
Abstract
Abstract
Purpose:
The aim of this retrospective study is to describe our initial experience by using new simplified mattress sutures with syringe needle for congenital diaphragmatic hernia (CDH) in neonates when no posterolateral rim of diaphragm exists.
Methods:
A retrospective review of the new simplified technique in 15 cases from February 2015 to February 2018 at a single institution was performed. In the procedure, two to three primary suture sites were taken from the relative intercostal region of the body surface. Two 2-0 nonabsorbable sutures around the rib were inserted between the anterior rim of the defect and the relative rib through a syringe needle. Knot tying was made extracorporally and the knots were under the skin of intercostals space.
Results:
Among the patients, 9 were male and 6 were female. The age was 10 minutes–1 day when admitted, 10 were term newborns, and 5 were premature. The mean operative time was 37.5 minutes (range, 25–60 minutes) for each CDH repair. No cases required conversion to open surgery, blood loss was minimal. The mean follow-up duration was 18.5 months (range 3–27 months), with no deaths, and no single case of recurrence.
Conclusion:
We have found this simple technique to be a useful adjunct in the thoracoscopic management of selected cases with CDH. It has the advantages of reduced operative time, simplicity, and feasibility and has the value of clinical popularization.
Introduction
Congenital diaphragmatic hernia (CDH) occurs in 1 in 2000–5000 births. 1 Traditional approaches to repair CDH included laparotomy or thoracotomy with primary or patch closure. However, the era of minimally invasive surgery has seen the application of thoracoscopic or laparoscopic techniques in the repair of congenital diaphragmatic defects.2,3 Although laparoscopic and thoracoscopic repairs have been described, management of the condition is still a challenge for pediatricians and pediatric surgeons alike. Acidosis during surgery and the higher recurrence rate are considerable risk factors, and most reports are in older infants.4,5 But intracorporeal suturing and knot tying for closure of the CDH need a long learning curve and may take a longer time, especially when no posterolateral rim of diaphragm exists. 6
We herein devised a new simplified technique by using a syringe needle for rapid thoracoscopic repair of CDH in neonates when no posterolateral rim of diaphragm exists and intracorporal suture placement difficult or even impossible. This article describes the operative technique and its outcomes, and demonstrates the advantages and feasibility of this procedure.
Materials and Methods
Fifteen consecutive neonates treated by this simplified technique during the period February 2015 to February 2018 were reviewed. Among the patients, 9 were male and 6 were female. The age was 10 minutes–1 day when admitted, 10 were term newborns, and 5 were premature. The mean weight was 2.85 kg (range 2.3–3.5 kg). All the cases were left sided. The procedures were carried out by the same surgical team and led by 1 of the coauthors (B.L.). This study was approved by the Ethics Committee of Huai'an Women and Children's Hospital (Jiangsu, China). Informed consents were obtained from all the parents preoperatively.
Surgical technique
After admission, if the baby is in hemodynamics stable condition, the operation should be performed as soon as possible. Primary repair of a CDH usually involves suture apposition of the unfused leaflets of the diaphragm. When a given diaphragmatic leaflet is nonexistent, the use of several sutures around a relative rib may still permit primary repair.
We devised a new simplified technique of sutures around a relative rib to the anterior rim of posterolateral defects by a syringe needle, knot tying was made extracorporeally, and then the simplified mattress sutures were accomplished. All the 15 neonates were subjected to thorough clinical examination and routine laboratory and radiological investigations.
After the induction of general endotracheal anesthesia, the patient was placed in the lateral decubitus position with left side of the diaphragmatic defect facing up. The surgeon was at the left of the operating table, and the display was placed on the side of the feet.
A 5-mm trocar was placed in the fourth intercostal space, at the midaxillary line by an open technique. Carbon dioxide (CO2) pneumothorax with a pressure of 6–8 mmHg was established. Through this port, a 5 mm 30° scope was used for initial visualization of the thoracic cavity and the diaphragmatic defect. A second port was placed in the fifth intercostal space, lateral to the posterior axillary line. A third port was positioned in the fifth intercostal space, below the nipple. And the two accessory trocars were inserted under direct vision.
Insufflation CO2 pneumothorax pressure was initiated at 6 mmHg. Sometimes a brief increase in insufflation pressure up to 10 mmHg often aided in the reduction of the hernial contents, especially when the spleen was difficult to reduce.
By using insufflation CO2 pneumothorax and laparoscopic instruments, the herniated contents could be reduced into the abdomen. Then the diaphragmatic defect with no posterolateral rim existence was examined.
A snip incision ∼1 mm of the skin was done at the intercostal space relative to the diaphragmatic defect for insertion of the syringe needle. A 2/0 nonabsorbable suture was mounted into the hollow of the syringe needle, with one end of the thread 1 cm ahead of the needle tip. The needle with the thread was introduced into the thoracic cavity from the snip incision of the skin and manipulated to pass through the anterior rim of the diaphragmatic defect; the thread in the thoracic cavity was clamped with grasper and was laid in the thoracic cavity, then the syringe needle was withdrawn out of the thoracic cavity. A second 2/0 nonabsorbable suture was introduced into the hollow of the syringe needle with the needle tip at the middle of the thread. The second needle with the thread was introduced around the relative rib into the thoracic cavity from the same snip incision of the skin and manipulated to pass through the anterior rim with the two ends of the thread being out of the thoracic cavity. The first thread end in the thoracic cavity was introduced into the ring of the second thread, pulled the two ends of the second thread, and then the end of the first thread was pulled out of the thoracic cavity (Fig. 1). The two ends of the first thread were tightened extracorporally to form a mattress suture and close the posterolateral diaphragmatic defect (Fig. 2); the knot was under the skin of intercostal space.

First thread was introduced into the thoracic cavity to sew the anterior rim of the defect. The end of the first thread in the thoracic cavity was introduced into the ring of the second thread, and then was pulled out of the thoracic cavity.
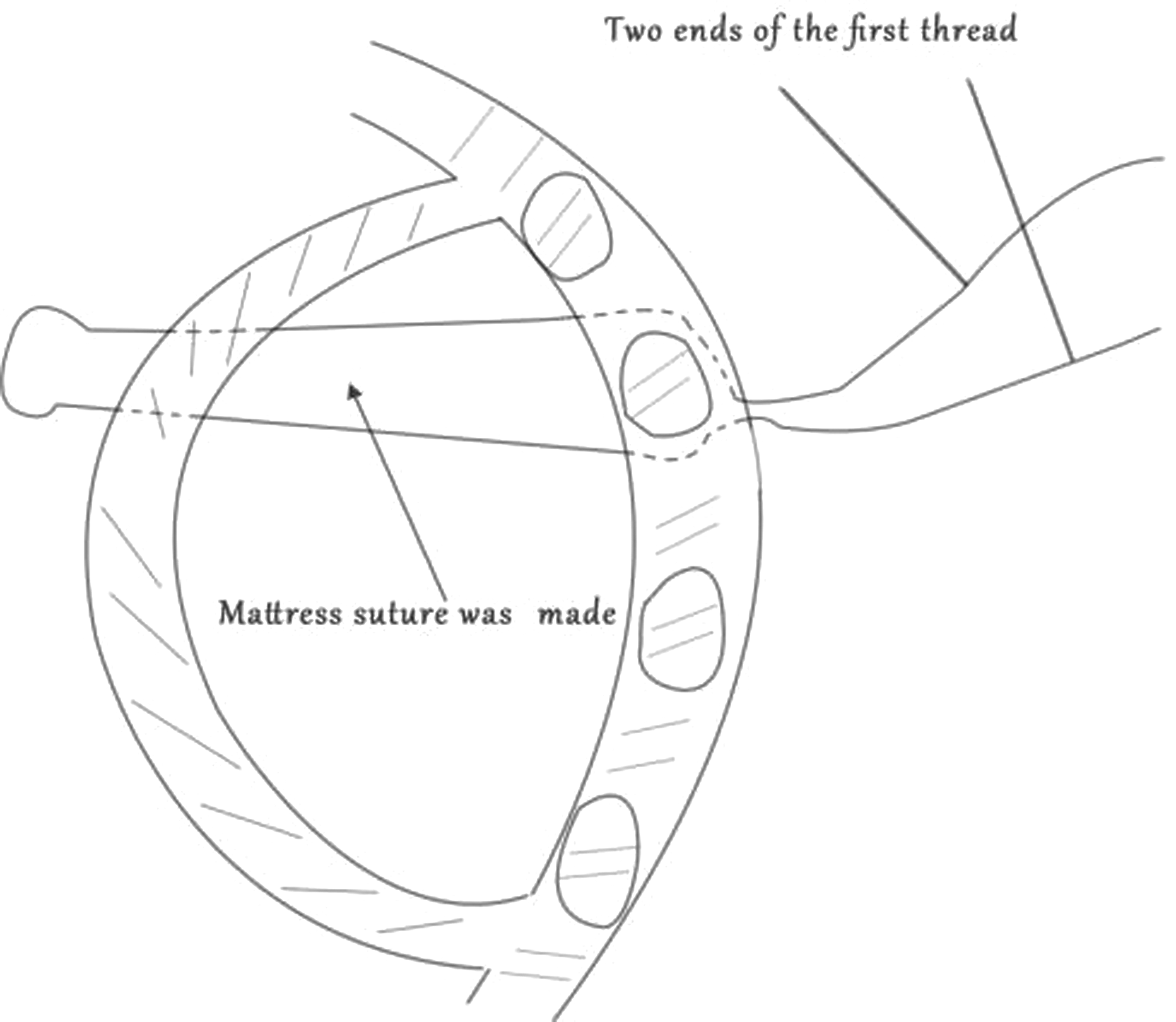
The two ends of the first thread were tightened extracorporally forming a mattress suture, closing the posterolateral diaphragmatic defect.
The amount of the mattress sutures was decided according to the necessity of the defect. Three mattress sutures could be accomplished with one spot of the skin. Most of the time, two to three spots were needed, and six to nine mattress sutures were made to close the diaphragmatic defect. All the defects were repaired primarily without the need of any patch. No chest tube was used in this group of the cases.
Results
A total of 15 selected cases with CDH were repaired successfully using this simplified technique. All the cases were left sided. Age at operation was 22.7 hours (range 10–36 hours). There was a hernial sac in 4 neonates, and the hernial sac was not excised during repairing. The contents of the hernia included intestine in 4 patients; intestine and stomach in 3 patients; intestine, omentum, colon, and spleen in 5 patients; intestine, omentum, stomach, and left lobe of liver in 3 patients.
The mean operative time was 37.5 minutes (range 25–60 minutes) for each CDH repair. There was no conversion to open surgery and no intraoperative various complications. There were no operative deaths. Blood loss during each operation was minimal, and all the patients did not require blood transfusion. No cases of this group required closure with a synthetic patch. During this period, one neonate required conversion because of a large diameter left-sided defect, with too much tension at the edge of the diaphragm. The borders of the diaphragm were torn when suturing, so the neonate was converted to open surgical repair with a synthetic patch. This case was not registered in this group. After the operation, a conventional ventilator was required for 24–72 hours in the newborns. One neonate was complicated with a small amount of pleural effusion postoperatively that healed 2 weeks later. The mean postoperative hospitalization was 6.4 days (range 4–13 days). The 15 cases were followed up for 18.5 months (range 3–27 months), with no deaths and no single case of recurrence (Table 1).
Summary of Diaphragmatic Hernias in the 15 Cases
Discussion
The first report of laparoscopic repair of CDH was published in 1995. 7 More recently, a thoracoscopic approach has been described, and has been performed in all age groups.8–10 The reported benefits of thoracoscopic approach may include faster recovery, a shorter time to discharge, lower hospital costs, fewer postoperative ventilator days and possibly less use of analgesics, and improved cosmesis. 11
Multiple studies showed a higher recurrence rate associated with thoracoscopic repair, which is also found in this study, due to learning curve, limited workspace, and the use of a patch.4,10 The posterolateral angle between the two hernia rims and the thoracic wall is always a weak point, and the defects were difficult to be closed completely in many cases.12,13 Jancelewicz et al. 10 reported that an extracorporeal posterolateral “corner” stitch might reduce recurrences.
In some neonates with CDH, a given diaphragmatic leaflet is nonexistent, and intracorporal suture placement is difficult or even impossible. 14 So how to repair the posterolateral defect completely is the key technique to reduce the recurrence rate in the future. Because a prolonged thoracoscopic approach to CDH could precipitate complications of respiratory acidosis, pulmonary hypertension, and even mortality, simplifying the operation and shortening the operation time are very important. 4 Since there is no tissue on which to anchor the sutures, the use of sutures around the rib may still permit primary repair.
In clinical practice, we devised the new simplified technique by using a syringe needle for rapid thoracoscopic repair of CDH in the neonates when no given posterolateral rim of diaphragm exists and direct closure of the two rims is impossible. 11 Simplified mattress sutures were made between the relative rib and the rim of the diaphragmatic defect with this technique. The posterolateral defect of CDH was repaired by extracorporeal suturing with thoracoscopic visualization. Extracorporeal knots could be easily done. Even some of the large defects could be closed without a patch with this simplified technique.
Most of the time we can use interrupted or even run sutures to sew the two borders of the diaphragmatic defect to repair CDH. But when the defect is large and when no posterolateral diaphragmatic rim exists, the anterior rims of the defect could be sewn to the thoracic wall by these simplified mattress sutures.
There were no intraoperative deaths or complications in our series. It shows that the simplified thoracoscopic repair is a safe procedure for CDH in newborns. The recurrence rate in our series was zero after an average follow-up of 18.5 months (range 3–27 months).
This technique offers a secure and rapid anatomical repair of the posterolateral diaphragmatic defect. It abandoned the difficult intracorporeal suturing and knot tying when no posterolateral rim of diaphragm exists, did not need a long learning curve, and without expensive instruments. We think it is an effective technique for closure of CDH in children and is worth introducing.
Footnotes
Authors Contributions
B.L. and S.-T.L. collected patients' records, contributed to literature search, drafted the article, and performed the review of the literature.
Acknowledgment
The authors thank Dr. Long Li, Capital Institute of Pediatrics for direction of this technique.
Disclosure Statement
No competing financial interests exist.