described.4,8 In LKP, a subumbilical 5 mm camera port was inserted. Two 5 mm ports and one 3 mm port were inserted at left and right upper quadrants of the abdomen. A Nathanson liver retractor was inserted at the epigastric region. In OKP, a right subcostal incision was made, and the liver was delivered outside the abdominal cavity after lysis of the triangular ligaments. The dissection of the fibrous cone was extended over the bifurcation of the portal vein. The fibrous cone was dissected at the level flush with the liver capsule. The use of electrocautery in hemostasis around the portal plate was minimal, and the portal vein tributaries were ligated between ligatures. The Roux-en-Y jejunal loop and portoenterostomy were performed in a similar fashion in both groups. In laparoscopic group, the Roux loop was fashioned extracorporeally through an enlarged umbilical wound.
Statistical methods
Statistical analysis was accomplished using the SPSS program for Windows 24.0 (SPSS, Chicago, IL). The t-test was used to compare the continuous data. Chi-square test was used to compare the categorical data. The survival curve was established according to the Kaplan–Meier method and compared by the log-rank test. P < .05 was considered statistically significant.
Results
This study included 11 infants who underwent LKP and 20 infants who underwent OKP. All had type III BA and were nonsyndromic. The demographics of the patients and the operative time are listed in Table 1.
Demographics, Preoperative Bilirubin, and Operative Time
P < .05 was considered statistically significant.
LKP, laparoscopic Kasai portoenterostomy, OKP, open Kasai portoenterostomy.
At 6 months after the KP, the clearance rate of jaundice in LKP was 45% (5/11), and the rate was 80% (16/20) in the OKP (P = .06). The 5- and 10-year native liver survival rate was 45% (5/11) in LKP and was 85% (17/20) in the OKP (P = .03; Fig. 1 and Table 2). Ten patients underwent liver transplantation and 1 patient who remained jaundice after KP defaulted follow-up. The jaundice-free 10-year native liver survival rate was 45% (5/11) in LKP and was 70% (14/20) in the OKP (P = .17; Table 2). The bilirubin levels were 29, 30, and 39 μmol/L in 3 jaundice patients, respectively, at 10 years after the operation.
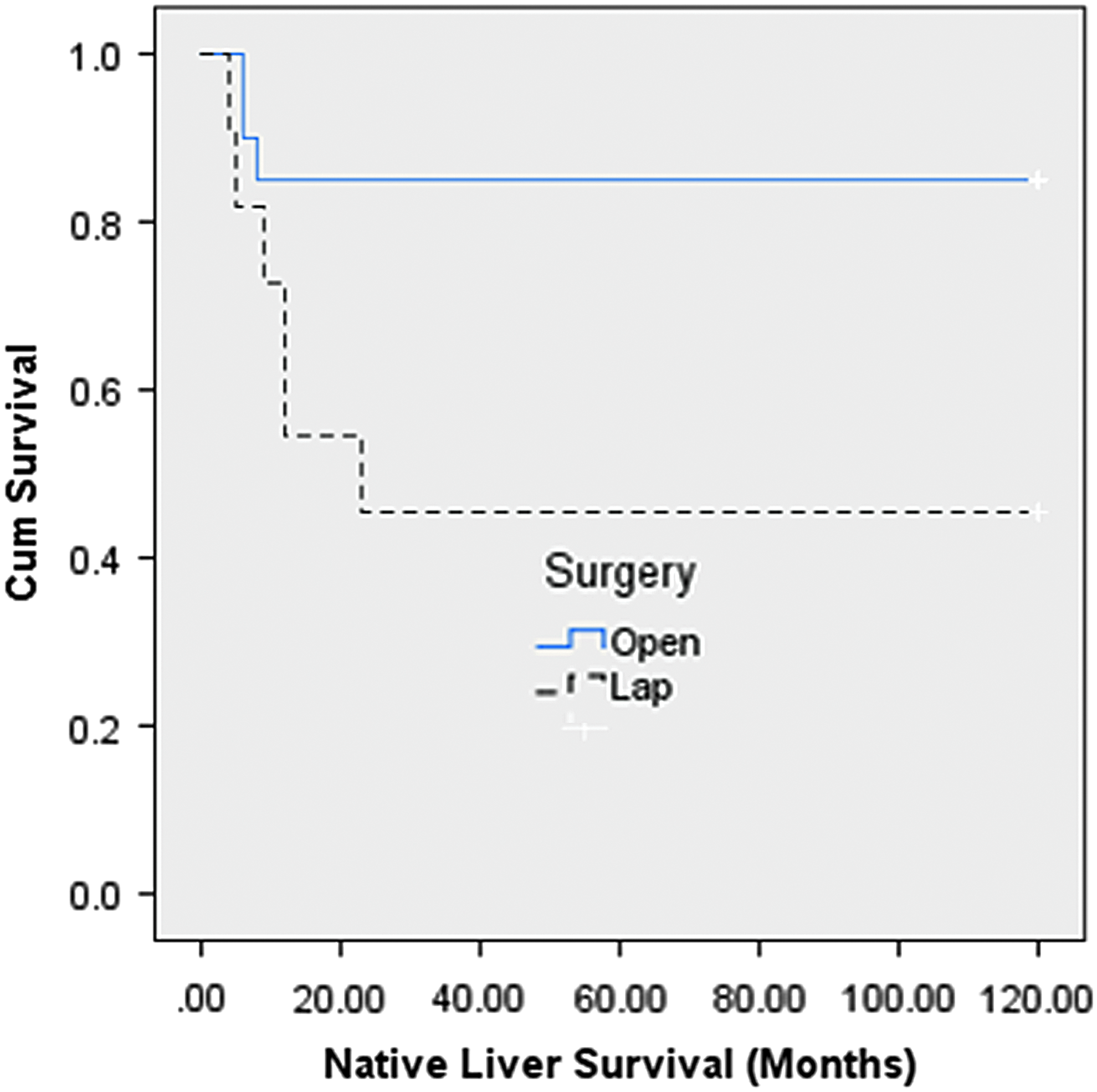
Ten-year native liver survival rate after Kasai portoenterostomy.
Clearance of Jaundice and Native Liver Survival After Kasai Portoenterostomy
P < .05 was considered statistically significant.
The clearance of jaundice or jaundice free was defined as the total bilirubin <20 μmol/L.
KP, Kasai portoenterostomy; LKP, laparoscopic Kasai portoenterostomy; OKP, open Kasai portoenterostomy.
Within 10 years after KP, 59% (13/22) of native liver survivors developed complications. The overall complication rate was 40% (2/5) in LKP and 71% (12/17) in OKP (P = .23) (Table 3). One patient after LKP and 4 patients after OKP had history of esophageal variceal bleeding requiring endoscopic hemostasis. No patients after LKP and 4 patients after OKP had hypersplenism. Approximately 40% of patients in each group had history of cholangitis. Two patients developed intestinal obstruction after OKP. One patient was managed conservatively, and the other patient required laparotomy and adhesiolysis.
Complications in Native Liver Survivors
P < .05 was considered statistically significant.
LKP, laparoscopic Kasai portoenterostomy; OKP, open Kasai portoenterostomy.
Discussion
This is the first report in the literature on the 10-year native survival rate after LKP. The reported 10-year native liver survival rate ranged from 31% to 60% after OKP.10–13 Our LKP result was comparable with the national and consortium statistics. A drop of 6%–9% in native liver survival rate was observed between 5 and 10 years after KP in large-scale studies. 13 In this study, all native liver survivors at 5 years after KP did not require liver transplantation in the following 5 years. In our center, parents of native liver survivors were counseled and educated on the risk of cholangitis. They were told to seek medical advice immediately if the patients developed fever or passed pale stools. To avoid delay in treatment, we did start board-spectrum antibiotics including third- or fourth-generation cephalosporin empirically for suspect cholangitis. Our results may reflect the importance of meticulous and timely management of cholangitis.
Although LKP was reported in the literature for over 15 years, there were only few reports published.2–5,8,9,14–18 Our center reported the jaundice clearance rate, 2-year native liver survival and 5-year native liver survival were 50% after LKP. 8 However, the outcomes of OKP were superior before the adoption of laparoscopic technique in 2002 and after we reintroduced OKP in 2007.4,9 A meta-analysis of LKP and OKP also reported that the rate of 2-year survival with native liver was significantly higher after OKP. 19 The inferior outcome after LKP was always attributed to the harmful effect of carbon dioxide pneumoperitoneum, inadequate exposure of the portal plate, diathermy injury to the bile ductules at porta, and learning curve of laparoscopic procedure in the literature.5,20 The meta-analysis concluded that LKP could not replace OKP, and OKP remains the “gold standard” for the treatment of BA. 19 In this study, the longer operation time for LKP reflected the learning curve in complex laparoscopic surgery. The longer operation may lead to the higher risk of damage to the liver cell as a result of the detrimental effects of a prolonged high-pressure carbon dioxide pneumoperitoneum.
Recently, there were increasing studies reporting a comparable or even more favorable outcome after LKP since 2015.21–26 A randomized controlled trial on LKP and OKP was performed in the Capital Institute of Pediatrics in Beijing. 21 The median follow-up was ∼17 months. They reported that the short-term and mid-term outcomes were comparable between the two groups. The jaundice clearance rate was 43% in LKP and 51% in OKP. Their result obtained for the LKP was similar to that of our study. 9 In Juntendo University School of Medicine, LKP had been performed since 2009.22–24 The authors emphasized the level of transection at the porta to be narrow using Kasai's original techniques. They could achieve a high jaundice clearance rate of 94%. The native liver survival rate at 2 years was 73.7%.
Shenzhen Children's Hospital reported a total of 80 infants who had undergone LKP from 2011 to 2015. 25 The overall jaundice clearance rate was 58%, and the overall 2-year native liver survival rate was 50%. After performing 40 LKP, the jaundice clearance rate was >75% and the 2-year native liver survival rate was >60%. The authors concluded that a surgeon is able to become more experienced after performing ∼40 LKP. Because of the rarity of BA, the learning curve is difficult to achieve in centralized centers elsewhere. In Taiwan, the 2-year native liver survival rate was 70% in 10 patients after LKP, which was comparable with 69.2% in 13 patients after open portoenterostomy. 26 Reconsideration of LKP was recommended by these centers in the management of BA.
Despite a successful KP, native liver survivors developed complications, either surgically related or associated with the progressive liver disease. 7 In this study, we only documented the complications occurred in the first 10 years after KP. Forty percent of native liver survivors after LKP and 71% of native liver survivors after OKP developed complications. There was no statistical difference in the complication rate for the two groups. Cholangitis is a well-known complication in native liver survivors. It was reported to occur in 30%–60% of patients. 26 Forty percent of native liver survivors of each group had history of cholangitis, which was comparable with international reports. 7 In our center, native liver survivors who developed cholangitis after infancy were treated successfully and remained transplant free during the study period. Complication rates related to portal hypertension including variceal bleeding and hypersplenism were also comparable in both groups. Of course, we only studied the complication within 10 years after KP. Patients after KP had life-long risk of developing complications attributed to portal hypertension. In patients with portal hypertension, a life-long follow-up is important in particular to watch out for the development of hepatopulmonary syndrome in future. 7
Open surgery carried a higher risk of postoperative intestinal obstruction. In this study, 2 patients after OKP developed intestinal obstruction. Despite the higher risk of intestinal obstruction; unlike complication related to chronic liver disease, it seldom affected the native liver survival rate. Our results suggested that the underlying reasons that account for inferior short-term outcomes in LKP may not have additional long-term impact in the development of chronic liver problem.
The best timing for KP remains controversial. It is generally accepted earlier that operation was associated with superior outcome, and the prognosis for patients aged ≥3 months is poor; however, there is no consensus whether 2 months is a critical age that can impact the prognosis. 27 Cazares et al. reported 81.3% native 3-year liver survival rate after LKP with the mean age of 67.1 days. 23 We only included infants who underwent KP by 75 days of life in this study. This age-specific cohort ensures that the age of patients was not statistically different between the two groups. The results of treatment could be correctly evaluated.
There were several limitations in this study. First, the sample size was small and the study period was long. Only 31 patients were included in this study. It reflected the rarity of BA. Despite the small case volume, our early jaundice clearance rates and, 5- and 10-year native liver survival rates were comparable with international standards even after LKP. Second, this study shared the common limitations in a retrospective cohort study. It was no doubt that with a study period of 14 years, there was heterogeneity in perioperative management, including postoperative steroid treatment and other adjuvant therapy. Whether the difference had any effect on the prognosis was unclear.
In conclusion, we have reported the first study in the literature on the 10-year native liver survival rates after LKP. The short-term and long-term native liver survival rates are superior after OKP in our center. The development of liver-related complications was not related to the initial approach to KP. Patients with early jaundice clearance after LKP had a similar clinical course to those who underwent OKP. Our center will not reintroduce LKP because of our superior outcome in the OKP. However, this study provides new information on the long-term clinical course after LKP and would be valuable in centers that advocate LKP.
Footnotes
Disclosure Statement
Drs. K.W.E.C., K.H.L., H.Y.V.W., S.Y.B.T., J.W.C.M., and Y.H.P.T. have no conflicts of interest or financial ties to disclose.