
Abstract
Abstract
Obesity is a worldwide increasing concern, and its prevalence has risen rapidly over the past several decades. Since nonsurgical treatment for weight loss in morbidly obese patients has poor long-term outcomes, bariatric surgery has gained acceptance and popularity in the last years. The laparoscopic Roux-en-Y gastric bypass has proved to be safe and effective, with successful long-term outcomes in morbidly obese patients. Key elements for the success of the operation are careful patient selection, a comprehensive preoperative evaluation, and a properly executed operation that respects the key technical elements.
Introduction
O
The first gastric bypass was introduced in 1967 by Edward E. Mason and Chikashi Ito in the University of Iowa. 5 Initially, it consisted of a horizontal gastric transection with a loop ileostomy. The technique was then optimized to smaller gastric pouches, and due to severe bile reflux, the reconstruction shifted to a Roux-en-Y loop. 6 Through the creation of a small gastric pouch and a 100–150 cm Roux limb, the procedure gains both a restrictive and a malabsorptive component. In 1994, Alan C. Wittgrove and colleagues performed the first laparoscopic Roux-en-Y gastric bypass (RYGB) in San Diego, California. 7 The laparoscopic RYGB has proved to be safe and effective, with successful long-term outcomes in morbidly obese patients.8–11
Key elements for the success of the operation are careful patient selection, a comprehensive preoperative evaluation, and a properly executed operation.
Patient Selection
The diagnosis of obesity should not be made based on body mass index (BMI) only. The BMI is a measure of body size, and obesity should be defined as a condition, in which excess abnormal body fat impairs health.
12
However, as the BMI correlates well with total body fat on a population basis and has utility in tracking populations,13,14 we can use the BMI to classify obesity in different types:
Class I obesity: BMI between 30 and 34.9 kg/m2 Class II obesity: BMI between 35 and 39.9 kg/m2 Class III obesity (morbid obesity): BMI over 40 kg/m2
According to the current criteria, the National Institute of Health guidelines states that to be considered for bariatric surgery, patients must have a BMI of 35–39.9 with an obesity-related comorbid condition (type 2 diabetes, hypertension, sleep apnea, nonalcoholic fatty liver disease, osteoarthritis, lipid abnormalities, gastrointestinal disorders, or heart disease) or a BMI ≥40 with or without a comorbidity. In addition, patients must have failed nonsurgical management of their morbid obesity, including diet, exercise, medications, and behavior modification.15,16
Preoperative Work-Up
A multidisciplinary approach during the preoperative evaluation is critical. The dietitian will be in charge of the nutritional assessment and preoperative weight loss efforts. In contrast with purely restrictive procedures, a more extensive perioperative nutritional evaluation is required for RYGB because of its malabsorptive component.17,18 A comprehensive evaluation by a psychologist or behavioral therapist is recommended to identify risk factors that may affect optimal surgical outcomes and weight loss goals. To maintain weight loss, individuals must adhere to behaviors that counteract physiological adaptations favoring weight regain. 19 In addition, the psychological evaluation will determine the quality and extent of social support available to the patient. 20
The medical evaluation should include laboratory tests (electrolyte panel and comprehensive metabolic panel) as well as the review of the cardiovascular, pulmonary, and gastrointestinal systems.21–23 The accurate diagnosis of comorbid conditions is critical to establishing individual patient goals and expectations.
The preoperative gastrointestinal imaging should include an abdominal ultrasound and an esophagogastroduodenoscopy (EGD). The ultrasound should be performed for the detection of biliary tract pathology because obese patients have a high incidence of cholelithiasis 24 and for assessing the presence of liver steatosis, fibrosis, or nonalcoholic steatohepatitis. 25 The EGD can help detecting gastrointestinal disorders associated with obesity (e.g., gastric or duodenal ulcers, gastroesophageal reflux, and/or Barrett's esophagus,) and rules out malignancy of the stomach before gastric bypass.26,27 The latter is particularly important because the remnant stomach will no longer be accessible to endoscopic surveillance.
Overall, the multidisciplinary workup along with the adequate medical evaluation and gastrointestinal imaging will help assessing the risks and benefits of the procedure.
Preoperative Weight Loss
The need for preoperative weight loss before the laparoscopic RYGB is a controversial topic. Previous studies have shown that the preoperative weight loss is not a reliable predictor of postoperative weight loss.28,29 In our experience, however, we have noticed that the preoperative weight loss reduces significantly the amount of abdominal fat and liver volume, which help performing the operation faster and safer. Therefore, a preoperative weight loss of 10% is a prerequisite to undergo bariatric surgery in our institution. A liquid low-energy formula diet for 1 or 2 weeks before the procedure often helps achieving this goal.
Surgical Technique
Position of the patient
After induction of general endotracheal anesthesia, the patient is positioned supine in low lithotomy position with the lower extremities extended on stirrups with pneumatic compression stockings and knees flexed 20°–30°. Both arms are left abducted and secured on a board with adequate padding. The surgeon stands on the patient's right side, and the first and second assistant on the patient's left side and between the legs, respectively (Fig. 1).
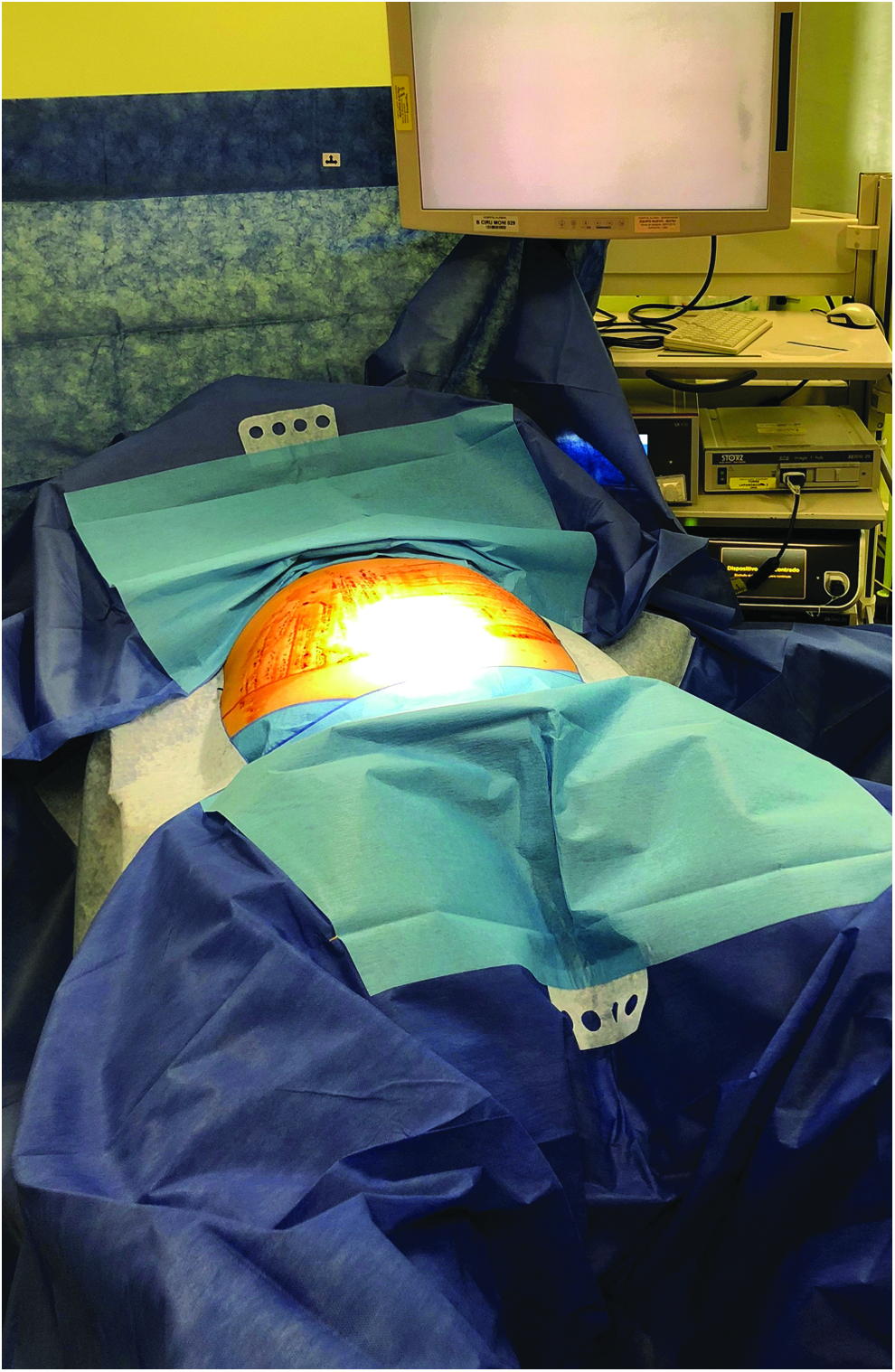
Positioning of the patient.
Troubleshooting
Deep vein thrombosis (DVT) and venous thromboembolism remain the important causes of postoperative morbidity in patients undergoing bariatric surgery. Besides the inherent risk for DVT of obese patients, the increased abdominal pressure secondary to the pneumoperitoneum and the steep Trendelenburg position decrease venous return and further increase the risk for DVT. Therefore, pneumatic compression stockings are strongly encouraged.
Pneumoperitoneum and trocar placement
A Veress needle is placed in a left subcostal location through Palmer's point (3 cm below the left costal margin in the mid-clavicular line). Pneumoperitoneum is established using carbon dioxide to a maximum pressure of 12 mmHg. We use a six-port technique. A 12 mm optical port is inserted 10–12 cm below the xiphoid process and 2–3 cm to the left of midline. The remaining five ports are then placed as shown in Figure 2.

Port placement.
Troubleshooting
Nonbladed trocars are preferred to reduce the rate of herniation. Care must be taken not to place the ports too low, which can make the operation more challenging. The liver can be simply retracted with a locking Allis grasper clamp or Endo Clinch placed through the subxiphoid 5 mm port and secured to the right crus just anterior to the gastroesophageal junction (GEJ).
Gastric pouch creation
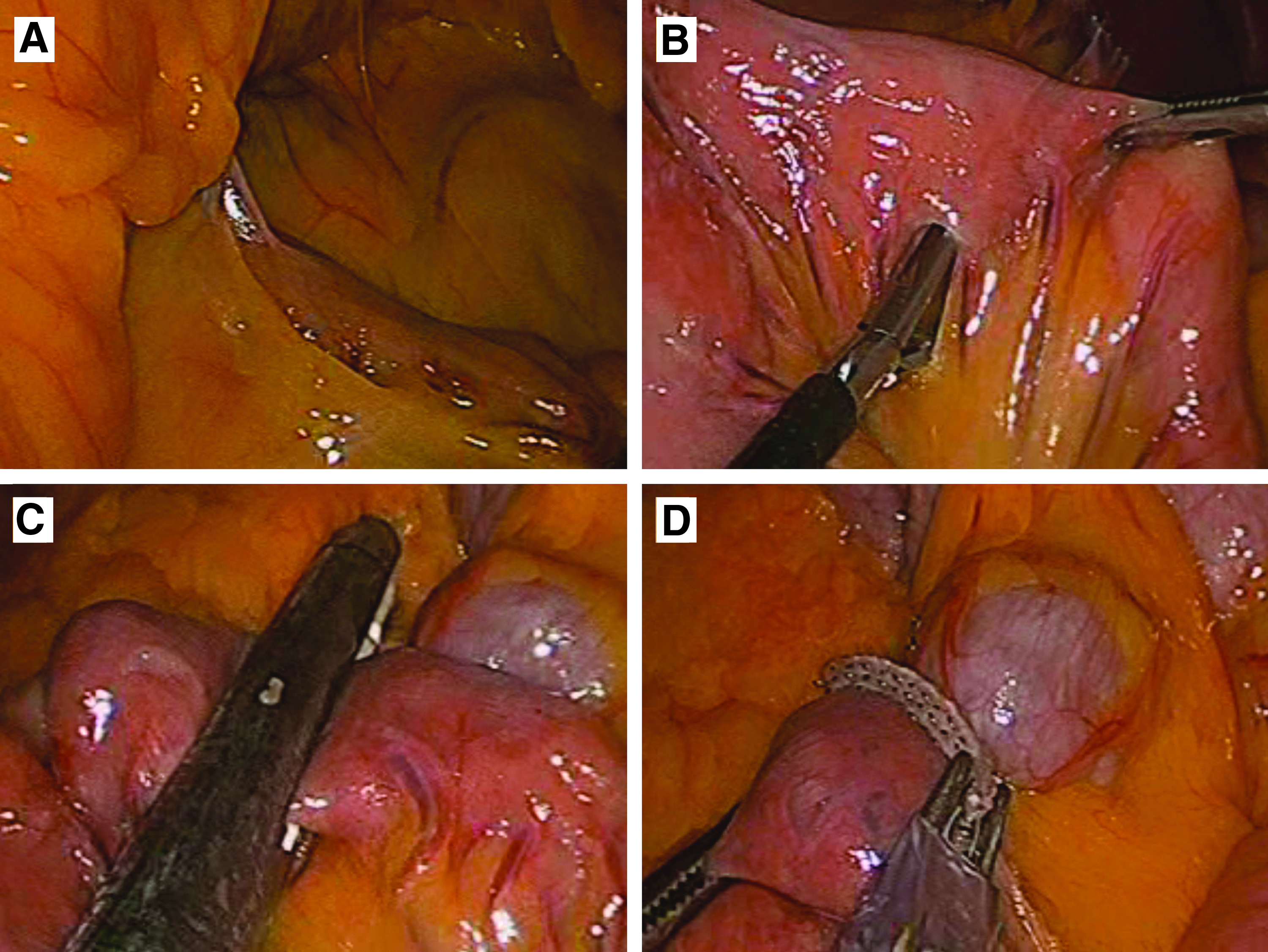
We begin the operation by removing the GEJ fat pad with ultrasonic shears. The angle of His is then exposed and dissected up to the base of the left crus (Fig. 3A). The gastrohepatic ligament is incised between the second and third branch of the left gastric artery and the lesser sac is entered (Fig. 3B). The gastric section is performed horizontally using 40–50 mm of a 60 mm blue load linear stapler (Fig. 3C). A 36-Fr gastric lavage tube is advanced by the anesthesiologist to abut this horizontal staple line. The gastric section is then completed with additional firings of 60 mm blue loads in a vertical direction toward the previously dissected angle of His (Fig. 3D). The length of the pouch should be ∼6–8 cm. The gastric remnant staple line is inspected and reinforced with an absorbable running suture (e.g., polyglactin 2.0) to prevent bleeding.

Gastric pouch creation.
Troubleshooting
In most patients, the lesser sac is free of adhesions, but patients with history of pancreatitis or gallbladder disease may have significant adhesions. During the creation of the gastric tunnel, care should be taken to avoid injury of the splenic vessels, the pancreas, or the posterior wall of the stomach. After creation of the gastric pouch, it is critical to verify the complete transection of the stomach to avoid communication between the pouch and the gastric remnant, and inspect the staple lines to ensure the hemostasis.
Creation of biliopancreatic and alimentary limbs
The greater omentum and the transverse colon are retracted cephalad to expose the ligament of Treitz and the inferior mesenteric vein (Fig. 4A). The jejunum is divided 60 cm (BMI <50 kg/m2) or 100 cm (BMI >50 kg/m2) distal to the ligament of Treitz using a white load linear stapler (Fig. 4B, C). The biliopancreatic limb is marked with a metallic clip to avoid an error when choosing the limb that needs to be sutured to the pouch (Fig. 4D). The alimentary limb is then raised with the stapler line orientated toward the left upper quadrant in an antecolic antegastric manner.
Creation of biliopancreatic and alimentary limbs.
Troubleshooting
When dividing the jejunum care must be taken not to undercut the biliopancreatic or Roux limb mesentery. The greater omentum is sometimes thick and bulky and prevents the adequate elevation of the alimentary limb. In this situation, the omentum should be divided vertically using the ultrasonic dissector to facilitate bringing the Roux limb up to the gastric pouch. Obtaining a tension-free alimentary limb is key to prevent complications of the anastomosis. In extreme cases, in which the division of the omentum is insufficient to release tension, the Roux limb should be placed in the retrocolic retrogastric position.
Gastrojejunostomy
A gastrostomy is performed with the ultrasonic scalpel at the distal end of the gastric pouch just under the staple line (Fig. 5A). An enterotomy is performed with the ultrasonic scalpel on the antimesenteric border of the alimentary limb 4–5 cm away from the stapled end (Fig. 5B). A side-to-side gastrojejunostomy is created with a blue load linear stapler. It is recommended to insert no more than 3 cm of the stapler to create a small anastomosis (Fig. 5C). The 36-Fr tube is passed through the anastomosis and the anterior wall is then closed with two layers of running suture using absorbable material (e.g., polyglactin 2.0) (Fig. 5D).

Gastrojejunostomy.
Troubleshooting
The 36-Fr tube is key to calibrate the anastomosis and to avoid suturing the posterior wall inadvertently. Whichever anastomosis technique is chosen, it is recommended to perform either a methylene blue test or a pneumohydraulic test to rule out leaks from the anastomosis.
Jejunojejunostomy
A 120 cm (BMI <50 kg/m2) or 150 cm (BMI >50 kg/m2) Roux limb is measured to determine the site of the anastomosis. The site chosen for the anastomosis is brought into apposition to the proximal jejunum with the stapled end of the biliopancreatic limb oriented toward the patient's right side and cephalad to the distal Roux limb. Enterotomies are performed using the harmonic scalpel at the antimesenteric border of both limbs (Fig. 6A). A white 60 mm linear stapler is inserted to its full length into both enterotomies to construct a side-to-side Jejunojejunostomy (Fig. 6B). The enterotomy is closed in one plane by running an absorbable suture (e.g., polyglactin 3.0) (Fig. 6C).
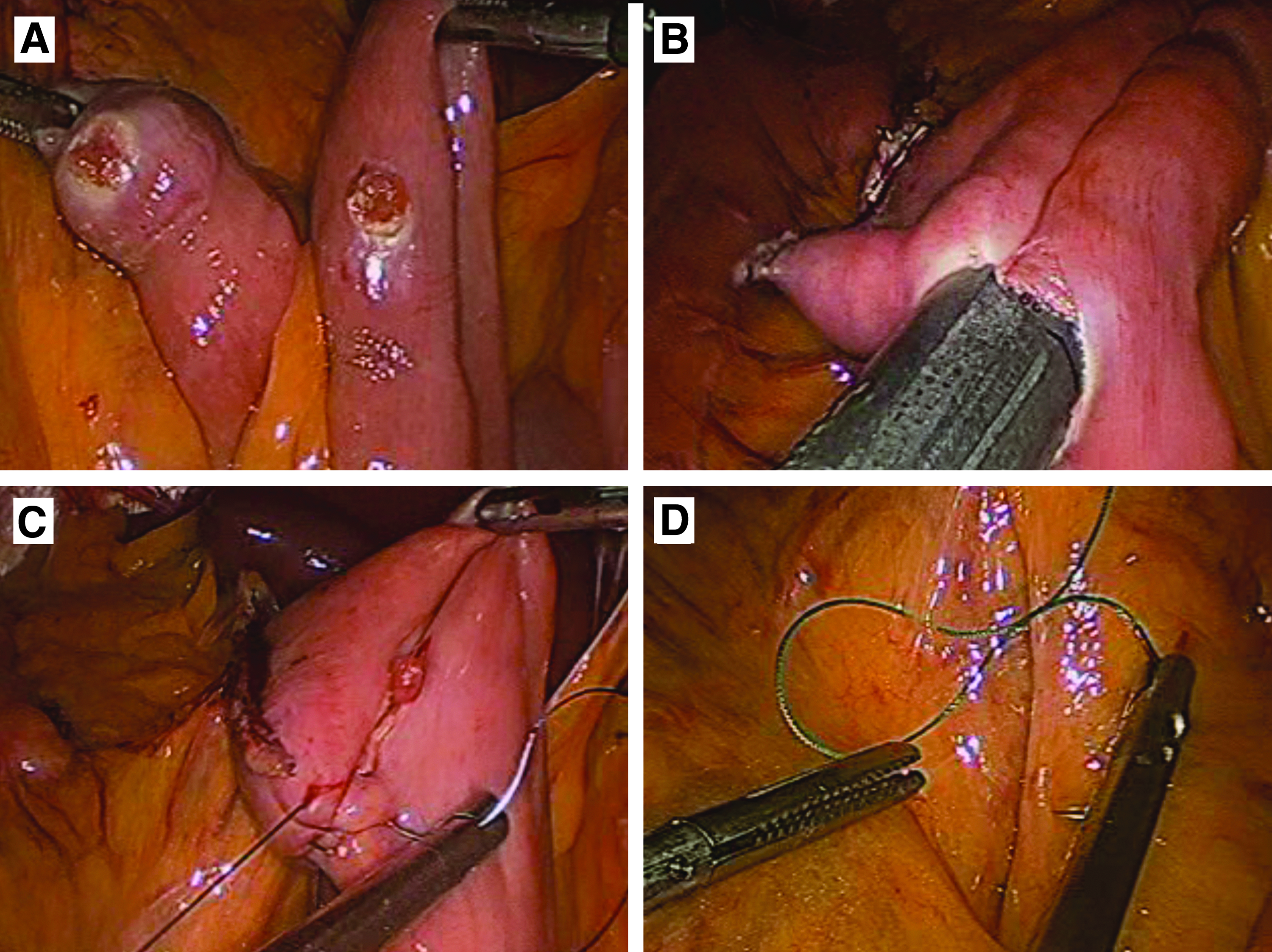
Jejunojejunostomy.
Troubleshooting
When performing this anastomosis, care should be taken to be certain that the mesenteries are properly aligned and no twists are present. If any area of separated serosa is noticed in the anastomosis, it should be approximated with Lembert sutures. An “anti-torsion” stitch between the two limbs of the bowel is useful to prevent future kinking of the anastomosis.
Closure of mesenteric and Petersen defect
The mesenteric defect is closed in a running, locking manner toward the root of the mesentery with nonabsorbable suture material (e.g., polyester 2.0) (Fig. 6D). The Petersen's space, limited posteriorly by the transverse colon and anteriorly by the alimentary limb, should be also closed with nonabsorbable suture material.
Troubleshooting
Internal hernias are the most frequent cause of reoperation after a laparoscopic RYGB. In addition, their management is complex because they can be difficult to identify. The closure of the mesenteric and Petersen defects is key to prevent this complication.
Conclusions
The laparoscopic RYGB remains the gold standard procedure for weight loss, and it is associated with excellent long-term outcomes. Its success relies on a careful patient selection, a comprehensive preoperative evaluation, and a properly executed operation that respects the key technical elements.
Footnotes
Disclosure Statement
No competing financial interests exist.